
Psychiatry
Lecture 24: Sexuality
Psychological sexual development
Gender identity: Sense of self as being male or female.
Gender role: Expression of one's gender identity in society.
Sexual orientation: Persistent and unchanging preference for people of the
same sex (homosexual) or the opposite sex (heterosexual) for love and sexual expression.
True bisexuality is uncommon; most people have a sexual preference. Homosexuality is
considered a normal variant of sexual expression.
Gender Identity Disorder
Individuals with gender identity disorder (transsexual or transgender individuals) have
a pervasive psychological feeling of being born into the body of the wrong sex despite a
body form normal for their physiological sex.
School-age children with gender identity disorder prefer to dress like and have
playmates of the opposite sex.
Since gender identity is permanent, the most effective management of this situation is to
help parents accept the child as he or she is.
In
adulthood, these individuals commonly take the hormones of their preferred sex and
may seek sex-change surgery.
THE BIOLOGY OF SEXUALITY IN ADULTS
In adults, alterations in circulating levels of gonadal hormones (estrogen, progesterone, and
testosterone) can affect sexual interest and expression.
Hormones and behavior in women
Because estrogen is only minimally involved in libido, menopause (i.e., cessation of
ovarian estrogen production) and aging do not reduce sex drive if a woman's general
health is good.
Testosterone is secreted by the adrenal glands (as well as the ovaries and testes)
throughout adult life and is believed to play an important role in sex drive in both men
and women.
Hormones and behavior in men
Testosterone levels in men generally are higher than necessary to maintain normal
sexual functioning; low testosterone levels are less likely than relationship problems,
age, alcohol use, or unidentified illness to cause sexual dysfunction.
Psychological and physical stress may decrease testosterone levels. Medical treatment with
estrogens, progesterone, or antiandrogens (e.g., to treat prostate cancer) can decrease
testosterone availability via hypothalamic feedback mechanisms, resulting in decreased sexual
interest and behavior.
Homosexuality (i.e., gay or lesbian sexual orientation)
The etiology of homosexuality is believed to be related to alterations in levels of
prenatal sex hormones (e.g., increased androgens in females and decreased androgens
in males) resulting in anatomic changes in some levels in adulthood are
indistinguishable from those of heterosexual people of the same biological sex.
Evidence for involvement of genetic factors includes markers on the X chromosome and
higher concordance rate in monozygotic than in dizygotic twins.
Social factors, such as early sexual experiences, are not associated
.
with the etiology of
homosexuality.
Homosexuality is a normal variant of sexual expression. Because it is not a dysfunction,
no treatment is needed.
People who are uncomfortable with their sexual orientation may benefit from
psychological intervention to help them become more comfortable.
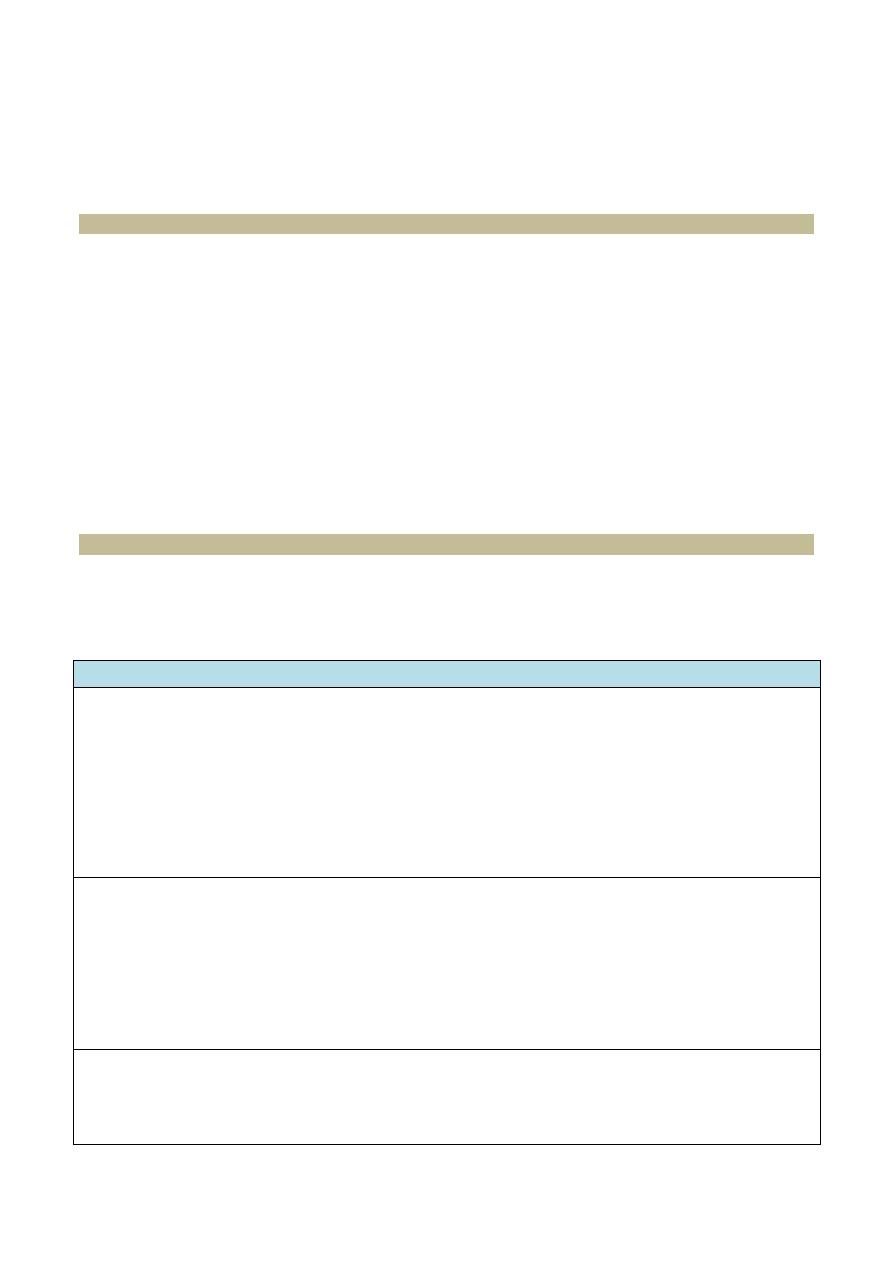
The sexual response cycle
Masters and Johnson devised a four-stage model for sexual response in both men and women,
including the excitement, plateau, orgasm, and resolution stages (see the table below),
Sexual dysfunctions involve difficulty with one or more aspects of the sexual response cycle.
Stages of the sexual response cycle
EXCITEMENT
• Penile and clitoral erection
• Labial swelling
• Vaginal lubrication (watery exudate caused by vasocongestion)
• Tenting effect (rising of the uterus in the pelvic cavity)
• Nipple erection (both sexes)
• Increased pulse, blood pressure, and· respiration (both sexes)
• Problems in this stage are associated with female sexual arousal disorder and male erectile
disorder
PLATEAU
• Increased size and upward movement of the testes
• Secretion of a few drops of sperm-containing fluid
• Flushing of the chest and face (both sexes) .
• Contraction of the outer third of the vagina, forming the orgasmic platform (enlargement of the
upper third of the vagina)
• Further increase in pulse, blood pressure, and respiration (both sexes)
• Absence of this stage is associated with premature ejaculation
ORGASM
• Forcible expulsion of seminal fluid
• Contractions of the uterus and vagina
• Contractions of the anal sphincter (both sexes)
• Further increase in pulse, blood pressure, and respiration (both sexes)
• Problems in this stage are associated with male and female orgasm disorder
RESOLUTION
• Muscle relaxation
• In men, a refractory, or resting period (length varies by age and physical condition) when
restimulation is not possible; little or no refractory period in women
• Return of the sexual, muscular, and card7iovascular systems to the prestimulated state over 10- 15
min
SEXUAL DYSFUNCTION
Characteristics
Sexual dysfunction can result from biological, psychological, or interpersonal causes, or
from a combination of causes.
Biological causes include an unidentified general medical condition (e.g., diabetes can
cause erectile dysfunction; pelvic adhesions can cause dyspareunia), side e ffects of
medication (e.g., selective serotonin reuptake inhibitors [SSRIs] can cause delayed
orgasm), substance abuse (e.g., alcohol use can cause erectile dysfunction), and
hormonal or neurotransmitter alterations.
Psychological causes include current relationship problems, stress, depression, and
anxiety (e.g., guilt, performance pressure).
In men with erectile disorder, the presence of morning e rections, erections during
masturbation, or erections during rapid eye movement (REM) sleep suggests a
psychological rather than a physical cause.
Dysfunctions may always have been present (primary sexual dysfunctions), or, more
commonly, they occur after an interval when function has been normal (secondary
sexual dysfunctions).
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text
Revision (DSM-IV-TR) classifications of sexual dysfunctions
1- The sexual desire disorders are hypoactive sexual desire disorder and sexual
aversion disorder (disorders of the excitement phase).
2- The sexual arousal disorders are female sexual arousal disorder and male erectile
disorder (disorders of the excitement and plateau phases).
3- The orgasmic disorders are male orgasmic disorder, female orgasmic disorder, and
premature e jaculation (disorders
of the orgasm phase).
4-
The sexual pain disorders are dyspareunia and vaginismus (not caused by a general
medical condition).
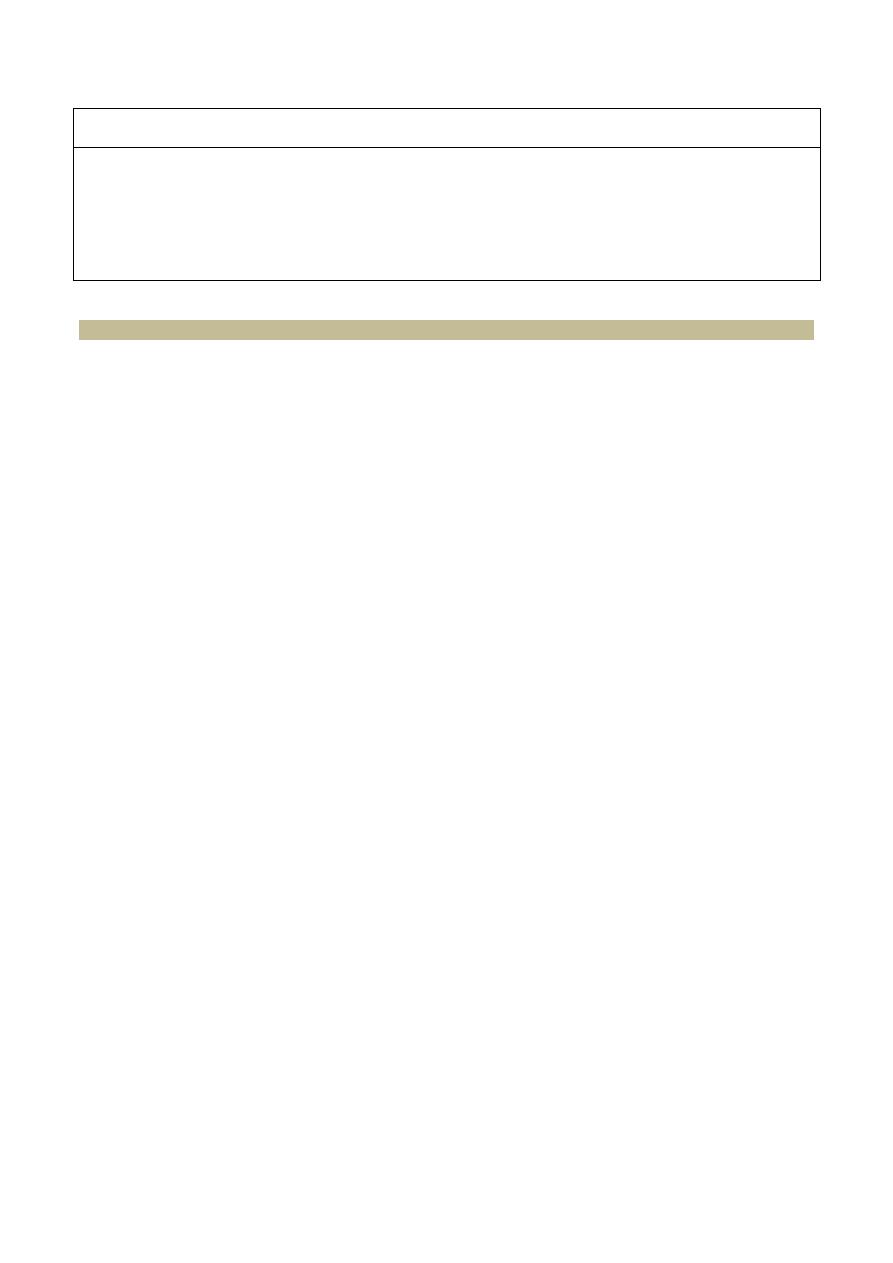
Characteristics of the sexual dysfunctions (see the table below)
Disorder
Characteristics
Hypoactive sexual desire disorder
Decreased interest
in sexual activity
•
May
be
normal
individual
variation
in desire
Sexual aversion disorder
Aversion
to
and
avoidance of sexual activity
Female
sexual arousal disorder
•
Inability to maintain vaginal lubrication until the sex
act
is comp
l
eted
despite
adequate physical
s
timulation
•
Reported in as many as
20%
of women
Male erectile disorder
(commonly called
"impotence")
Lifelong
or primary (rare):
Has never had
an erection
sufficient
for
penetration
•
Acquired or
secondary (the
most
common of all
male
sexual
disorders): Current inability to maintain
erections despite
normal erections
in
the past
•
Situational
(common):
Difficulty maintaining
erections
in
some situations,
but not others
•
In men
with erectile
disorder
,
the
presence of
morning erections
,
erections during masturbation
,
or
erections
during rapid
eye
movement
sleep suggests a
psychologicai
rather
than
a
physical
cause
Orgasm disorder (male
and
female)
Lifelong: No previous
orgasm
•
Acquired:
Current
inability to
achieve orgasm despite
adequate
genital
stimu
l
ation
(normal
orgasms in
the
past)
•
Reported in more women than men
Premature
ejaculation
Ejaculation before
the
man
would
li
ke
it
to occur
•
Short or absent
plateau phase
of
the
sexual response
cycle
•
Usually
accompanied
by anxiety
•
Second
most
common of all
male
sexua
l
disorders
Vaginismus
Pa
inful spasm
of the outer third of the vagina
• Makes
intercourse
·
or pelvic examination difficult
Dyspareunia
Persistent pain associated with
sexual
interc
o
urse
•
Much more
common
in
women; can occur
in men
Treatment of sexual dysfunction
1- The physician must understand the patient's sexual problem before proceeding with
treatment (e.g., clarify what a patient means when he says, "I have a problem with sex.").
2- The physician should not assume anything about a patient's sexuality (e.g., a middle-aged
married male patient may be having an extramarital homosexual relationship).
3- There is a growing tendency for physicians to treat the sexual problems of heterosexual and
homosexual patients rather than to refer these patients to sex therapists.
4-
Treatment of sexual problems may be behavioral, medical, or surgical.
Behavioral treatment techniques
1. In sensate-focus exercises (used to treat sexual desire, arousal, and orgasmic disorders),
the individual's awareness of touch, sight, smell, and sound stimuli are increased during
sexual activity, and psychological pressure to achieve an erection or orgasm is
decreased.
2. In the squeeze technique, which is used to treat premature e jaculation, the man is taught
to identify the sensation that occurs just before the emission of semen. At this moment,
the man asks his partner to exert pressure on the coronal ridge of the glans on both
sides of the penis until the erection subsides, thereby delaying ejaculation.
3. Relaxation techniques, hypnosis, and systematic desensitization are used to reduce
anxiety associated with sexual performance.
4. Masturbation may be recommended to help the person learn what stimuli are most
effective for achieving arousal and orgasm.
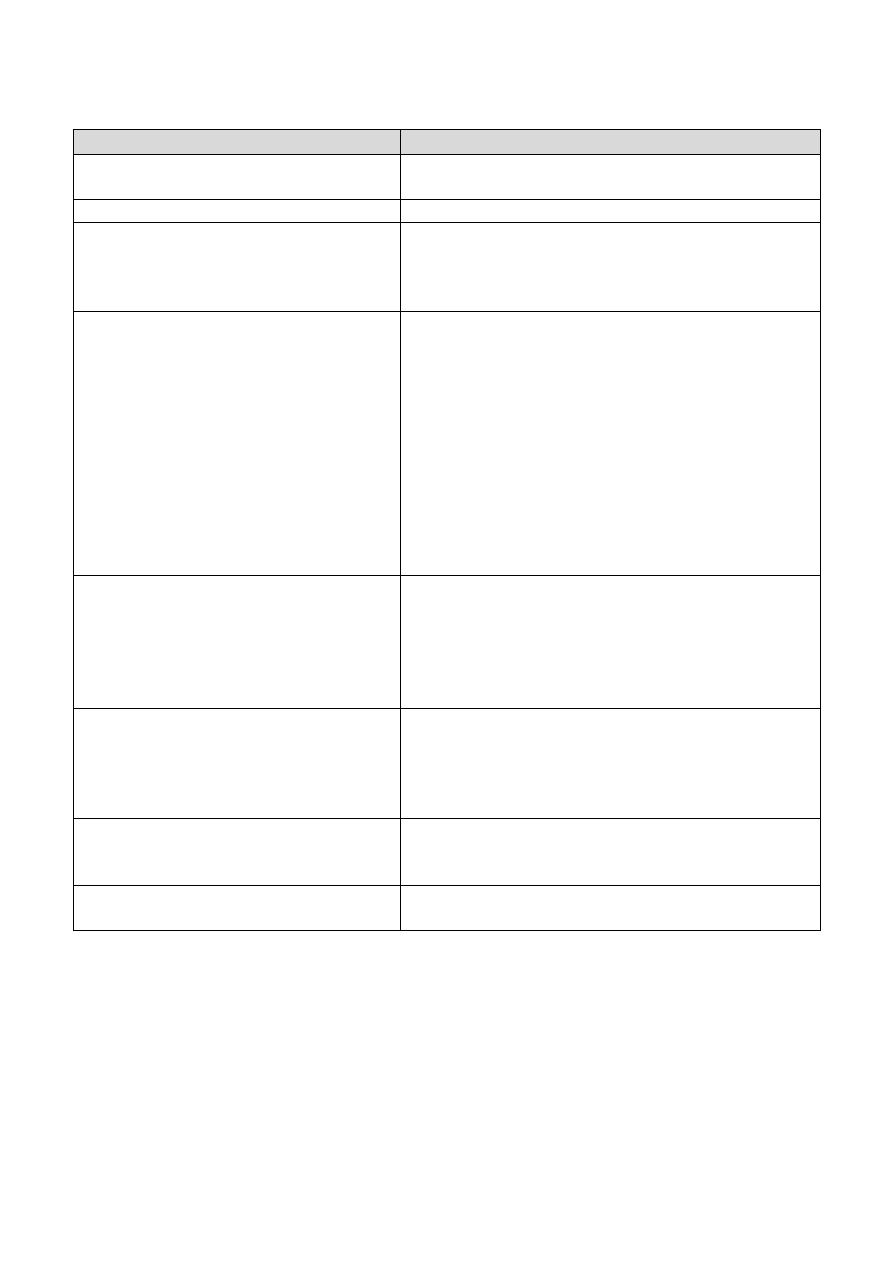
PARAPHILIAS
Definition
Paraphilias involve the preferential use of unusual objects of sexual desire or engagement in
unusual sexual activity (see the table below). To fit
DSM-IV-TR criteria, the behavior must
continue over a period of at least 6 months and cause impairment in occupational or social
functioning.
Occurrence and treatment
Paraphilias
occur almost exclusively in men.
Pharmacologic treatment includes antiandrogens and female sex hormones for paraphilias that
are characterized by hypersexuality.
Paraphilia
Sexual gratification obtained by
Exibitionism
Revealing one's genitals to unsuspecting women
•
Shocking unsuspecting women
F
etishism
Contact with certain inanimate objects, such as shoes or rubber sheets
•
In transvestic fetishism (exclusive to heterosexual men), wearing women's
clothing,
particularly underclothing
Frotteurism
Rubbing the penis against a
clothed
woman
•
The woman is not consenting and not aware
Pedophilia
Engaging in fantasies or actual behaviors with
children
under age 14 years,of the
opposite or same
sex
•
The pedophile must be at least 16 years
of age and
4 or 5
years older
than the
victim
•
Most common paraphilia
Sexual masochism
Receiving physical paih
•
Being humiliated
Sexual sadism
Giving physical pain or humiliation
Voyeurism
Secretly watching other people (often with binoculars) undressing or
engaging in sexual activity
The End