Nephrotic syndrome
Dr.Basma Adel
FIFTH GRADE 2017-2018
At the end of this lecture you
should know:
Types
Pathophysiology
Clinical manifestations
D.Dx.
Investigations.
Treatment .
Complications.
12/3/2017
2
12/3/2017
3
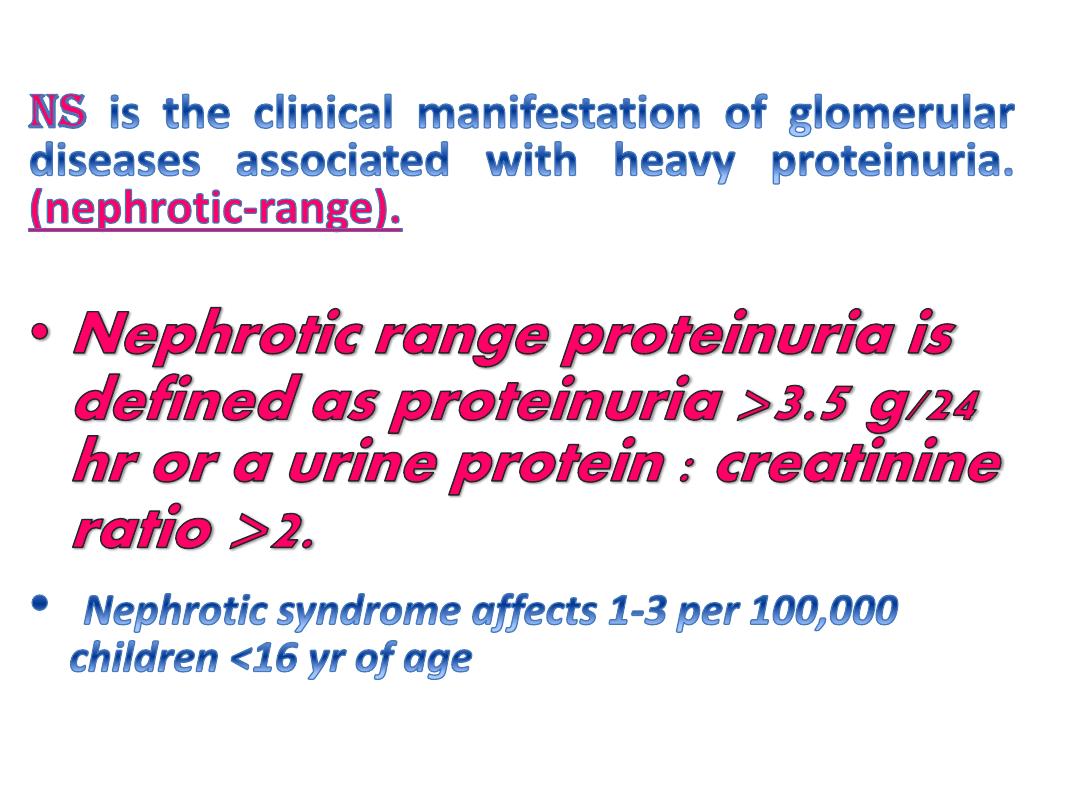
heavy proteinuria
edema
hypoalbuminemia
hyperlipidemia
.
12/3/2017
4
12/3/2017
5
( However, this theory does not apply to all pts with NS).
Proteinuria & Hypoalbuminemia is due to
increase permeability of the glomerular capillary
wall
Edema and decreases plasma oncotic
pressure
transudation
of
fluid
from
the
intravascular
compartment
to
the
interstitial space
The reduction in intravascular volume
decreases renal perfusion pressure
Activation of renin-angiotensin --
aldosterone system increase
reabsorption of Na,H2O
12/3/2017
6
• Hyperlipidemia is due to hepatic lipoprotein
synthesis (stimulated by hypoalbuminemia)
combined with decrease lipid catabolism due
to urinary loss of lipoprotein lipase
12/3/2017
7
1- Idiopathic (most common 90%).
2- Secondary to other diseases or
syndromes.
3- Congenital.
NS can be divided into:
12/3/2017
8
It is divided into the following pathological types:
1.Minimal Change NS(85%) :characterized by effacement "fusion"
of the epithelial cell foot processes
2. Focal Segmental Glomerulosclerosis :characterized by
mesangialproliferation and segmental scarring
3.Membranous Nephropathy: characterized by thickening of
basement membrane with subepithelial deposits.
4. Other types include: Mesangial Proliferation &
Membranoproliferative Glomerulonephritis (type 1 & 2).
12/3/2017
9
Clinical manifestations
12/3/2017
10
usually occur between
2-6
yr.(MCNS), whereas FSGS is tend to
occur in older children.
: and subsequent
relapses may follow minor infections
or sometimes insect bite.
12/3/2017
11
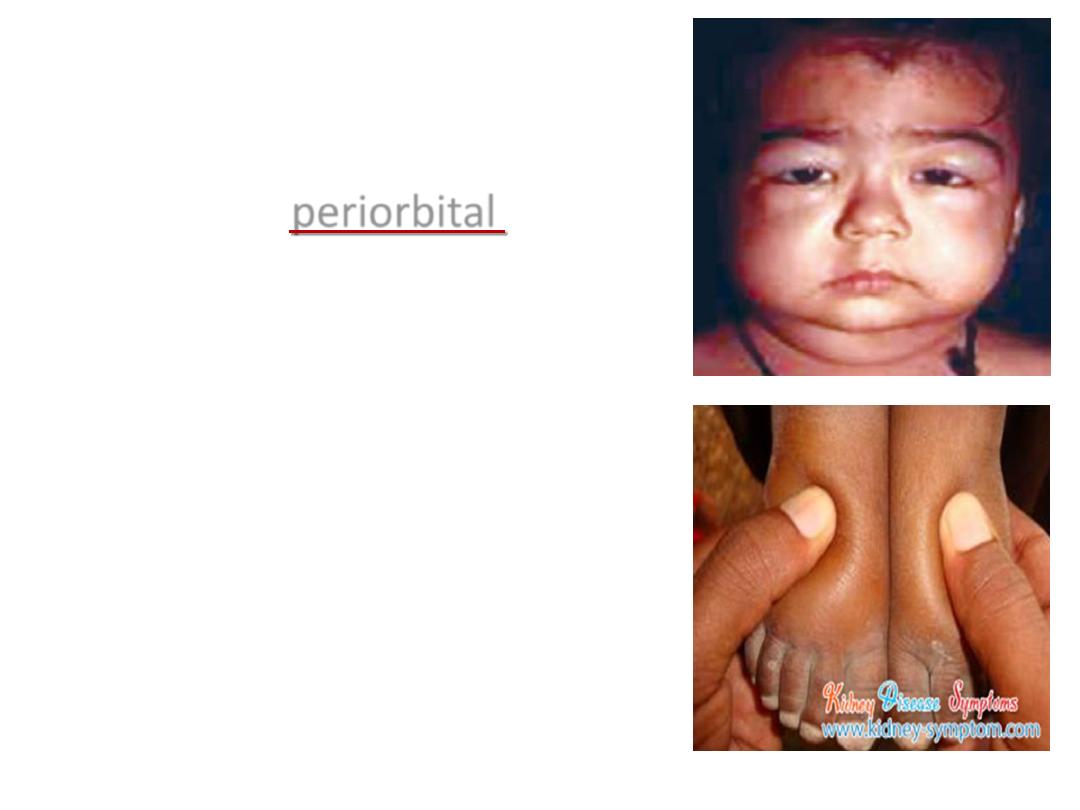
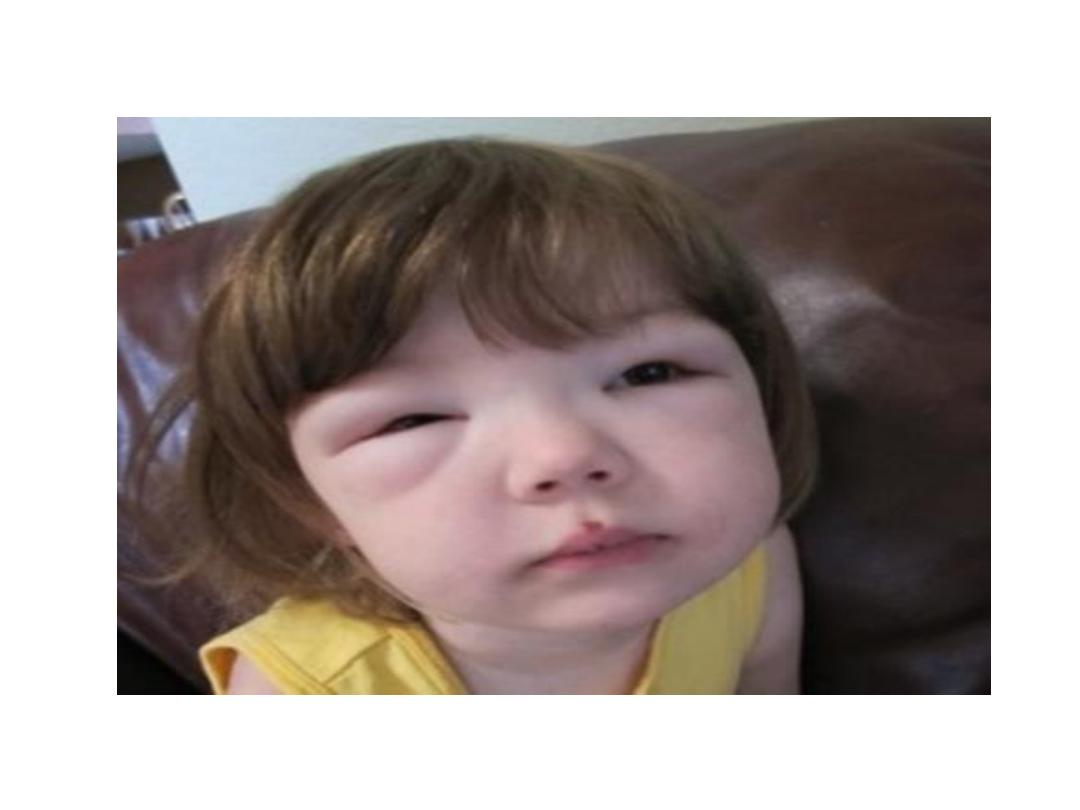
Children usually present
With mild
periorbital
&
lower extremities edema.
12/3/2017
12

Then edema becomes generalized with
development of ascites,
pleural effusions, and
genital edema
Other symptoms include:
irritability, anorexia,
abdominal pain & diarrhea
12/3/2017
13

D.Dx
I.
Glomerulonephritidis,
II.
Protein-losing enteropathy.
III.
Protein malnutrition (kwashiorker)
IV.
Hepatic failure
V.
Congestive HF.
12/3/2017
14
INVx:
• GUE for Proteinuria (3+ or 4+) or(> 40 mg/m2/hr) or
(>150 mg/kg/hr).
• Urinary protein/creatinine ratio (1st voiding at morning)
>2.
• Serum Albumin <2.5 g/ dL.
• Serum Cholesterol & Triglyceride (cholesterol >200
mg/dL).
• Serum Urea & Creatinin, C3 & C4 are typically normal.
12/3/2017
15
• Age <1 yr or >8 yr
• Family hx of renal disease,
• Extrarenal findings "
(arthritis, rash, anemia),
• hypertension,Hematuria,
Pulmonary edema,
• Renal insufficiency,
Hypocomplementemia
• Resistance to steroid Rx.
Renal
Biopsy is
not
routinely
indicated
unless :
12/3/2017
16

Treatment:
Corticosteroids are the cornerstone in Rx of NS
Prednisone orally, 60 mg/m2/day
(max. 80) as single dose in morning
For 4-6 wk ).
Then the dose should be tapered to
40 mg/m2 EOD for at least 4 wk,
then tappered & stopped over the
next 1-2 mo ( total 3-4 mo ).
12/3/2017
17
The response( -ve or trace proteinuria for 3 consecutive
days). to steroid usually occur within 2-4 wk of daily steroid
Rx
• Children with 1st episode with mild to moderate edema
can be managed as outpatient by the following (in addition
to prednisone):-
1. Salt intake "No added salt".
2. Diuretics orally ” with caution due to the risk of
thromboembolism.”
12/3/2017
18
• Children
with severe
edema,
should be
hospitalized
& managed
by the
following (in
addition to
prednisone)
1.Fluid restriction (in
addition to sodium
restriction) may be
necessary if the child is
hyponatremic
2.Swollen scrotum may be
elevated.
3. Diuretics e.g.
furosemide orally or IV,
1-2 mg/kg/dose.
4. If the above measures
are not effective, give
25% albumin IV (0.5-1
g/kg/dose) slowly
followed by furosemide
12/3/2017
19
• Relapse in NS: Many children with NS will
experience at least 1 relapse
• patients who are frequent relapsers, steroid
dependent or resistant or children suffer from
severe SE of corticosteroids are candidate for
alternative agents such as Cyclophosphamide,
Cyclosporine..ets.
• ACE inhibitors & Angiotensin II blockers may be
helpful as adjunct Rx to decrease proteinuria in
steroid-resistant patients.
12/3/2017
20
Complications:
1• Infection; it is the major Cx of NS, Spontaneous bacterial
peritonitis is the most frequent infection, although sepsis, pneumonia,
cellulitis, and UTI may also occur. S. pneumoniae is the most common
organism as well as other Gram -ve bacteria e.g. E. coli.
Vaccinations, especially "polyvalent" pneumococcal, varicella
& influenza vaccines can be given during remission or low
dose alternate day steroids
Note: Corticosteroid Rx usually mask fever and other signs
of inflammation,
thus it need high index of suspicion for infection combined
with aggressive Rx after Dx
2 • Thromboembolism; it is uncommon Cx due to high prothrombotic factors
(fibrinogen level, thrombocytosis, hemoconcentration, relative
immobilization) and low fibrinolytic factors (urinary losses of antithrombin III,
proteins C and S), thus overaggressive diuresis should be avoided .Anti-
coagulation Px is not recommended unless there is previous thromboembolic
event
3• Hyperlipidemia; CVS events e.g. MI is rare in children.
4• Psychological effects; patient with NS should not be considered as an "ill
12/3/2017
21
Secondary Nephrotic Syndrome
1. Glomerular diseases may have a nephrotic component e.g. Membranous
nephropathy; Membranoproliferative GN, PostinfectiousGN , SLE, and HSP
2. Infections & infestation e.g. HBV, HCV, HIV, Malaria and Schistosomiasis.
3. Drugs e.g. NSAIs, Penicillamine, Captopril, Phenytoin, Gold & Lithium.
4. Malignancy e.g. Lymphoma & Leukemia (but mainly in adults).
5. Syndromes that may associated with NS include: Alport syndrome, Hurler
syndrome, Alagille syndrome, Glycogen storage disease .... etc
12/3/2017
22
Congenital Nephrotic Syndrome
Appears at birth or within the 1st 3 mo pf life.
Causes of congenital NS include:-
1. Finnish-Type NS: It is the most common cause of
congenital NS, inherited as AR. It is manifested in utero
as fetal hydrops, large placenta high a fetoprotein;
prematurity, respiratory distress, hypothyroidism and
separation of cranial sutures.
The disease is persistent edema and progressive renal failure
with death by age of 5 yrs
Rx. Aggressive nutrition , ACE inhibitor, IV albumin, IVIG,
unilateral (or bilateral) nephrectomy, chronic dialysis, and
kidney transplantation; whereas corticosteroids &
immunosuppressives are of no value in Finnish-type NS.
2. Congenital Infections e.g. TORCHS can cause congenital NS
12/3/2017
23

12/3/2017
24

12/3/2017
25