Retention in orthodontics
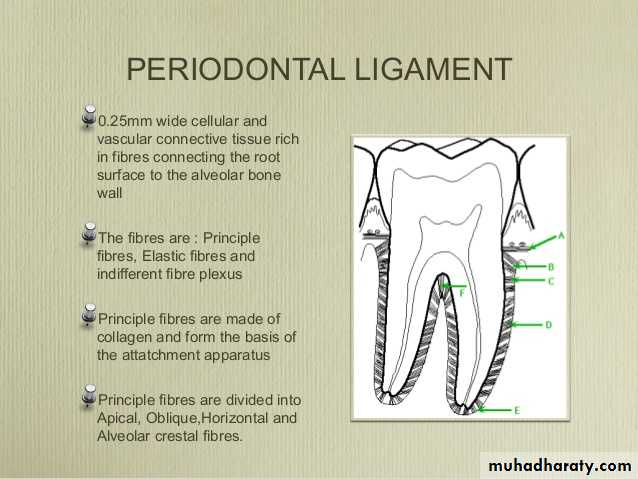
General Factors affecting retentionthe involvement of the periodontal ligament fibers and gingival fibers
late mandibular growth
physiologic imbalance of local extrinsic forces acting on the corrected dentition such as:
- occlusion
- tongue musculature
- cheek musculature
- gingival fibers
- fibers of the PDL
Correction of deep overbite
Following the correction of a very deep overbite, the use of an anterior biteplane until the completion of facial growth has been recommended. This may be particularly useful when there is evidence of an anterior mandibular growth rotation
Correction of anterior open bites
While the use of retainers incorporating posterior bite blocks has been recommended for prolonged retention of anterior open bite malocclusions with unfavorable growth patterns, there is currently a lack of scientific evidence to support this.
Patients with a history of periodontal disease or root resorption
In patients with previously treated severe periodontal disease, permanent retention is advised. For those with minimum to moderate disease, a more routine retention protocol can be used. There is evidence of an increased risk of deterioration of lower incisor alignment post-retention in cases with root resorption or crestal bone loss. These cases may therefore benefit from prolonged retention.
Growth modification treatment
Following the use of headgear or functional appliances, retention using a modified activator appliance has been reported as effective in maintaining Class II correction. However, no comparative studies have confirmed the usefulness of this form of retention.
Correction of posterior and anterior crossbites
When the incisor overbite and posterior intercuspation are adequate for maintaining the correction, no retention is necessary. However, for most of the case a retention of 3-6 months should be conducted

Adult Patients
When the periodontal supporting tissues are normal and no occlusal settling is required, there is no evidence to support any changes in retention protocol for adult patients compared with adolescent patients.
Spaced dentitions
Permanent retention has been recommended following orthodontic treatment to close generalised spacing or a midline diastema in an otherwise normal occlusion

Retainer Design
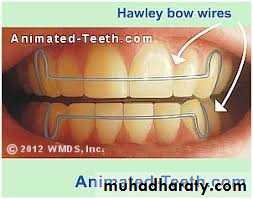
Removable retainers with a labial bow (Hawley retainers)
These retainers can be worn full day but not during eating. Hawley retainers and labial bow can be used to accomplish simple tooth movements if required, and an anterior biteplane can easily be incorporated for retention of a corrected deep overbite.
Removable vacuum formed retainers
Vacuum formed retainers are relatively inexpensive and can be quickly fabricated on the same day as appliance removal. Full posterior occlusal coverage (including second molars if present) is advisable in order to reduce the risk of overeruption of these teeth during retention. Vacuum retainers were significantly less effective in promoting posterior occlusal settling than Hawley retainers. However this is likely to be of little importance if good posterior intercuspation has been established by the time of debonding.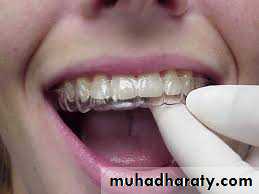
Fixed bonded retainers Smooth wire, Flexible spiralwire
Fixed retainers are indicated for long-term retention of the labial segments, particularly when there is reduced periodontal support, and for retention of a midline diastema. Fixed retainers are discreet and reduce the demands on patient compliance. However they are associated with failure rates of up to 47%, particularly on upper incisors when there is a deep overbite. In addition, calculus and plaque deposition is greater than with removable retainers. Fixed retainers therefore require long term maintenance.

Flexible spiral wire retainers allow differential tooth movement and are particularly useful for patients with loss of periodontal support. Current orthodontic opinion recommends either the use of 0.0215 inch multistrand wire, or 0.030 - 0.032 inch sandblasted round stainless steel wire.
