Paracetamol
Paracetamol (acetaminophen) is the drug most commonly used in overdose in the UK.Toxicity results from formation of an intermediate reactive metabolite which binds covalently to cellular proteins, causing cell death.
This results in hepatic and occasionally renal failure.
In therapeutic doses, the toxic intermediate metabolite is detoxified in reactions requiring glutathione, but in overdose, glutathione reserves become exhausted
Management
Management
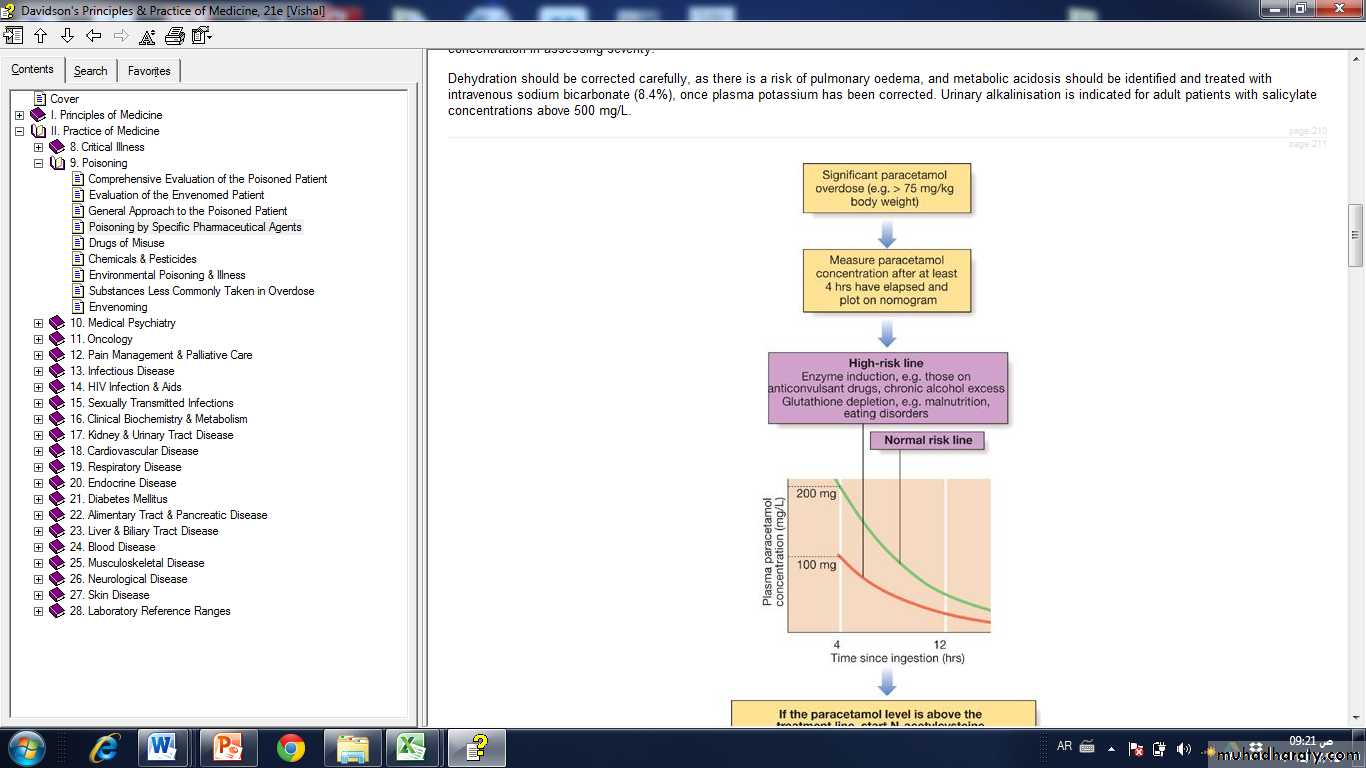
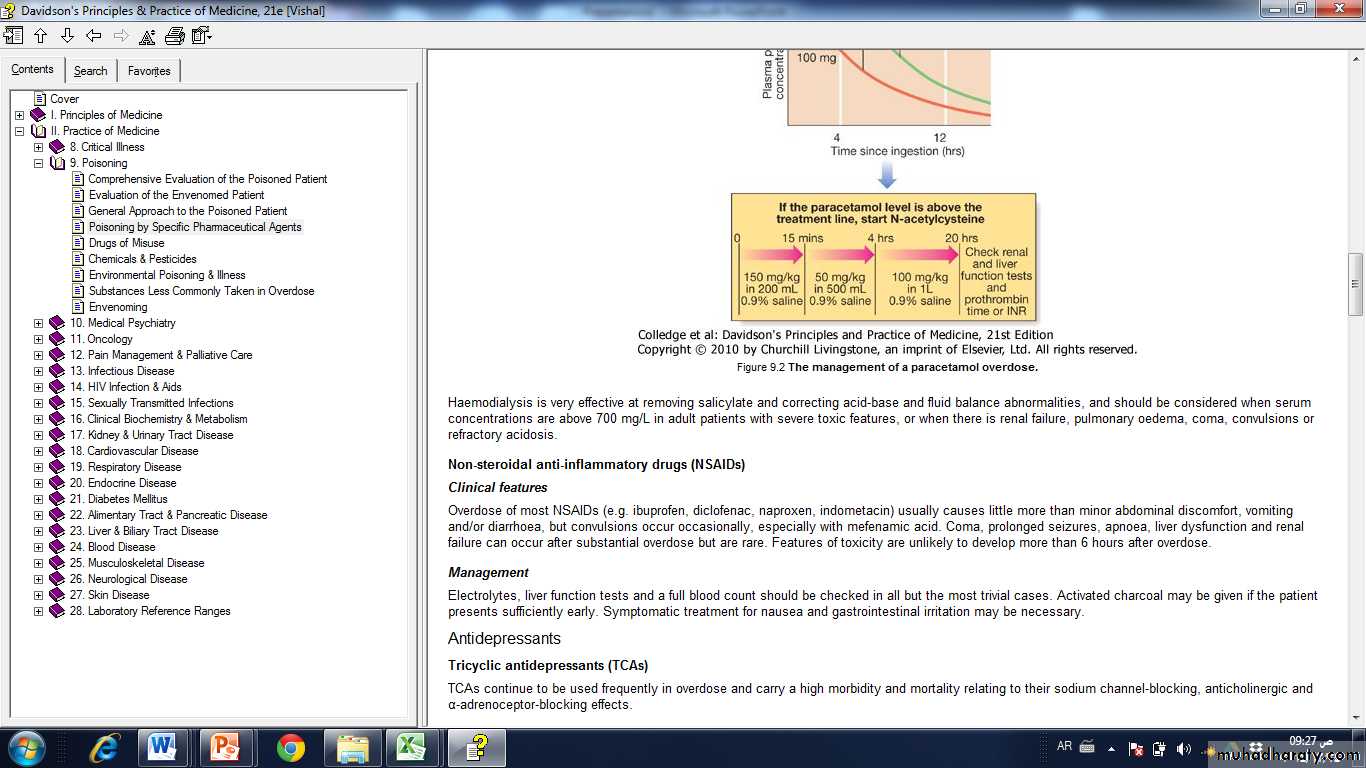
Activated charcoal may be used in patients presenting within 1 hour.Antidotes for paracetamol act by replenishing hepatic glutathione. Acetylcysteine given intravenously (or orally in some countries) is highly efficacious if administered within 8 hours of the overdose.
However, since efficacy declines thereafter, administration should not be delayed in patients presenting after 8 hours to await a paracetamol blood concentration result.
The antidote can be stopped if the paracetamol concentration is shown to be below the appropriate treatment line.
The most important adverse effect of acetylcysteine is related to dose-related histamine release, the 'anaphylactoid' reaction, which causes itching and urticaria, and in severe cases, bronchospasm and hypotension.
Most cases can be managed by temporary discontinuation of acetylcysteine and administration of an antihistamine. An alternative antidote in paracetamol poisoning is methionine 2.5 g orally 4-hourly to a total of four doses, but it is less effective, especially after delayed presentation.
If a patient presents more than 15 hours after ingestion, liver function tests, prothrombin time (or international normalised ratio-INR), renal function tests and a venous bicarbonate should be measured, the antidote started, and a poisons information centre or local liver unit contacted for advice if results are abnormal.
An arterial blood gas sample should be taken in patients with severe liver function abnormalities; metabolic acidosis indicates severe poisoning.
Liver transplantation should be considered in individuals who develop life-threatening liver failure due to paracetamol poisoning
If multiple ingestions of paracetamol have taken place over several hours or days (i.e. a staggered overdose), acetylcysteine should be given when the paracetamol dose exceeds 150 mg/kg body weight in any one 24-hour period or 75 mg/kg body weight in 'high-risk groups'
Salicylates (aspirin)
Clinical featuresSalicylate overdose commonly causes nausea, vomiting, sweating, tinnitus and deafness.
Direct stimulation of the respiratory center produces hyperventilation and respiratory alkalosis.
Peripheral vasodilatation with bounding pulses and profuse sweating occurs in moderately severe poisoning.
Serious salicylate poisoning is associated with metabolic acidosis, hypoprothrombinaemia, hyperglycaemia, hyperpyrexia, renal failure, pulmonary oedema, shock and cerebral oedema.
Agitation, confusion, coma and fits may occur, especially in children.
Toxicity is enhanced by acidosis, which increases salicylate transfer across the blood-brain barrier.
Management
Activated charcoal should be administered if the patient presents early.Multiple doses of activated charcoal may enhance salicylate elimination but currently are not routinely recommended.
The plasma salicylate concentration should be measured at least 2 (in symptomatic patients) or 4 hours (asymptomatic patients) after overdose and repeated in patients with suspected serious poisoning, since concentrations may continue to rise some hours after overdose.
In adults, concentrations above 500 mg/L and 700 mg/L suggest serious and life-threatening poisoning respectively, although clinical status is more important than the salicylate concentration in assessing severity.
Dehydration should be corrected carefully, as there is a risk of pulmonary oedema, and metabolic acidosis should be identified and treated with intravenous sodium bicarbonate (8.4%), once plasma potassium has been corrected. Urinary alkalinisation is indicated for adult patients with salicylate concentrations above 500 mg/L.
Haemodialysis is very effective at removing salicylate and correcting acid-base and fluid balance abnormalities, and should be considered when serum concentrations are above 700 mg/L in adult patients with severe toxic features, or when there is renal failure, pulmonary oedema, coma, convulsions or refractory acidosis.