Dr. Bushra Rashid
Radiographic examination in childrenObjectives
Purpose for prescribing radiographsCriteria for exposing of radiographsin asymptomatic children
Child preparation and ManagementRadiographic techniques commonly used in children
The risk the patient may encounter during therapyWhy children are higher risk than adults?
important considerations when deciding whether to perform a radiographic examination for children are• The stage of dentition development
(2) The risk of dental caries.
CRITERIA FOR EXPOSING OF RADIOGRAPHSIN ASYMPTOMATIC CHILDREN
Guideline for Prescribing Dental RadiographsNew Patient
Primary Dentition (before eruption
of first permanent tooth)
Transitional Dentition (after eruption of
first permanent tooth)
All new patients to assess dental
diseases and growth and
development
Posterior bite-wing examination
if proximal surfaces of primary
teeth cannot be visualized or
probed
Individualized radiographic examination
consisting of periapical/
occlusal views and posterior bitewings
or panoramic examination
and posterior bite-wings
Primary Dentition (before eruption
of first permanent tooth)Transitional Dentition (after eruption of first permanent tooth)
Clinical caries or high-risk factorsfor caries
Posterior bite-wing examination 6-month intervals or until no carious lesions are evident
Posterior bite-wing examination 6-month intervals or until no carious lesions are evident
No clinical caries and low-risk
Factors for cariesPosterior bite-wing examination at 12- to 14-month
intervals if
proximal surfaces of primary teeth cannot be visualized or
probed
Posterior bite-wing examination at
12- to 24-month intervals
Recall Patient
Patient recall cont….
Periodontal disease or a history of
periodontal treatment
Individualized radiographic examination consisting of selected periapical and/or bite-wing radiographs for areas where periodontal disease can be demonstrated clinically
Tell show do (TSD)
CHILD PREPARATION ANDMANAGEMENT
technique for preparingthe child to be radiographed:
Tell
The child is explained and theX-ray machine is compared to a camera;
Show
The X-ray tube isplaced near doll’s mouth;
Do
The X-ray is taken once the child is
cooperative and ready
RADIOGRAPHIC TECHNIQUES COMMONLY USED IN CHILDREN
1. Intraoral
– PA– Bite wing
– Occlusal
2. Extraoral
– TMJ and lateral oblique view-Lateral cephalograms.
-Orthopantomography (OPG)
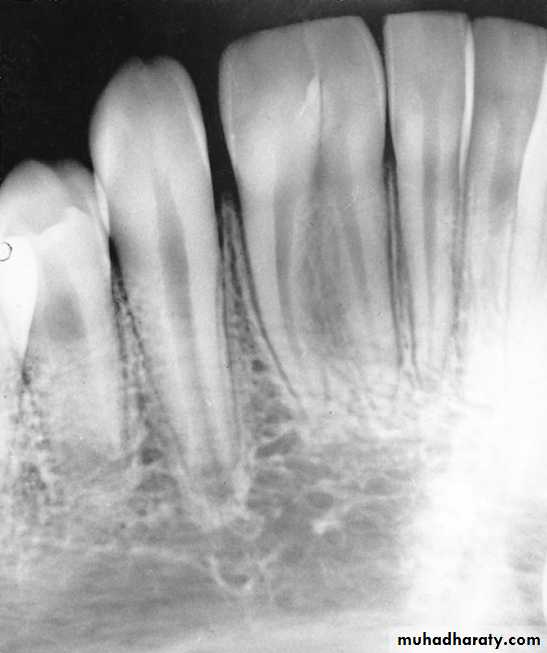
• Intraoral Periapical (IOPA) RadiographsIndications
1. To evaluate the development of the root end and to study the periapical tissue
2. To detect alterations in the integrity of the periodontal membrane
3. To evaluate the prognosis of the pulp treatment by observing the health of the periapical tissues4. To identify the stage of development of unerupted teeth
A, Pulp of the fi rst permanent molar was exposed by caries. The tooth was considered a candidate for the calcium hydroxide pulpotomy technique.
B, Calcifi ed
bridge has formed over the vital pulp in the canals.C, Continued
root development and pulpal recession are indicative of continuing pulpal vitality. The crown should be supported with a full-coverage restoration.


Mature and immature teeth in the x-ray
Closed apex maxillary central incisors (mature)
Open apex maxillary central incisors (immature)

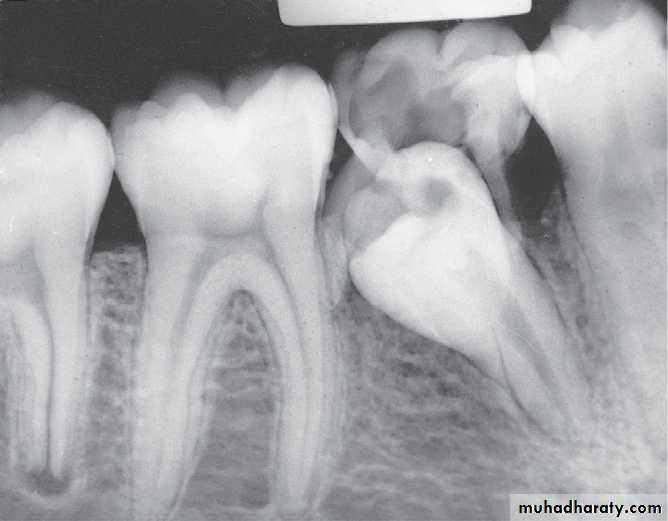
Ankylosed 1st mandibular molar
5. To detect developmental abnormalities like supernumerary, missing or malformed teeth
6. For early detection of pathologic changes associated with teeth7. For space analysis in the mixed dentition
8. To assess the path of eruption of permanent teeth9. To evaluate the extent of traumatic injuries to the root and alveolus.
Some of the indications of IOPA:(A) Evaluate the extension of caries; (B) Odontome; (C) Bifid premolar root; (D) Pathologic root resorption of lower central incisors; (E) Pre-eruptive caries
• Bite Wing RadiographsIndications
• Early detection of incipient interproximal caries• To understand the configuration of the pulp chamber
• Record the width of spaces created by premature
loss of deciduous teeth• Determine the presence or absence of premolar teeth
• To determine the relation of a tooth to the occlusal plane for possibility of tooth Ankylosis• Detect levels of periodontal bone at the interdental area
• Detect secondary cariesPosterior bite wing Radiograph
Record the width of spaces created by prematureloss of deciduous teeth

Indications of bite wing radiograph
(A) Interproximal caries detection;
(B) Evaluate the interdental bone

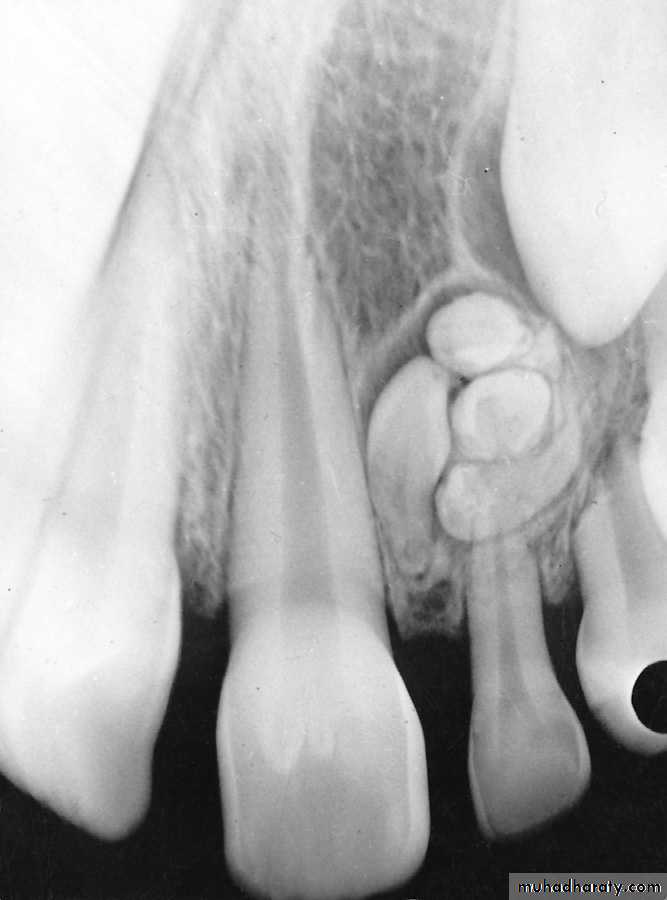
Occlusal RadiographIndications:
Determine the presence, shape and position of midline supernumerary teeth.Determine impaction of canines
Determine the presence or absence of incisors
Assess the extent of trauma to teeth and anterior
segments of the arches
In case of trismus and trauma, where the patient cannot open the mouth completely
Determine the medial and lateral extent of cysts and tumors.
Palatal cyst can be easily diagnosed in an occlusal radiograph
Occlusal radiographSupernumerary tooth

mandibular occlusal film shows the expansion of the
buccal cortical plate and the associated bone loss with this cyst.
Occlusal radiograph
Detection the Presence of permanent anterior teeth
Occlusal radiograph
Dilacerated tooth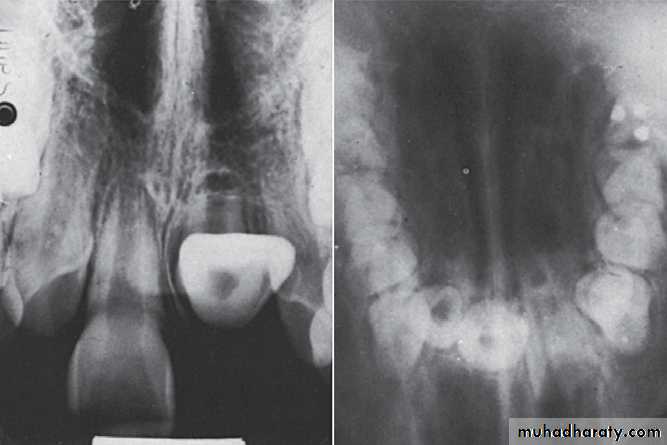
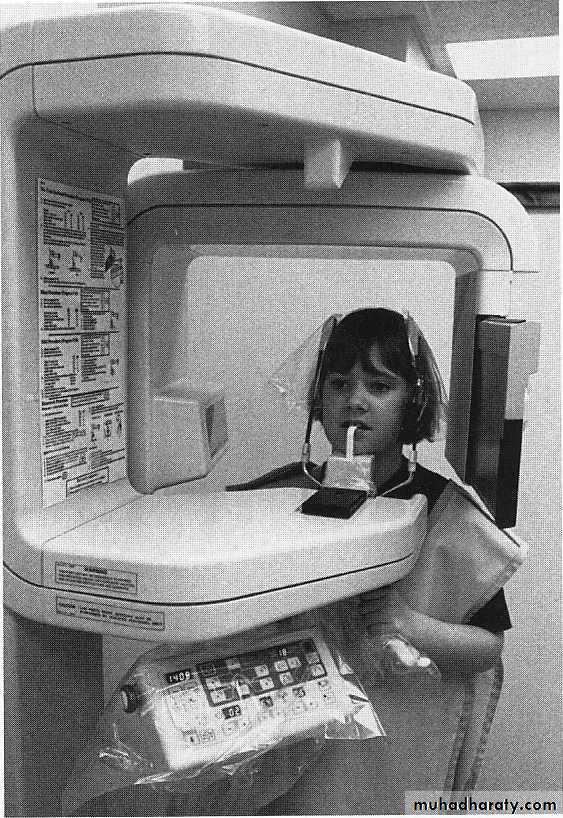
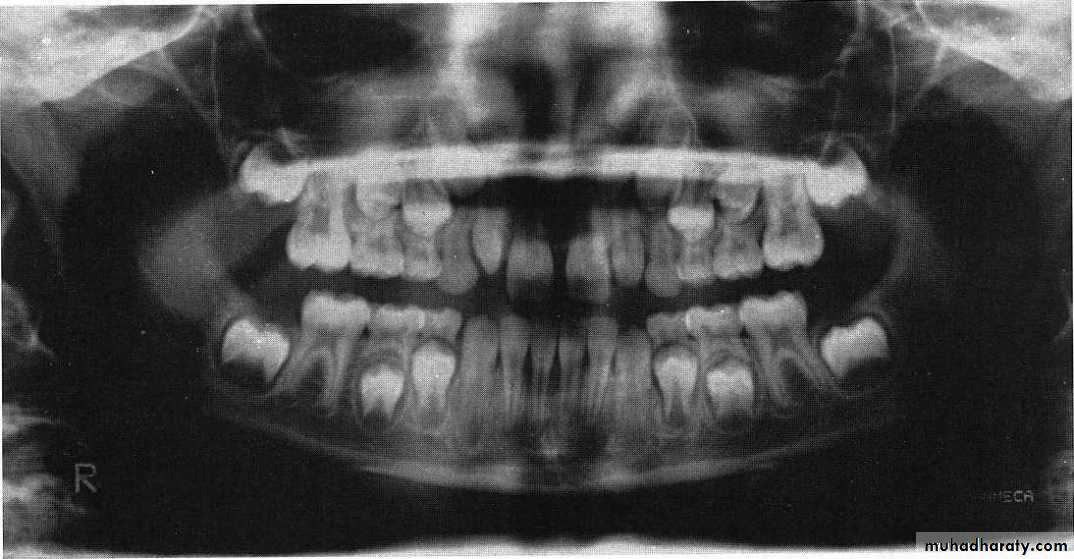
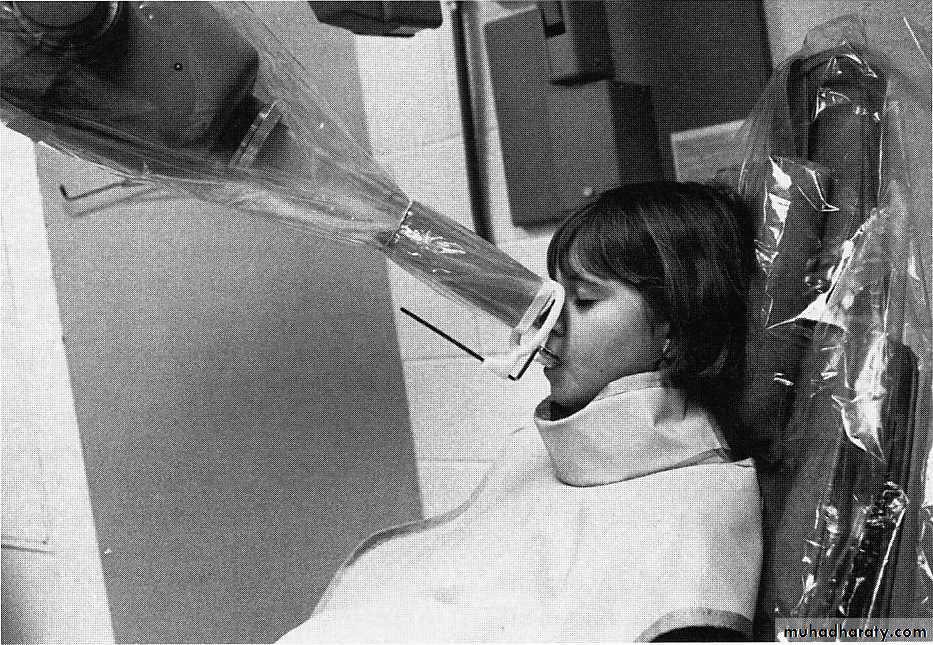
PANORAMIC RADIOGRAPHY
A panoramic radiographic unit can be used for examination of children.Advantages
Since the examination is obtained without placement of the film in the mouth, it does not alarm the anxious child who may refuse an intraoral film.
Moreover, the young patient may find the movement entertaining or fun.
This view can be useful in handicapped children and for viewing a wide area of the TMJ and associated region.
Panoramic is recommended at approximately the time of the early mixed dentition to assess
1. the dental age of the patient and
2. to aid in the early diagnosis of congenital and developmental anomalies.Panoramic radiograph
A diagnostic film includes
the teeth,the supporting structure,
the maxillary region extending to the superior third of the orbit,
the entire mandible including the temporomandibular joint region.
Panoramic used to diagnose:
Condylar fractures,traumatic cysts,
and anomalies that might have gone undetected with the routine periapical survey.
disabled patients are examined if the patient can sit in a chair and hold his or her head in positionIt may be necessary to administer relaxants or sedatives to palsied or spastic patients, who are more difficult to control when they are emotionally charged by the dental visit.
Disadvantages: panoramic radiography is:
However, staying completely immobile for 15 seconds may not be possible for some very young children.lack of image detail for diagnosing early carious lesions. Adjunct bite-wing radiographs and selected periapical radiographs are required for that task.
Patient’ age nearly 9 because the lower canines erupted and their eruption on 9-10 year and the upper lateral emerging now
This child is 7-8 years old because he has the upper maxillar centrals erupted (depending on schedule of time of eruption of permanent teeth (eruption lecture)

PURPOSES FOR PRESCRIBINGRADIOGRAPHS
It depends on the following criteria:1.Evaluation of the Development of Dentition
This can be done by observing the radiographs for the following:
A. Stages of development, eruption and exfoliation of teeth
B. Amount of root formation
C. Physiologic root resorption
D. Amount of bone over the
erupting tooth
E. Degree of pulp maturity.

2.Pathologic Evaluation
It includes:A. Caries detection
B. Evaluation of traumatic
injuries
C. Degree of pulp involvement such as proximity of caries to pulp horn, internal resorption or calcific degeneration
D. Evaluation of periodontal health by observing thickness of periodontal ligament, furcation involvement, bone loss, external resorption, etc.

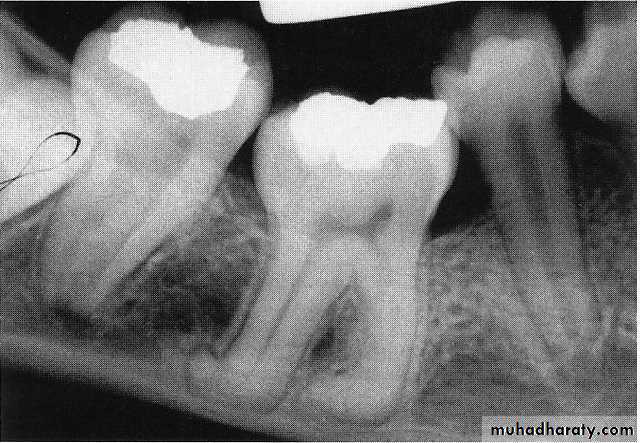
Internal resorption after calcium hydroxide pulpotomy in a primary tooth
Deep caries in the first primary molar and due to that caries resorption in the bifurcation areaDeep caries in the mandibular second primary molar



Periapical radiographs
3.Detection of Developmental Anomalies
Commonly observed anomalies are:
A. Widely divergent roots
B. Sharply curved pulp canals
C. Alterations in the number and
length of roots
D. Ectopically positioned teeth
E. Ankylosis
F. Supernumerary teeth
G. Congenitally missing teeth
H. Malformed teeth such as microdontia, macrodontia, dens in dente, taurodontism, gemination, fusion, root dilacerations, etc.


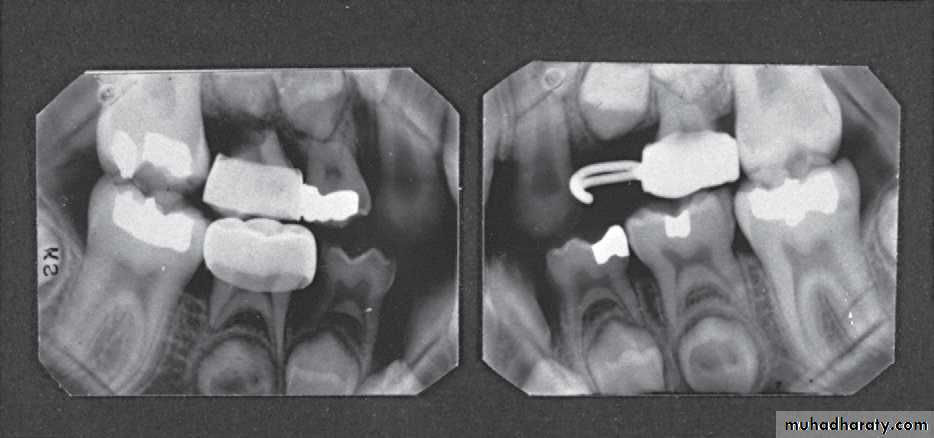
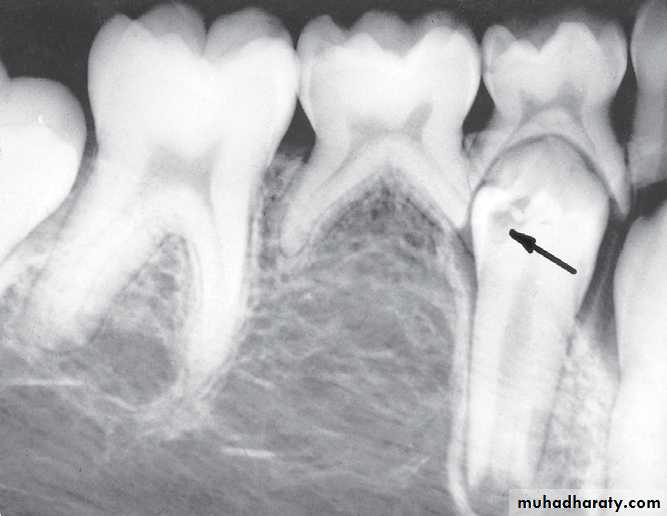
Infected mandibular second primary molar
has caused hypoplasia of the second premolar and delayed eruption of the tooth.Pre-eruptive “caries” on the crown of an
unerupted first premolar (arrow).
Odontoma
Necrotic tooth resulting from a carious exposure of the pulp of the second primary molar. Because the succedaneous second premolar was congenitally missing, a decision was made to attempt to save thetooth as a functional space maintainer through the growing years, if possible. Note the evidence of internal resorption
at the floor of the pulp chamber.

Ankylosis of the primary teeth which prevents the eruption of the second permanent premolar

4. Post-treatment Evaluation
It is done to evaluate:A. Accuracy of treatment
B. Type and success of pulp treatment
C. Postsurgical
healing
D. Treatment failure.
Dental health professionals must be concerned about any risk the patient may encounter during therapy.
Concern is focused on three primary biologic effects of low-level radiation:
(1) Carcinogenesis,(2) Teratogenesis (malformations)
(3) Mutagenesis.
In general, younger tissues and organs are more sensitive to radiation
Why children are higher risk than adults?• The tissues of the child are in the growth period and are more sensitive to radiation.
• Children have a longer life span with greater susceptibility to tumors.
• The effect of radiation are cumulative.
• Because of their smaller stature children are closer to the central x-ray beam.
• Because of carious activity children may have an increased frequency of radiographs.
Recently, there has been an increased use of beam-positioning devices that have virtually eliminated some technical errors, particularly film cone cuts.
Treatment planning
Advantages of the treatment planning
1. Re-diagnosis at every visit is avoided.
2. Serial appointments can be given on the first day as the patient's treatment needs are already planned in a sequential order.
3. Instruments can be prepared well in advance before the patient's arrival for the treatment.
4. Total fee estimation can be done
Treatment plan must be discussed with the parents and permission taken before performing any treatment on the child
.
Information relating to the following must be given:
Dental need of their child including the treatment as well as the preventive measures.
Amount of time required to perform the treatment.Total cost.
ModificationTreatment planning may be modified during the procedure based on:
• Estimation of cooperation from the patient and parents.
2. Assessment of the condition of the teeth and the oral hygiene.
3. Whether extraction is needed or not.
4. Nature of tooth movement and type of appliance required.
Treatment planning for the routine visits should provide1. age-appropriate oral hygiene instructions.
• 2. Scalling and polishing if the patient need.
• 3. Fissure sealant for the caries susceptible teeth.
• 4. counseling and services like mouthguards to prevent orofacial trauma
• 5. Assessment of malocclusion.
6. required treatment and/or appropriate referral for any oral diseases, habits, or injuries as indicated.
7. Assess speech and language development and
provide appropriate referral as indicated.