Rheumatic Fever
It is caused by Group A Streptococcus upper
respiratory tract infections.
The incidence of both initial attacks and
recurrences of acute rheumatic fever peaks in
children
5-15 yrs
. of age.
The onset of acute rheumatic fever.
(approximately
2-4
wk
.) after GAS pharyngitis
12/6/2017
2
Diagnosis of acute rheumatic fever can
be established when a patient fulfills
(2 major) or
(1 major and 2 minor) criteria
+
evidence of preceding GAS
infection.
12/6/2017
3
The 5 Major Criteria are
1.
Migratory Polyarthritis
2.
Carditis
3.
Chorea Sydenham
4.
Erythema Marginatum
5.
Subcutaneous Nodules
12/6/2017
4
Minor Criteria are:
1)
Arthralgia (only if arthritis is not used as a
major criterion)
2)
Fever
3)
Elevated acute phase reactants ( ESR ,CRP)
4)
Prolonged P-R interval on ECG (unless
carditis is a major criterion).
12/6/2017
5
Recent Group A Streptococcus
Infection
An absolute requirement for the diagnosis
of acute RF.
+ vet throat culture or rapid streptococcal
antigen test( Streptozyme test)
Elevated or rising serum antistreptococcal
antibody titers. ASOT, anti–DNase B,
antihyaluronidase
12/6/2017
6
Migratory Polyarthritis :
1)
Occurs in 75% of patients
2)
typically involves larger joints knees, ankles, wrists, and elbows.
(spine, small joints of the hands and feet, or hips is uncommon).
3)
Rheumatic joints are classically hot, red, swollen, and
exquisitely tender.
4)
migratory in nature; that is, a severely inflamed joint can
become normal within 1-3 days without treatment.
5)
A dramatic response to salicylates is characteristic feature . If a
child is suspected to have acute RF, it is useful to withhold
salicylates and observe for migratory progression and the
absence of such a response should suggest an alternative
diagnosis.
6)
Rheumatic arthritis is almost never deforming
12/6/2017
7
Carditis :
occurs in 50-60% of all cases,
pancarditis( myocardium, pericardium, and
endocardium)
Endocarditis (valvulitis) is a universal
finding in rheumatic carditis, whereas the
presence of pericarditis or myocarditis is
variable
isolated mitral valvular disease or
combined aortic and mitral valvular
disease.( Isolated aortic or right-sided
valvular involvement is uncommon).
12/6/2017
8
Carditis usually presents as tachycardia , cardiac
murmurs, cardiomegaly , heart failure with
hepatomegaly , peripheral and pulmonary edema
Mitral regurgitation is characterized typically by a
high-pitched apical holosystolic murmur radiating to
the axilla. Aortic insufficiency is characterized by a
high-pitched decrescendo diastolic murmur at the left
sternal border.
A change in the 2015 revision of the Jones Criteria is
the acceptance of subclinical carditis (defined as echo
evidence of valvulitis without a murmur of valvulitis)
or clinical carditis (with a murmur
)
12/6/2017
9
Chorea Sydenham:
10-15% of patients with acute rheumatic fever
The latent period from acute GAS infection to chorea is usually
substantially longer than for arthritis or carditis and can be months
usually presents as an isolated, movement disorder. Emotional
liability, incoordination, poor school performance, uncontrollable
movements, and facial grimacing, all exacerbated by stress and
disappearing with sleep.
chorea rarely, if ever, leads to permanent neurologic sequelae.
Clinical maneuvers to elicit features of chorea include:
(1)
demonstration of milkmaid’s grip
(2)
spooning and pronation of the hands when the patient’s arms are
extended
(3)
wormian movements of the tongue upon protrusion
(4)
examination of handwriting to evaluate fine motor movements
12/6/2017
10

•
is a rare (approximately 1% )
•
characteristic rash of acute rheumatic fever.
•
It consists of erythematous,
serpiginous, macular lesions
with pale centers that are not
pruritic. It occurs primarily on
the trunk and extremities,
but not on the face, and it can
be accentuated by warming
the skin
.
Erythema Marginatum :
12/6/2017
11
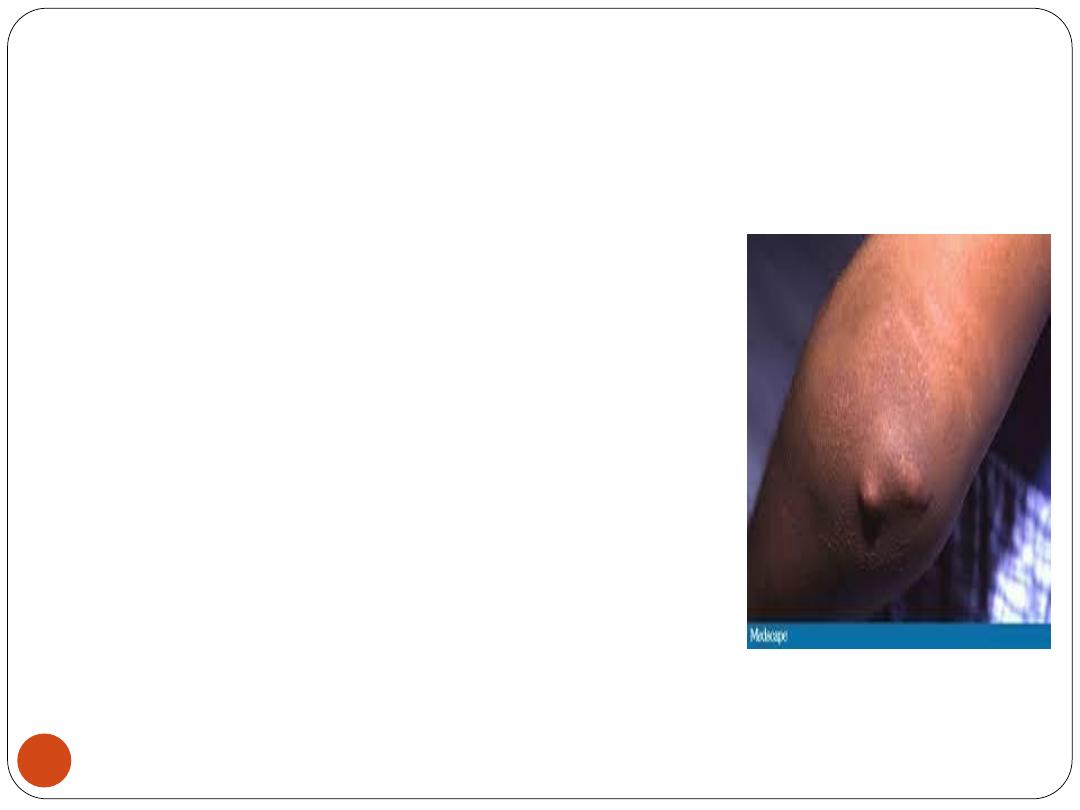
Subcutaneous
Nodules
rare (≤1% of patients )
finding and consist of firm nodules
approximately 1 cm in diameter
along the extensor surfaces of
tendons near bony prominences.
There is a correlation between the
presence of these nodules and
significant rheumatic heart disease.
12/6/2017
12
TREATMENT
All patients with acute rheumatic fever should
be placed on bed rest and monitored closely
for evidence of carditis.
Antibiotic Therapy:
regardless of the throat culture results, the
patient should receive 10 days of orally
administered penicillin or amoxicillin or
erythromycin or a single IM injection of
benzathine penicillin to ensure eradication of
GAS from the upper respiratory tract.
12/6/2017
13
Anti-inflammatory Therapy
Patients with polyarthritis and those with carditis without
cardiomegaly or CHF should be treated with oral salicylates.
The usual dose of aspirin is 50-70 mg/kg/day in 4 divided
doses PO for 3-5 days, followed by 50 mg/kg/day in 4
divided doses PO for 3 wk. and half that dose for another 2-4
wk.
Patients with carditis With cardiomegaly and/or CHF
should receive corticosteroids. The dose of prednisone is 2
mg/kg/day in 4 divided doses for 2-3 wk. followed by half
the dose for 2-3 wk. and then tapering of the dose by 5
mg/24 hr. every 2-3 days
.
12/6/2017
14
Supportive therapies for patients with moderate
to severe carditis include digoxin, fluid and salt
restriction, diuretics, and oxygen
Sydenham Chorea; Sedatives may be helpful
early in the course of chorea; phenobarbital
,haloperidol ,chlorpromazine. Some patients may
benefit from corticosteroids
.
12/6/2017
15
PREVENTION
Prevention of both initial and recurrent episodes of
acute RF depends on controlling GAS infections of
URT
A. primary prevention
Appropriate antibiotic therapy instituted before the
9th day of symptoms of acute GAS pharyngitis is
highly effective in preventing first attacks of acute
RF . However, approximately.
Oral pencillin or erythromycin 50 mg/kg/day or
single IM benzathine penicillin G 600.000 <27 kg
and 1.200.000 for those >27kg
12/6/2017
16
B. Secondary Prevention
Individuals who have already suffered an attack of acute RF are
susceptible to recurrences of RF with any subsequent GAS URTI.
Therefore, these patients should receive continuous antibiotic
prophylaxis to prevent recurrences
Antibiotic prophylaxis should continue in these patients until the
patient reaches 21 yrs. of age or until 5 yrs. since the last RF attack,
whichever is longer. (Sometimes lifelong prophylaxis is needed for
those with carditis and residual heart disease).
The regimen of choice for secondary prevention is a single IM injection
of benzathine penicillin G (600,000 IU for children weighing ≤27kg
,1.2 million IU for those weighing >27kg) every 4 wk.
In compliant patients, oral Penicillin V 250 mg twice daily ,
sulfadiazine or sulfasoxazole are equally effective.
For patient who is allergic to both penicillin and sulfonamides, a
macrolide (erythromycin or clarithromycin or azithromycin) may be
used
12/6/2017
17