
Lecture 3 Dr. Janan Alrefaee
II. Tubular processing of the glomerular filtrate
Substance filtration rate = Glomerular filtration rate x substance plasma concentration.
Suppose that the substance is freely filtered and not bound to plasma proteins.
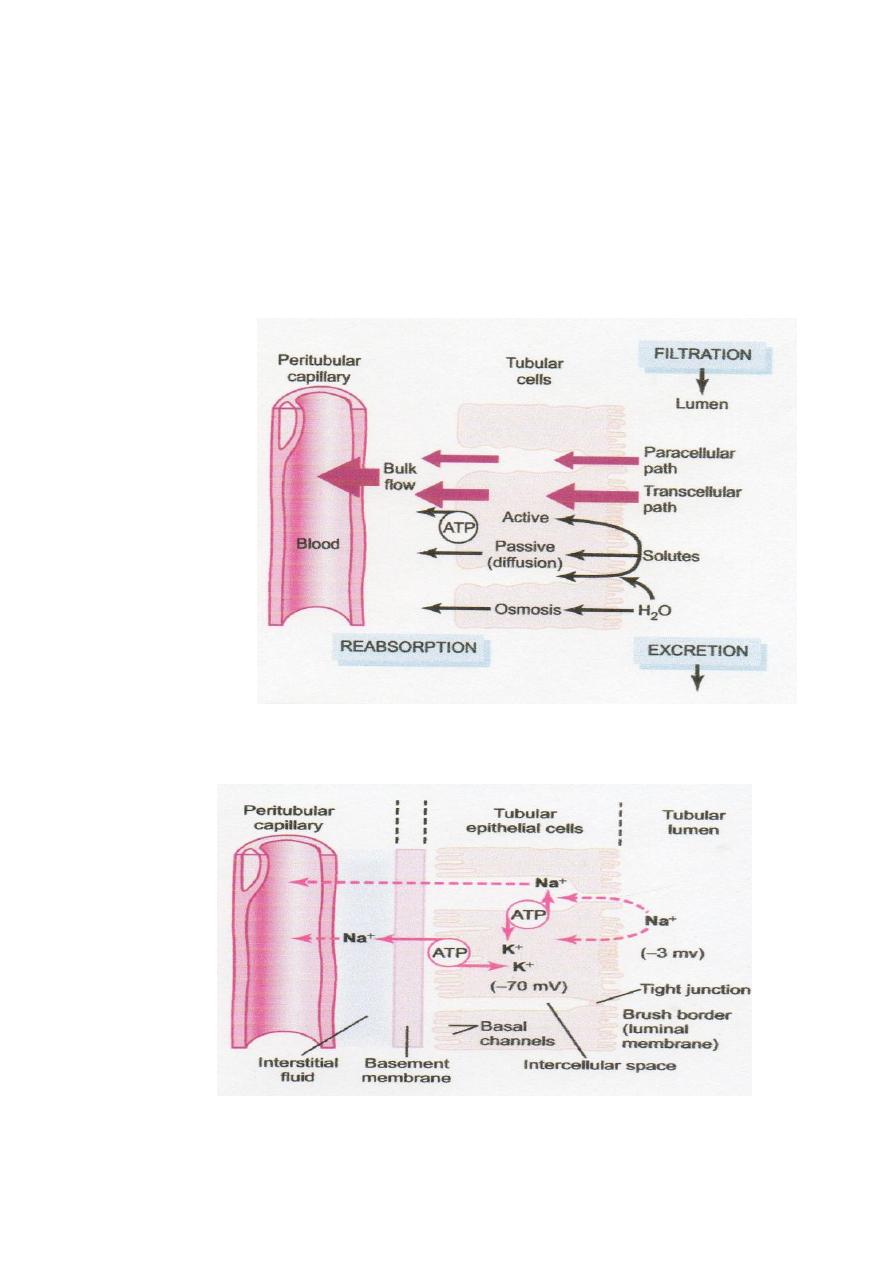
*The reabsorbed substance is transported across the tubular epithelial membranes (passive or
active transport) into the renal interstitial fluid, Water and solutes can be transported either
transcellular pathway or paracellular pathway (junctional space between cells) and then
through the peritubular capillary membrane to the blood by ultrafiltration (Fig. 3–1).
Active Transport: it is solute movement from low to high concentration and requires
energy. There are 2 types of active transport:
Primary active transport: its energy source directly from the hydrolysis of adenosine
triphosphate (ATP) by membrane-bound ATPase, ATPase also binds and moves solutes
across the cell membranes as the sodium-potassium ATPase pump.
A good example of a primary active transport system is the reabsorption of sodium ions
across the proximal tubular membrane; it involves the following steps (Fig.3.2).
1. Sodium is transported across the basolateral membrane from low concentration at the renal
tubular cell to high concentration at the interstitium by the sodium-potassium ATPase pump
and potassium is transported vice versa. This leading to 1-low intracellular sodium and high
intracellular potassium concentrations and 2- creates a net negative charge within cell. These
both reasons lead to:
2. Sodium passive diffuses (from high to low concentration) across the luminal membrane
into the renal tubular cell. The negative intracellular charge attracts the positive sodium ions
from the tubular lumen into the cell.
3. Sodium, water, and other substances are reabsorbed from the interstitial fluid into the
peritubular capillaries by ultrafiltration, a passive process driven by the hydrostatic and
colloid osmotic pressure gradients.
Secondary active transport: it utilizes energy indirectly from energy source (sodium-
potassium ATPase pump). when two or more substances combine with a carrier protein, as
one of the substances (e.g. sodium) diffuses to the low concentration in the cell, the energy
released from this transport is used to drive another substance (e.g. glucose
or amino acid)
from its low to high concentration (Fig. 3.3). Glucose and amino acids exit the cell across the
basolateral membranes by facilitated diffusion.

Secondary active secretion into the tubules: For e.g. Sodium-hydrogen counter-transport.
It happens when substances are secreted into the tubules (hydrogen) by secondary active
transport as counter-transport (opposite direction) with sodium (Fig. 3.3).
Pinocytosis: is an active transport for reabsorption of proteins, especially at the
the brush
border of
proximal tubule (invagination of protein into tubule cell and digested into amino
acids then reabsorbed).
Transport maximum: It is transport limit for the substances that are actively reabsorbed or
secreted by renal tubule occur when the tubular load of the substance exceeds the capacity
of the carrier proteins and specific enzymes involved in the transport process.
Filtered load of substance= GFR * plasma concentration of substance.
In the adult human, the transport maximum for glucose averages about 375 mg/min. With
the filtered load of glucose above 375 mg/min (uncontrolled diabetes mellitus), the excess
glucose filtered is not reabsorbed and passes into the urine. However, when the plasma
concentration of glucose rises above 200 mg/100 ml (the filtered load= 250 mg/min when
GFR=125 ml/min), a small amount of glucose begins to appear in the urine, this called the
threshold for glucose. The reason is that not all nephrons have the same transport maximum
for glucose and 375 mg/min is the transport maximum for the kidneys is reached when all
nephrons have reached their transport maximum for glucose.
Other passive and some active reabsorbed substances (as sodium) do not have a transport
maximum because their transport is determined by gradient-time transport.
Water is reabsorbed passively by osmosis (passive) but this can occur only if the tubular
membrane is permeable to water.
Reabsorption of chloride, urea, and other solutes by passive diffusion
Chloride (negative charge) is reabsorbed passively due to 1-electrical potentials: the
transport of sodium (positive charge) leaves the lumen negatively charged compared with the
interstitial fluid. This causes chloride ions to diffuse passively through the paracellular
pathway.
2-concentration gradient: after water osmosis, the chloride concentrates in the tubular
lumen (Fig. 3.4).
3- by secondary active transport as co-transport of chloride with sodium across the luminal
membrane.
Urea is passively reabsorbed from the tubule due to concentration gradient after water
osmosis (Fig. 3.4). Urea reabsorption is facilitated by specific urea transporters in some
parts of the nephron, especially the inner medullary collecting duct; one of urea transporters
is activated by ADH. About one half of the filtered urea is reabsorbed & the rest passes into
the urine.
Creatinine is larger molecule; almost all the creatinine filtered is not reabsorbed but
excreted in the urine.
Figure 3.1 Reabsorption of filtered water and solutes from the tubular lumen
Figure 3.2 Basic mechanism for active transport of sodium through the tubular
epithelial cell
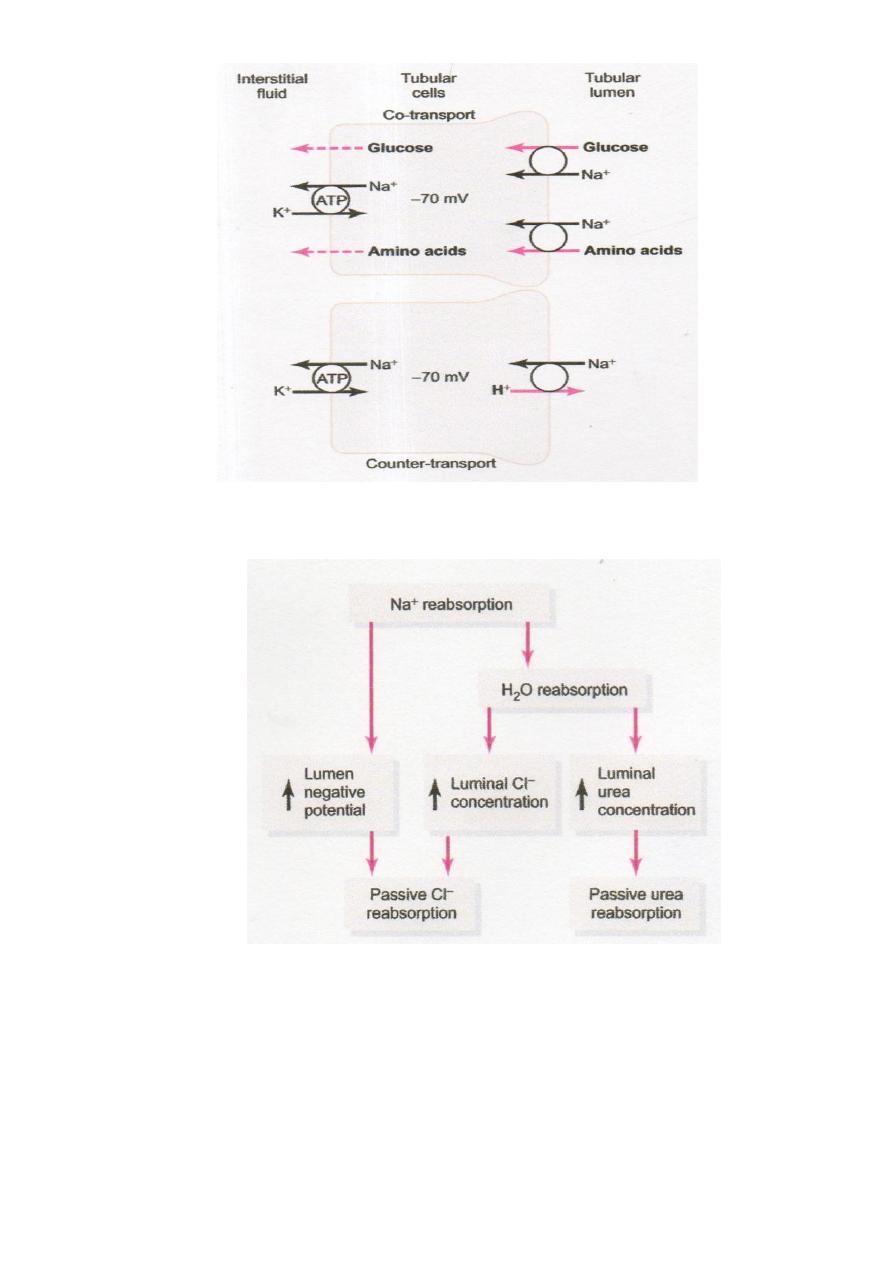
Figure 3.3 Mechanisms of secondary active transport
Figure 3.4 Mechanisms by which water, chloride, and urea reabsorption are coupled
with sodium reabsorption