EVALUATION
Evaluation for hypertension has three objectives:1. to assess lifestyle and identify other cardiovascular risk factors or concomitant disorders that may affect prognosis and guide treatment.
2. to reveal identifiable causes of high BP.
3. to assess the presence or absence of target organ damage and cardiovascular disease (CVD)
1
TARGET ORGAN DAMAGE
HeartLeft ventricular hypertrophy
Angina or myocardial infarction
Heart Failure
Brain
Stroke or transient ischemic attack
Chronic kidney disease
Peripheral artery disease
Retinopathy
2
The relationship between BP and risk of CVD events is continuous, consistent, and independent of other risk factors.
The higher the BP, the greater is the chance of heart attack, heart failure, stroke, and kidney disease.
The risk of developing CVD doubles for every increment of 20 mm Hg Systolic (SBP) or 10 mm Hg of Diastolic (DBP).
The risk of dying of ischemic heart disease and stroke increases progressively and linearly when blood pressure exceeds 115/75 mm Hg.
3
The JNC-8 panel confirms that the >140/90 mmHg definition for hypertension remains the standard for diagnosis for individuals who do not have additional comorbidities.
4
Older than 50 years, SBP > 140 mmHg is a much more important CVD risk factor than DBP.
80-90% risk of developing hypertension by the age of 80 to 85 years.
SBP of 120–139 mmHg or DBP of 80–89 mmHg: considered as pre-hypertension and requires promoting lifestyle modification to prevent CVD.
5
Undiagnosed hypertension has been proven to shorten a life-span by 10-20 years
6ESSENTIAL / PRIMARY HYPERTENSION
Causative factors are unknown
about 90-95% of all hypertensive cases7
Identifiable cause in 5-10% of all cases of HTN
adults Disorders associated with secondary diseaserenal parenchymal disease
renovascular diseasesCushing's syndrome
Obstructive sleep apnea
primary hyperaldosteronism
pheochromocytoma
Thyroid Disorders
hyperparathyroidism
8
MEASUREMENT
Proper technique for obtaining accurate blood pressure measurements mandates;
Patient should be seated quietly for at least 5 minutes in a chair.
Feet on the floor, and arms supported at heart level.
An appropriate-sized cuff, a cuff bladder that encircles at least 80% of the arm, to ensure accuracy.At least two measurements should be taken during the visit
9Antihypertensive drugs are able to induce a series of adverse effects with the oral cavity, these includes:
# Xerostomia (DIURETICS like furosemide)
# Lichenoid reactions (adrenergic blocking agents like propanolol)# Burning mouth sensation (angiotensin -converting enzyme inhibitors like Captopril)
# Loss of taste sensation (angiotensin -converting enzyme inhibitors like Captopril)
# Gingival hyperplasia, (calcium antagonists Nifedipine ‘Adalat’)
# Extraoral manifestations such as sialadenosis (adrenergic blocking agents)
Oral manifestations
ARTERIAL HYPERTENSION
10
Blood Pressure Classification
• BP Classification
• SBP mmHg
• DBP mmHg
• Normal
• < 120 and
• < 80
• Pre-hypertension*
• 120-139 or
• 80-89
• Stage 1 Hypertension
• 140-159 or
• 90-99
• Stage 2 Hypertension
• > 160 or
• > 100
• *newly recognized, requiring
• lifestyle modifications
11
HypertensionClinical Manifestations
• Frequently asymptomatic until severe and target organ disease has occurredFatigue, reduced activity tolerance
Dizziness
Palpitations, angina
Dyspnea
12
Hypertension: Complications
Complications are primarily related to development of atherosclerosis (“hardening of arteries”), or fatty deposits that harden with age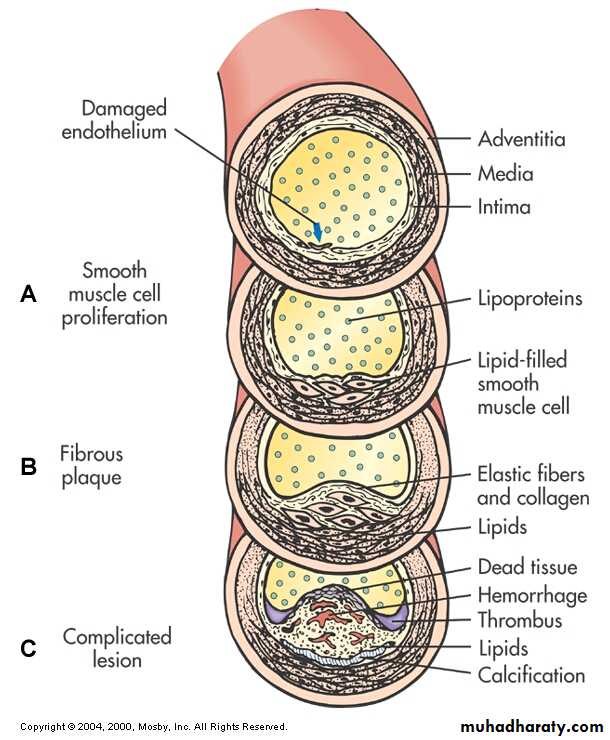
13
HypertensionDiagnosis
• Diagnosis requires several elevated readings over several weeks (unless > 180/110)• BP measurement in both arms
- Use arm with higher reading for subsequent measurements
14
HypertensionDiagnosis
Ambulatory BP MonitoringFor “white coat” phenomenon, hypotensive or hypertensive episodes, apparent drug resistance
15
Treatment Goals
Goal is to reduce overall cardiovascular risk factors and control BP by the least intrusive means possibleBP < 140/90
In patients with diabetes or renal disease, goal is < 130/80
16
Benefits of Lowering BP
Average Percent Reduction
Stroke incidence 35–40%
Myocardial infarction 20–25%
Heart failure 50%17
HypertensionCollaborative Care
• Lifestyle Modifications- Weight reduction
- Dietary changes (DASH diet)- Limitation of alcohol intake (< 2 drinks/day for men;
< 1/day for women)
- Regular physical activity
- Avoidance of tobacco use
- Stress management
18
HypertensionCollaborative Care
• Nutritional Therapy: DASH Diet = Dietary Approahes to Stop HTN- Sodium restriction
- Rich in vegetables, fruit, and nonfat
dairy products
- Calorie restriction if overweight
19
Hypertension: Drug Therapy
β – adrenergic blockers (suffix “olol”)(metoprolol, propranolol)
Block β – adrenergic receptors
↓ HR, ↓ inotropy, reduces sympathetic vasoconstriction)
Side effects
Bradycardia, hypotension, heart failure, impotence
20
Hypertension: Drug Therapy
Calcium Channel Blockers
Block movement of calcium into cells, causing vasodilation
Side effects
Brdaycardia, heart block
21
Hypertension: Drug Therapy
ACE Inhibitors (suffix “pril)Enalapril, captopril
Prevents conversion of angiotensin I to angiotensin II, thereby preventing the vasoconstriction associate with A II.
Side effects
Hypotension, cough
22
Hypertension: Drug Therapy
Thiazide-type DiureticsInhibit NaCl reabsorption
Side effects:
Electrolyte imbalances: ↓ Na, ↓ Cl, ↓ K** (advise K rich foods)
Fluid volume depletion (monitor for orthostatic hypotension)
Impotence, decreased libido
23
Hypertension: Drug Therapy
Adrenergic InhibitorsReduce sympathetic effects that cause HTN by:
Reducing sympathetic outflow
Blocking effects of sympathetic activity on vessels
Side effects
Hypotension
Varied, depending on specific drug
24
Hypertensive Crisis Clinical Manifestations
- Hypertensive encephalopathy (H/A, N & V,seizures, confusion, coma)
- Renal insufficiency
- Heart failure
- Pulmonary edema
25
Hypertensive Crisis
• Severe, abrupt elevation in BP
• The rate of in BP is more important than the absolute value
• Most common in patients with a history of HTN who have failed to comply with medications or who have been under-medicated
26
Hypertensive CrisisNursing and Collaborative Management
Hospitalization- IV drug therapy
- Monitor cardiac and renal function
- Neurologic checks
- Determine cause
- Education to avoid future crises
27




ARTERIAL HYPERTENSION
28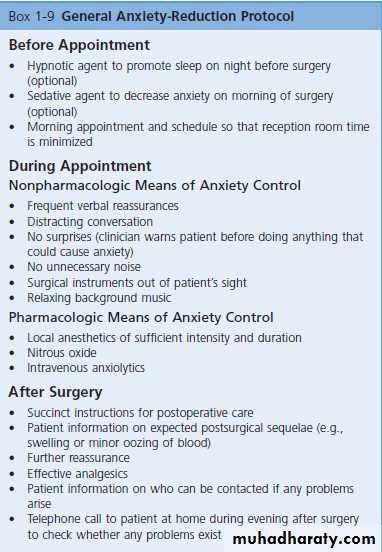
29
Dental management
- A well controlled hypertensive patients does not pose a risk in clinical practice.- Consultation with the supervising physician is advisable in order to know the degree of hypertension control and the medication prescribed at that time.
- The patient is to be instructed to take his or her medication as usual on the day of dental treatment.
- Prior to such treatment, the patient blood pressure should be recorded, and if the values are found to be high ( ≥ 180/110) , the visit should be postponed until adequate pressure control is achieved
- Cautious use of epinephrine in local anesthetic in patients taking non-selective b-beta blockers or peripheral adrenergic antagonists.
ARTERIAL HYPERTENSION
30
- Because some antihypertensive agents tend to produce orthostatic hypotension, sudden changes in chair position during dental treatment should be avoided.
ARTERIAL HYPERTENSION
Dental management
- It is preferable for the visits to be brief and in the morning.
- The prescription of anxiolytic agents may prove necessary in particularly anxious patients (5-10 mg of diazepam the night before and 1-2 hours before the appointment) before dental treatment, or altaernatively sedation with nitrous oxide may be considered.
- Vasoconstrictor use should be limited, taking care not to exceed 0.04 mg of adrenaline (2 carpules containing 1.8 ml of anesthetic with adrenalin 1: 100,000)
31
- A good local anesthetic technique should be performed, avoiding intravascular injection and using a maximum of two anesthetic carpules with vasoconstrictor. If more anesthesia is needed, it should be provided without vasoconstrictor. Absorbable suture are to be avoided with adrenalin.
ARTERIAL HYPERTENSION
Dental management
- When the patient does not present good blood pressure control, it is best to refer him or her to the physician in order to ensure adequate control before dental treatment.
- In the case of emergency dental visits, treatment should be conservative, with the use of analgesics and antibiotics.
- Surgery is to be avoided until adequate blood pressure control has been secured.
32• Certain nonsteroidal antiinflammatory drugs (NSAIDs), such as ibuprofen, indomethacin or the naproxen, can interact with antihypertensive drugs (beta-blockers, diuretics), thereby lowering their antihypertensive action. Normally more than five days of treatment with both types of drugs are required for interactions to manifest; as a result, NSAIDs should not be prescribed for longer than this five-day period.
- Avoid NSAID because of their renal effects which cause retention of sodium and water that lead to raise in the blood pressure.
ARTERIAL HYPERTENSION
Dental management
33