ORTHO – PERIO PROBLEMS
Orthodontic treatment involves the use and control of forces acting upon the teeth . During tooth movement, the tooth supporting tissues (ie, gingiva, periodontal ligament, alveolar bone) usually exhibit favorable responses. However ,some clinical, radiographic, and histologic investigations have indicated that such forces may cause damage not only to the root substance, but also to the bone-supporting tissuesFood debris and plaque represent a risk factor for gingival inflammation, which can be reduced or eliminated by better oral hygiene and by fluorides. Orthodontic treatment can also have an adverse effect upon the periodontal tissues ( eg .gingival recession, marginal bone loss, infrabony pockets) depending on the magnitude, direction and duration of force applied and the age of the treated patient.

Adverse Effect on Gingival Tissues
Bacterial plaque at the gingival margin is the initiating and most significant factor in gingival inflammation. Patients undergoing orthodontic treatment have increased retention sites for microbial samples, which may be responsible for gingivitis.
Higher plaque indices ,bleeding tendencies and pocket depths have been observed for molars with orthodontic bands than for bonded brackets.
Loss of attachment was also more common for molars with orthodontic bands which can be due to the difficulty in plaque removal on the gingival margin of the bands or due to mechanical injury caused by the placement of the band too deep within the gingival pocket.
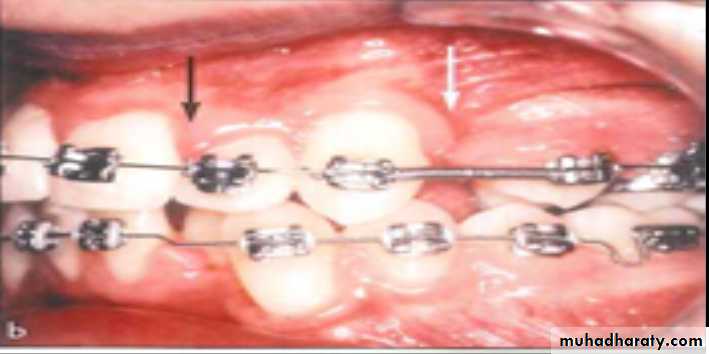

Orthodontic closure of extraction sites often results in compressed gingival tissue with an interdental fold most frequently at the buccal aspect of the maxillary first molar extraction site or at the mandibular first molar extraction site
A proper oral hygiene regimen in patients with fixed orthodontic appliances (especially around molar band) prevent plaque accumulation, bleeding tendency, and loss of attachment. The use of light forces in closing extraction space will minimize compression of the gingival tissue with interdental folds, which may be responsible for relapse after closure of the gap.
Loss of Marginal Bone Support
Orthodontic appliances have the potential to damage the periodontal support of the treated teeth which may show a slightly larger distance between CEJ and the alveolar crest than untreated teeth especially with patients who had difficulties with the oral hygiene regimen during the treatment. This indicates that orthodontic treatment can aggravate a pre-existing plaque- indused gingival lesion, which may cause loss of alveolar bone and periodontal attachment.
In the absence of plaque , orthodontic force and tooth movement fail to induce gingivitis. In the presence of plaque, similar forces may cause marginal bone loss.
Adverse Effect of Labial/ Buccal Tooth Movements
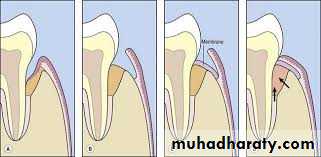
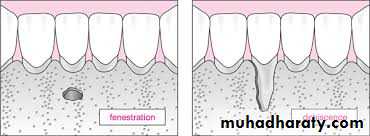
Labial and buccal tooth movement displace the root toward, and sometimes through the cortical plate. If more toque is incorporated into the archwire, the magnitude of force is increased and the apex may be displaced through the cortical bone, resulting in a fenestrationContrary to the bone fenestration, which is localized in the apical part of the root , A bone dehiscence involves marginal bone loss at the labial / buccal aspects of the root
Marginal bone recession displacement of the soft tissue margin apical to CEJ with exposure of the root surface, is a common feature in individuals who have not undergo orthodontic treatment. Such recessions are also observed in association with orthodontic therapy, for example , after alignment of crowded teeth .This type of recession may be associated with localized plaque- induced inflammatory lesions.

As long as the tooth can be moved within the envelop of the alveolar process, risk of development of harmful side effects in the marginal tissue is minimal regardless of the dimension and quality of the soft tissue. If the tooth movement result in an alveolar bone dehiscence, it must be stressed that no bone regeneration occur, even after a long period of retention. The volume (thickness) of the soft tissue cover should be considered as a factor that may cause a soft tissue recession to develop during or after active orthodontic treatment.
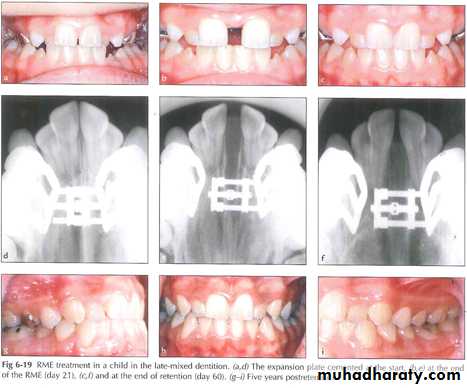
RMT Treatment in Posterior Skeletal Crossbite
There are two types of posterior crossbite: the dentoalveolar crossbite (palatally inclined maxillary teeth) and the skeletal crossbite ( narrower dimension in the maxilla than mandible). In the skeletal crossbite tipping of the premolars and molars may result in bone dehiscence and and gingival recession ;therefore ,rapid maxillary expansion (RME) .An activation force above the recommended value (1-1.5 mm) per activation will result into overrotation of the mesiobuccal root, which may cause marginal recession which can be exposed many years after treatment has been completed and generally required a soft tissue graft for root coverage. The primary indications for root coverage procedures are esthetic demands, root hypersensitivity, and management of shallow root caries lesions and cervical abrasions.
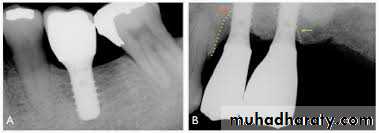
Potential Problems with Implants in Adolescent Patients
In orthodontic- prosthodontic treatment , implants serve as orthodontic anchorage units and then as abutments for prosthetic reconstructions of missing teeth in adults. In regular orthodontic treatment, the anchorage units must be placed in regions other than the alveolar bone , such as the palate. Because of the thin bone height in the palate , an endosseous implant must have small dimensions, especially in the length, so as not to perforate the nasal cavity. Another disadvantage of palatal implants is that they must be removed after the completion of orthodontic treatment with the risk of bony defects or soft tissue damageConclusions
The following facts deserve attention in the orthodontic patients to avoid /minimize damage to tooth supporting tissue in orthodontics:
1- A proper oral hygiene regimen during the total treatment period is required to prevent plaque accumulation and thus minimize the risk for gingivitis , attachment loss, infrabony pockets and loss of the marginal alveolar bone.
2- the use of light orthodontic forces in closure of extraction sites will minimize the formation of interdental folds which may cause relapse after closure of the extraction space.
3- Labial and buccal tooth movements should be preceded by careful examination of the tissue covering the labial /buccal aspect of these teeth. During such movements , the roots are displaced toward and sometimes even through the thin cortical bone plate, which may result in fenestration and dehiscence. Torque tooth movements and rapid maxillary expansion ( in patient with partially or totally obliterated sutures ) heightens the risk of such complications.