Risk factors associated with etiology of periodontal diseases
Dr. Hussein Al dabbagh
In recent years, it has become apparent that the pathogenesis of periodontal diseases is more complex than the presence of virulent microorganisms. In fact, periodontitis is defined as an inflammatory disease of bacterial origin begin with the accumulation of biofilms on the tooth surface which is called dental plaque, in addition to dental plaque, some of the host factors has been considered as risk factors that associated with increased severity of periodontal diseases.
Introduction

Risk
is the probability that an individual will develop specific disease over specific period of time.
The risk of developing the disease varies from individual to individual.
Risk factors may be environmental, behavioral, or biologic factors.
Risk predicts the progression from health to severe periodontitisHealth
Initialdisease stage
Gingivitis
Mild periodontitis
Moderate periodontitis
Severe periodontitis

• Risk factors
• The characteristic of individuals that put them at increased risk for getting a disease.
Modifiable
• Dental plaque• Smoking.
• Diabetes mellitus.
• Specific Pathogenic bacteria and Microbial tooth deposits.
• Risk determinants \non modifaible
• which is sometimes substituted for
• the term risk factor, should be reserved
• for those risk factors that cannot be modified.
• Genetic factors
• Age
• Gender
• Stress

1-Tobacco smoking
Tobacco smoking is a well-established risk factor for periodontitis. A direct relationship exists between smoking and the prevalence of periodontal disease.Severity is directly related to both –the number of cigarettes
smoked per day- the numbers of years a patient has been smoking.
In a study on subjects with different smoking histories, it was found that smokers had significantly higher levels of Tannerella forsythia(2.3 times) more likely than nonsmokers and former smokers. Of particular interest was the observation that smokers do not respond to mechanical therapy as well as nonsmokers; this is associated with increased levels of T. forsythia, A. actinomycetemcomitans, and P. gingivalis remaining in the pockets after therapy in the smoking group with greater post treatment probing depth and less gain in clinical attachment levels when compared with nonsmokers.

Microbiology No effect on rate of plaque accumulation.
↑ Colonization of shallow periodontal pockets by periodontalpathogens.
↑ Levels of periodontal pathogens in deep periodontal pockets.
Immune-inflammatory
Response
*Altered neutrophil chemotaxis, phagocytosis.
*# reduction in the production of antibodies essential for killing the bacteria specially IgG2
physiological effect of smoking on the etiology of periodontal disease include of following:
Decrease of gingival blood vessels and reduce bleeding on probing with increase severity of inflammation (vasoconstriction).
Decrease gingival crevicular fluid flow.
.

Effects of Smoking on the Prevalence and Severity ofPeriodontal Diseases
Gingivitis ↓ bleeding on
probing.Periodontitis ↑ Prevalence and severity of periodontitis.
↑ Pocket depth, attachment loss, and bone loss.
↑ Rate of periodontal destruction.
↑ Prevalence of severe periodontitis.
↑ Tooth loss.
↑ Prevalence with increased number of
cigarettes smoked per day.
↓ Prevalence and severity with smoking
cessation.





Effect of smoking on periodontal therapy
Nonsurgical ↓ Clinical response to root surface debridement.↓ Reduction in pocket depth.
↓ Gain in clinical attachment levels.
Surgery and implants↓ Pocket depth reduction.
↓ gain in clinical attachment .↑ Deterioration of furcation after surgery.
↓ Gain in clinical attachment levels, ↓ bone fill
↑ recession.
↑ membrane exposure after GTR.
↓ Pocket depth reduction after bone graft . procedures.
↑ Risk for implant failure and periimplantitis.
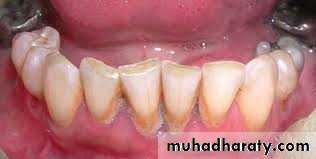
2-Diabetes Mellitus
Diabetes is a clear risk factor for periodontitis.Epidemiologic data demonstrate that the prevalence and severity of periodontitis is significantly higher in patients with type I and type II diabetes than in those without diabetes and that the level of diabetic control is an important variable in relationship with the pathogenesis.

The influence of diabetes on the periodontium has been thoroughly investigated. variety of changes have been described, including a tendency toward enlarged gingiva, sessile or pedunculated gingival polyps, abscess formation, periodontitis, and loosened teeth.
Perhaps the most striking changes in uncontrolled diabetes are the reduction in defense mechanisms and the increased susceptibility to infections, leading to destructive periodontal disease.
the periodontal problems in diabetic patients with poor oral hygiene are:-
1-Severe gingival inflammation,
2-deep periodontal pockets.
3-rapid bone loss.
4-frequent periodontal abscesses.






3-Pathogenic bacteria and microbial tooth deposits
Several studies demonstrate a causal relationship between accumulation of bacterial plaque and gingival inflammation.Often, patients with severe attachment loss have
minimal levels of bacterial plaque on the affected teeth,indicating that the quantity of plaque is not of major importance in the disease process.
although quantity may not indicate risk, there is evidence that the composition, or quality of the complex plaque biofilm is of importance.

• specific bacteria have been identified as etiologic agents for periodontitis:
• 1. A. actinomycetemcomitans --- aggressive• periodontitis.
• 2. Porphyromonas gingivalis --- chronic
• 3. Tannerella forsythia periodontitis.

Obesity
Obesity has been postulated to reduce blood flow to the periodontal tissue, promoting the development of periodontal disease. Furthermore, obesity may enhance immunological or inflammatory disorders, which might be the reason obese subjects tend to exhibit poor periodontal status relative to non-obese individuals.-genetic factors
There is evidence that genetic differences between individuals may explain why some patients develop periodontal disease and others do not.The familial aggregation seen in localized and generalized aggressive periodontitis also is indicative of genetic involvement in these diseases. Tannerella


Ex….
A specific (IL-1) genotype has been associated with severe chronic periodontitis.Immunologic alterations, such as
neutrophil abnormalities, monocytic hyper responsiveness to lipopolysaccharide stimulation in patients with localized aggressive periodontitis.Pregnancy associated gingivitis is inflammation of the gingival tissues associated with pregnancy. This condition is accompanied by increase in steroid hormones in crevicular fluid and increase in levels of (Prevotella intermedia microorganism) which use the steroids as growth factors. The increase in sex hormones may exaggerate the inflammatory response to dental plaque which means small amount of plaque may lead to gingivitis. Puberty is also accompanied by an exaggerated response of gingiva to local irritation.
-Age
Both the prevalence and severity of periodontal disease increases with age .It is possible that
1. degenerative changes related to aging may increase susceptibility to periodontitis.2. the attachment loss and bone loss seen in older individuals is a result of prolonged exposure to other risk factors over a person's life, creating a cumulative effect over time.

Changes that take place with
aging:Arteriosclerosis (reduction in arterial blood supply).
The gingiva become more fibrotic and less keratinized.The periodontal fiber bundles become thicker with decrease in cellularity.
Osteoporosis of alveolar bone..

Medications:
Gingival enlargement is a well-known consequence of the administration of some drugs as anticonvulsants ( phenytoin or Dilantin) , immunosuppressants ( cyclosporine) ,and Ca channel blockers (nifedipine).in general the over growth of the gingiva start as painless enlargement of the interdental papilla and extend to the marginal gingiva , then as the condition progress , the marginal and papillary enlargement unite together and may cover the clinical crown and may interfere with the occlusion.
Duration & dose.
The first drug induced gingival enlargement is Phenytoin (Dilantin Na) which is anticonvulsant drug used in the treatment of epilepsy. Gingival enlargement occur in 50-65% of patients receiving the drug.
The other drug is Cyclosporine A which is immunosuppressive agent used to prevent organ transplant rejection. The enlargement occurs in 30% of patients receiving this drug.
Ca channel blockers are drug used for the treatment of cardio-vascular conditions such as hypertension and angina pectoris. Some of these drugs can induce gingival enlargement. Nifedipine is one of most commonly used drug that induced the enlargement in about 20% of the patients. More recent are Amlodipine and Verapamil which also induced enlargement.


• (1) males have more loss of attachment than Females.
• (2) males have poorer oral hygiene than females.• So higher levels of plaque and calculus lead to gender differences in prevalence and severity of periodontitis that related to preventive practices rather than any genetic factor.
Gender

-Socioeconomic & education Status
• Gingivitis and poor oral hygiene can be related to lower
• socioeconomic status:
1) decreased dental awareness.
• 2) decreased frequency of dental visits.
• when compared with more educated individuals of higher SES.
• After adjusting for other risk factors such as smoking and poor oral hygiene lower SES alone does not result in increased risk for periodontitis.
-Stress
The incidence of necrotizing ulcerative gingivitis increases during periods of emotional and physiologic stress, suggesting a linkBetween them.
Emotional stress may :
1) interfere with normal immune function.
2) result in increased levels of circulating hormones
that can have an impact on the periodontium.

.
Individuals with financial strain, distress, depression, or inadequate coping mechanisms have more severe loss of attachment.
The local anatomic risk factors: include
Furcation anatomy: the entrance of bifurcations or trifurcations is restricted enough to limit the access for mechanical root instrumentation. Also the presence of concavities in the furcal aspects of molar will limit instrumentation as well.Cervical enamel projections (CEP): these are tooth developmental deformities of the CEJ found on molars. The enamel is projected toward the entrance of the furcation and this projection may responsible for furcation invasion and localized severe bone loss around the teeth.
Palatoginival grooves (PGG): These are tooth developmental deformities of maxillary central and lateral incisors. They begin in lingual pits and extend vertically onto root surfaces and may extend to the root apex and are associated with increased gingival inflammation and plaque accumulation.
Root morphology: the mesial root surface of the maxillary first premolar presents with a pronounced concavity which may not be accessible to oral hygiene procedures or professional instrumentation.
