Small & Large bowel
د.محمد هشام
1
Small & Large Bowel
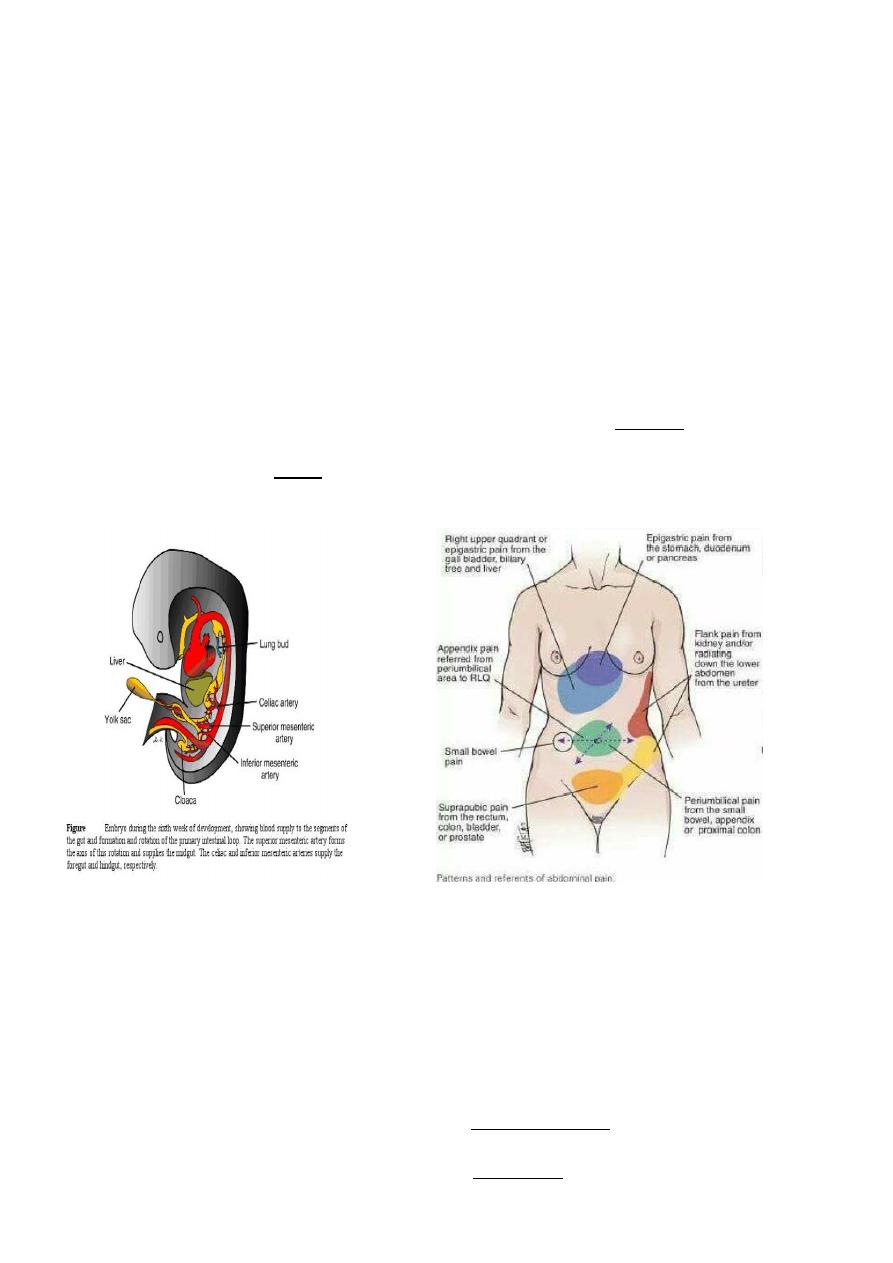
Gastrointestinal tract formed from 3 parts:
Foregut: stomach and duodenum down to the Ampulla of Vater and supplied by Celiac
artery and the visceral pain felt in the epigasrtic region.
Midgut: from the middle of 2
nd
part of duodenum till the junction of middle 3
rd
and the
lat 3
rd
of transverse colon & supplied by superior mesenteric artery & its visceral pain felt
around umbilicus
Hindgut remaining part colon & upper half of anal canal & supplied by inferior
mesenteric artery & Pain felt.
Small Bowel
It may vary from 300 to 850 cm between the duodenojejunal (DJ) flexure to the
ileocaecal valve. The proximal 40 % is referred to as the jejunum; the remainder is the
ileum. There is no clear demarcation between jejunum and ileum, but the small bowel
does change gradually in character from proximal to distal. The jejunum tends to have a
wider diameter and a thicker wall, with more prominent mucosal folds (valvulae
conniventes), while the ileum has a thicker, more fatty mesentery with more complex
arterial arcades. The ileum also contains larger aggregates of lymph nodes (Peyer’s
patches).
The Wall of Small intestine
Mucosa : single layer of columnar epithelium with mucus goblet cells The absorptive
surface area approaches 500 m2 which achieved by the presence of mucosal folds, villi,
and microvilli on the cell surface. Under the epithelium is a thin muscle layer; the
muscularis mucosa.The submucosa is the strongest layer It contains lymphoid
aggregates (Peyer's patches), &The Meissner's nerve plexus is present in the submucosa.
Muscularis propria outer longitudinal, inner circular with Aurbach myenteric plexus.
Serosa: part of visceral peritoneum.
Blood Supply
:
from the superior mesenteric artery, while venous drainage is via the portal venous
system, into which the superior mesenteric vein drains blood rich in nutrients after a
meal. The portal vein drains in the liver . The lymphatic drainage of the small intestine

Small & Large bowel
د.محمد هشام
2
follows the arterial supply. The small intestine has a rich autonomic innervation arising
from the splanchnic nerves, which contribute a dense network of sympathetic fibres
around the superior mesenteric artery and its branches. Referred pain from the small
intestine is usually felt in the periumbilical region (T10).
Physiology Of The Small Bowel
Main function is absorption of fat, protein, carbohydrate ,vitamins and electrolytes,
The jejunum is the principal site for digestion and absorption of fluid, electrolytes, iron,
folate, fat, protein and carbohydrate, Resection of jujenum can be compensated by
ileum but the jejunum cannot compensate resection of terminal ileum. Vit B12to be
absorbed combine with intrinsic factor secreted by stomach then absorbed in the ileum
therefore resection of ileum may produce vit.B12 deficiency.
Colon
Is formed of cecum, ascending colon, transverse colon, desending, and sigmoid
colon, ileocecal valve is a competent valve.Cecum is a blind pouch and the appendix
opens at the junction of tenia coli.Transverse colon join the ascending at hepatic flexure
and the descending at splenic flexure, whih is suspended by Phrenecocolic ligament.The
descending colon continues as sigmoid (pelvic) colon ends at the level of S3 where
rectum begin.Cecum is completely covered with peritoneum. Transverse and (pelvic)
colons completely covered with peritoneum have mese ntery and are mobile. Greater
omentum attached to the antimesentric bordeer of transverse colon .
Blood Supply
Superior mesenteric artery to midgut.
Inferior mesenteric artery to hindgut.
Venous drainage :Superior and inferior mesenteric veins to portal veins
Lymphatic drainage to L.N. alongside of superior and inferior mesenteric vv.
Walls: * Mucosa columnar epithelium with goblet
Submucosa the strongest layer, connective tissue
Muscular layer inner circular& outer longitudinal Taenia coli
Serosa visceral peritoneum.
Rectum
12-15 Cm. In length starts at S3 recto sigmoid junction downward in hollow of
sacrum and ends at anorectal junction at pelvic floor.
* Rectal Ampulla act as reservoir , There are 3 lateral curves in the rectum their
inner aspect form a valve of Houston (on endoscope).
* The rectum has no tenia , haustration nor mesentry.
The upper 1\3 is covered with peritoneum from above & both sides.
The middle 1\3 only covered by peritoneum anteriorly.
The lower 1\3 is totally extra peritoneal.
Posteriorly
the rectum is loosely bound to sacrum by connective tissue (Waldeyer
Fascia) behind it is a plexus of autonomic nerves.
Anteriorly (Denoviller fascia)
separate it from the base of bladder & prostate
in male.
Small & Large bowel
د.محمد هشام
3
Arterial supply:
Sup.
rectal artery from inf.Mesenteric art. ,Middle rectal artery
from internal Iliac art., Inferior rectal from Pudendal art.
Venous drainage
: Sup.
rectal v. to inf. Mesenteric vein to portal
Middle & Inferior.rectal veins to systemic circulation.
Lower rectum and anal canal, are site for porto-systemic collaterals
Lymphatic drainage: Upper
to the Inf. Mesent. lymph nodes & to para-aortic L.N.
Lower
to internal Iliac L.N.
Physiology
main function of the small bowel is absorption. Fat, protein,
carbohydrates, vitamins, water, and electrolytes are all absorbed.
o
With a few exceptions (e.g. iron and calcium), the small intestine absorbs
indiscriminately without regard to body composition.
o
To be absorbed, vitamin B12 combines with the intrinsic factor secreted by the
stomach. It is then absorbed in the distal ileum. Resection of a long segment of the
distal small intestine is, likely to produce vitamin B12 deficiency. intestinal
secretions present a total of 5-9 L/day, but only 1-2 L pass the ileocaecal valve to the
colon.
Function of colon & Rectum:
Absorption of water and sodium to concentrate the
waste products. This is mainly a function of the right side of the colon.
1. The left side of the colon acts as a reservoir for solid faeces till ldefaecation.
2. Mucus secreted by the mucosa acts as a lubricant. Potassium and bicarbonate are
also secreted in small quantities. Excessive diarrhoea may result in potassium and
bicarbonate loss and metabolic acidosis.
Preoperative preparation for elective surgery
Anastomosis in colon is liable for disruption, leakage and peritonitis, causes:
1.Highly infective contents of both aerobic and an aerobic bacteria
2.constant gaseous distension 3.incomplete serous coat
4. peculiar blood supply where terminal arteries poorly connect each other
Preoperative preparation for elective surgery Improving nutritional status
Bowel preparation : the risk of leakage & sepsis decrease much if bowel is clean .
Methods of preparation:
Mechanical preparation:
A. Standard preparation: 1. Non residue diet for 4 days before operation
2. Enema and mild laxative for
2-3
days before surgery.
B.Rapid preparation. Another method performed 1 day before suegery.
1.Whole gut irrigation using 2-4L/hour of a balanced crystalloid solution passed via
a nasogastric tube until the patient passes clear fluid per rectum.( not for bowel obst.
Or with heart disease)
2.Mannitol 1 litre of flavored mannitol given orally.
Chemical Preparation: Intestinal antiseptics administered orally help to reduce
the density of colon bacteria. A combination of neomycin and metronidazole
(Fiagyl) for two days will cover the Gram negative bacilli and the anaerobes
which are normally resident in the large intestine.
Prophylactic Parenteral antibiotics: systemic antibiotic administered immediately before
operation & continued Postoperatively for 1 day (Peri-Operative antibiotic prophylaxis)
usually Cephalosporin or an Aminoglycoside with either flagyl or Clindamycin.
Operative Procedure
Small & Large bowel
د.محمد هشام
4
Resection : extent of resection is governed by art. Blood supply & disease process.
In surgery for malignancy it is essential to remove draining lymph nodes .
Divisions of peritoneal attachments allow adequate mobilization of bowel.
Anastomosis: For a successful anastomosis the two bowel ends should be
adequately vascularized, and should be sutured without tension. An intestinal
anastomosis can be done by one of two methods.
1-By hands two layers: 1
st
interrupted full thickness & seromuscular, defect in
mesentery closed.
2- By stapler which is rapid and coasty.
Emergency Surgery: in patient with obst.,perforation, toxic dilatation, bleeding from
colon emergency surgery might be needed
In critical ill patient with obst. Temporary colostomy done resection postponed
If patient condition permit resection ( but not prepared )&dealing with according to site:
1.ileotransverse anastomosis in right colon resection other parts of colon primary .
anastomosis abandoned due to high leakage possibility,
2. proximal colostomy & distal end closed left in abdomen (Hartman procedure)
3. both ends brought to skin proximal as colostomy & distal mucus fistula .Later on
after few weeks elective closure with preparation.
Intestinal Stoma
Ileostomy indications:proctocolctomy for ulcerative colitis or familial polyposis coli.
Conventional ileostomy:
The stoma is performed so that the nippl of ileostomy protrude from the skin leading to
direct delivery of of irritant small bowel contents to the appliance(it is incontinent).
Continent Ileostomy:
Done by fashioning a valve with an underlying reservoir (Koch Pouch) which the
patient regularly evacuate by passing a tube.
Colostomy: Opening of the colon to the skin.
Indications of Temporary Colostomy
1.To relieve large bowel obstruction in patients with:
a.
High anorectal malformations.
b.
Hirschsprung's disease.
c.
Inflammatory stricture.
d.
Carcinoma of the colon.
After the obstruction
is relieved, the
colon is prepared and the cause is
corrected. Later,the colostomy is closed.
This is called three-stage
management of acute colon obstruction.
2. Injuries of the colon. The injured segment is either
exteriorized as a colostomy, or is closed and a
proximal diverting colostomy is performed.
3. To protect a distal doubtful colonic or rectal anastomosis.
Small & Large bowel
د.محمد هشام
5
Permanent Colostomy
1.
After abdomino-perineal resection.
2.
lrresectable carcinoma of the large bowel with obstruction.
3.
Incurable cases of anal incontinence.
4.
High anal fistulae that is not amenable to surgery.
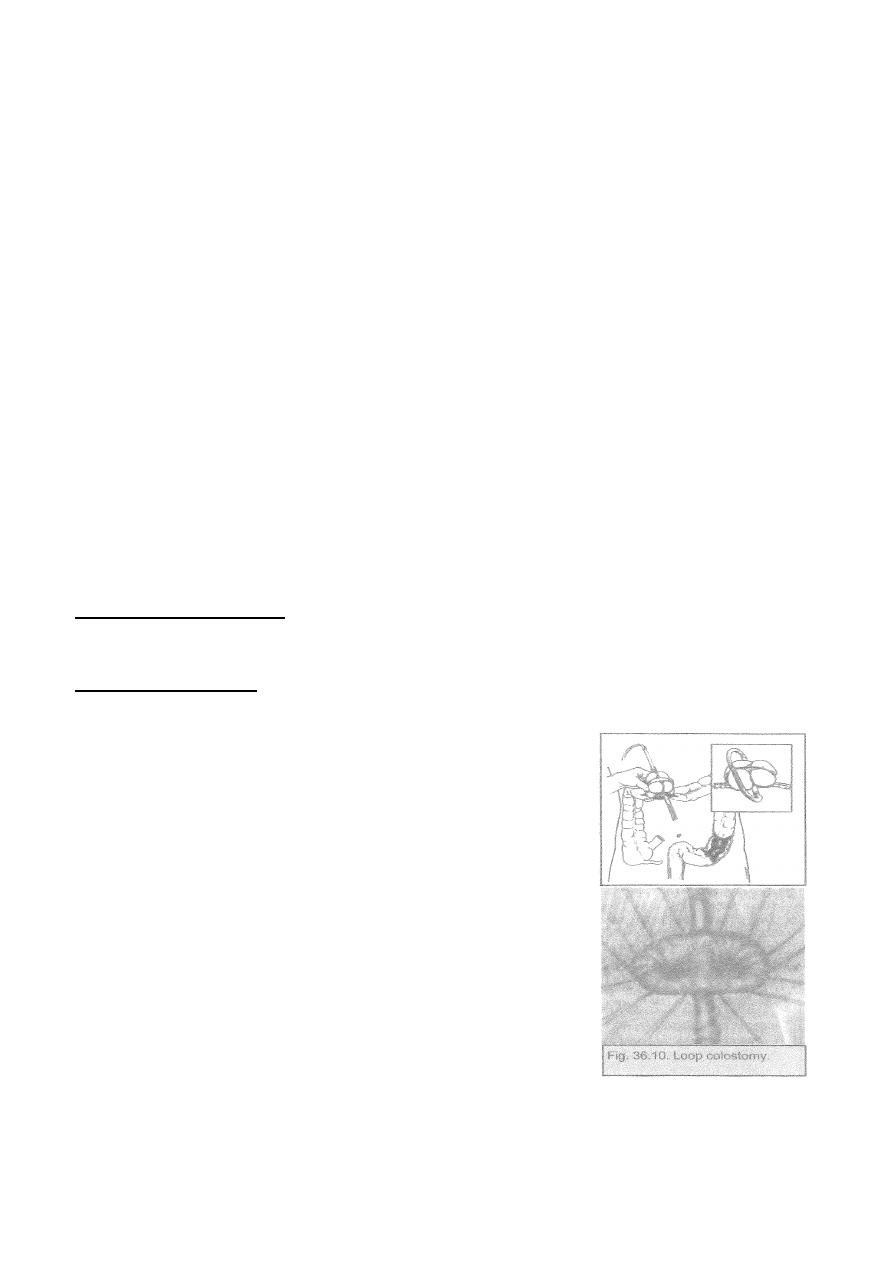
1. Loop colostomy is usually temporary and is usually done in the right side
of the transverse colon brought to the surface, fixed to the abdominal wall,
opened along one of the taeniae coli, and then stitched to the skin. A rod is
passed beneath the loop to prevent retraction, and is removed after one
week.
2. End colostomy may be permanent or temporary. It is commonly
.constructed in sigmoid colon left colon
3. Cecostomy :for temporary decompression of the colon and done by insert of
wide bore tube in to the cecum.
Colostomy complications
1.
Prolapse.
2.
Retraction.
3.
Necrosis of distal end.
4.
Stenosis of the orifice.
5.
Colostomy hernia. through the anterior abdominal all opening beside the
colon end, or internal when the surgeon fails to close the space lateral to
the exiting colon between it and the parietal peritoneum.
Intestinal Trauma:
The small and large intestines are frequently injured, either alone or in
combination with other intra-abdominal viscera. The prognosis after treatment
of intestinal injury largely depends on these associated injuries. Colon injuries
are more dangerous than those of the small intestine because of the magnitude
of intra-abdominal contamination.
The intestine may be injured by:
1.
Blunt abdominal trauma as in road traffic accidents (RTA) or blows to the
abdominal wall. Presence of seat belt injuries should direct attention to
the possibility of intestinal injury.
2.
Penetrating trauma as stabs and bullets. High velocity missiles are more
damaging than low velocity ones and stabs. Indirect trauma, e.g., blast
injuries are known to affect the colon.
3.
Iatrogenic injury is increasing with the rising popularity of invasive
investigations.
Examples:
*The duodenum may be
injured
during
an
attempt
at
endoscopic sphincterotormy. *The colon may also be injured with
colonoscopic diatherm.
Small & Large bowel
د.محمد هشام
6
Types of Injury:
1. Contusion and haematoma.
2. Rupture which may be complete or incomplete and single or multiple.
3. Tears of mesentery or mesenteric vessels resulting into haematomas, and
gangrene of the affected bowel segments.
Sequela:
1. Peritonitis occurs due to the escape of intestinal contents into the peritoneum.
2. Internal haernorrhage. With intestinal injuries bleeding is less of a problem
than peritonitis.
3. Hypovolaemia and septic shock.
4. Paralytic ileus.
5. Injuries may heal by strictures and massive adhesions by intestinal
obstruction.
Clinical Picture:
1-History of trauma.
2-Abdominal pain at site of trauma which spread to all abdomen.
Signs:
General : tachycardia, fever, & hypotension. And Local:
1.
signs of injury: bruises, inlet or outlet of a bullet, stab .
2.
Tenderness with rebound tenderness.
3.
Loss of liver dullness due to free air in peritoneum .
4.
Distension due to developing ileus.
5.
Shifting dullness because of free intraperitoneal fluid.
6.
Frank peritonitis due to perforation nearly or late.
Investigations:
1.Clinical .
2.Laboratory tests (leukocytosis , & hemodilution)
3.Radiology
Plain abdominal X-Ray may show free air under diaphragm or multiple fluid
levels, due to ileus, bullet & shell or fracture may be seen.
Ultrasound or CT scan reveals hematoma or collection.
4.Needle tap, diagnostic peritoneal lavage (DPL) may show free blood, bile ,or
intestinal contents.
Treatment: Surgery (laparotomy)
Preoperative:
1. Anti-shock measures.
2. Antibiotic coverage Cephalosporin & Metronidazole.
3. Tetanus toxoid booster dose.
4. Insertion of nasogastric tube & urinary catheter.
Operation:
Midline incision full exploration 1
st
bleeing managed then bowel injury.
Priorities of multiple trauma management should be followed
1. Small bowel and Right side of colon :if tinny small injury suturing is enough.
bigger need trimming & suturing , big wounds , big segment need resection &
anastomosis .
Small & Large bowel
د.محمد هشام
7
2. Transverse colon and left colon: localized injury exteriorized as colostomy or
injury sutured and protective proximal colostomy closed after 1 month or
resection of injured segment with proximal colostomy & distal mucous fistula or
Hartman's procedure, closure after month, good peritoneal irrigation with N.S.
Intstinal Fistula:
1. 80% of external fistulae develop after an abdominal operation. The cause
is either: *.Unrecognized intestinal injury.
*.Failure of an intestinal anastomosis. Causes of this failure include:
i.
Poor vascularity.
ii.
Anastomosis under tension.
iii.
Anastomosis in the presence of sepsis.
iv.
Distal obstruction.
v.
Lack of proper surgical technique.
vi.
Presence of a specific pathology as Crohn's disease.
vii.
Generalized diseases that impair healing, e.g., hypoproteinaemia.
2.
Other Causes:
Congenital as patent vitello intestinal duct through the umbilicus
Abdominal trauma
Inflammatory bowel disease (Crohn's) colonic diverticulitis, radiation enteritis
which produce internal and external fistula .
Malignant tumour.
Pathology:
Fistula is abnormal communication between two epithelial surfaces. It is lined
by granulation tissue but sometimes it is lined by epithelium.
1.
Intestinal fistulae are classified into:
* internal connect the intestine to hollow viscera ( b l a d d e r , v a g i n a , e t c . )
* external when it is connected to the skin.
External fistulae are low-output fistulae that discharge less than500 ml/day,
and high-output more than 500 ml/day. amount of fistula output has an
important metabolic effect.
According to origin in intestine.& by the nature of discharge
Bile stained duodenum, jejunum.
Greenish fluid ,fecal fluid ileum, cecum.
Fecal material distal colon .
complications:
1. Metabolic effect: high output fistulae lead to loss of intestinal contents with
malabsorption & catabolic state, the metabolic effect include:
a.
Dehydration.
b.
Malnutrition, e.g., hypoalbuminaemia.
c.
Electrolyte disturbances as hypontraemia, hypokalaemia.
d.
Acid-base disturbance causes acidosis.
2. Sepsis If fistula track is not effectively walled off, and enteric contents
escape producing an intraperitoneal abscess.
3. Skin irritation & maceration due to continuous flow of intestinal contents
.
Management:
The great majority of intestinal fistulae heal spontaneously if sepsis is
Small & Large bowel
د.محمد هشام
8
treated, the nutritional status is maintained and distal obstruction is relieved.
1.Resuscitation &skin protection :
I.V.fluid ,blood,correct electrolyte &skin protection
2Nutritional support.:
TPN for high output, entral feeding for low output fistula.
3.
Investigations
&
treat sepsis: to know: level of fistula ,bowel disease, distal
obstruction ,sepsis by:
1.clinical assessment,
2.fistulography &.Ba follow through,
3.U/S or CT scan for abscess to be treated or aspirated.
4.Suppression of intestinal secretion by Somatostatin.
Definitive Treatment
External Fistula:conservative treatment succeeds mostly.
Surgery :If no improvement after 6-8 weeks , Distal obstruction , Active disease
Malignancy or Crohn's , Total discontinuity of bowel ends , Mucocutaneous continuity
, Excision of the fistula correct pathology .
Internal Fistula: spontaneous closure rare. Many internal fistulae need no correction.
Surgery indicated :
Internal fistula to urinary bladder.
Fistula Bypassing long segment of bowel causing malabsorption
A is a blind pouch that is continuous with the lumen of a hollow viscus (gut or
urinary bladder).
Diverticula can occur anywhere in the bowel from the duodenum down to
the sigmoid colon. common ones, however, are diverticula of the colon and
Meckel's Diverticulum:
It is the most prevalent cong. Anomaly of of gastrointestinal tract .it is caused by
persistant patency of proximal part of vitello intestinal duct of embryo the abnormal
persistence of the duct may have anomalies as well:
A fecal fistula connecting the ileum with the umbilicus, caused by persistent
patency of the whole vitello-intestinal duct
A fibrous band remaining
obliteration of the duct. An enterocyst that results
from the persistent patency of the middle part of the duct
An umbilical extremity of the duct is everted producing an umbilical polyp
Pathology
Meckel's diverticulum is a true diverticulum that incorporate whole layers of the bowel
wall. It lies on antimesenteric border, and has its separate blood supply via a branch of
sup. Mesenteric artery .It may contain ectopic mucosa and sometimes pancreatic and
colonic cells. Rule of 2-3as an approximation :
It occur 2-3% of population It averages 2-3 inches in length
It situated in ileum 2-3 feet from the cecum
Symptoms are due to complications which occur in about 2-3% of affected people
Complications:
1.
Intestinal obstruction is the commonest complication. be due to
a.Intussusception: The ectopic mucosa at the base of the diverticulum
acts as a foreign body and forms the apex of an ilea-ileal
intussusception.
b.Pressure on an intestinal loop by a fibrous band or rotation of the
Small & Large bowel
د.محمد هشام
9
ileum around its axis (volvulus).
2. Incarceration in an inguinal or a femoral hernia is called Littre's hernia.
3. Peptic ulceration and bleeding are caused by the ectopic gastric mucosa,.
Bleeding from Meckel's diverticulum is the commonest cause of lower
gastrointestinal bleeding in children.
4. Acute diverticulitis is similar to acute appendicitis. Gangrene and
perforation may occur and leads to peritonitis .
Clinical Picture:
1. Accidental at surgery.
2. Complication like I.O.,painless rectal bleeding.
3. Acute abdomen like in acute appendicitis
Treatment:
1. Symptomatic resection is indicated.
2. Accidentally discovered at surgery
resection is indicated in children & young adults & in those with an
attached band..
in patient over 40 years old NO need for surgery
Diverticular disease of the colon
Aetiology:
Lack of fibers in nthe diet leading to chronic constipation & increased
intra luminal colonic pressure,increase muscle spasm may play a role
.
Pathology:
it is a pulsion diverticulum of the colonic mucosa through the circular
muscle layerat the points of entry of the blood vessels between the tenia coli on the
anti mesenteric border.
The Sigmoid colon is the most affected part, but any part could be affected except the
rectum.
Complication :
1.
Acute Diverticulitis:
Is inflammation of one or more of the diverticula
secondary to obstruction of the neck.
2. Perforation leading to localized or generalized peritonitis.
3. Recurrent attacks of inflammation.
4. Bleeding due to erosion of blood vessels.
5. Stricture chronic distension I.O.
6. Fistula formation ( colovesical , colointestinsl.)
Clinical Picture:
1. Age above 40 years.
2. Asymptommatic recurrent attacks of lower abdominal pain, distension.&
Flatulence .
3. Acute Diverticulitis mimic acute appendicitis but on the left side . It may
be complicated by pericolic abscess & peritonitis.
4. Chronic diverticulitis, recurrent attacks of blood and mucus per
rectum,palpable tender mass in LIF mimic colon cancer.
5.
Fresh bleeding per rectum (massive bleeding) should be differentiated
Small & Large bowel
د.محمد هشام
10
from angiodysplasia by angiography, Ca colon bleeding
not massive.
Investigation:
1. Ba enema.: in early stage show saw teeth appearance ,fully developed
diverticula will be visualized, In acute case Barium enema is
contra-indicated .
2. Sigmoidoscopy: detect the mouth of the diverticula.
3. CT scan reveals thickenings of the wall ,peridiverticular abscess.
Treatment:
1. In stage of diverticulosis high fiber diet , antispasmodic for colic
2. Acute diverticuliculitis treated as appendicular mass.
3. If peri-colic abscess drainage should be done.
4. Generalized peritonitis laparotomy, resect the affected part with
colostomy,
Hartmann's
procedure
,peritoneal
toilet
and
drainage
,exteriorization of perforated segment is less successful option.
5. Chronic diverticulitis colectomy after adequate preparation.
6. Bleeding in majority of cases stop spontaneously with conservative treatment
,if continued & massive angiography and urgent colectomy.
Inflammatory Bowel Diseases:
o Ulcerative Colitis ,Crohn's Disease ,(Main Diseases)
o Others : schistosomal colitis, ileocecal T.B., amoebic colitis, typhoid
enteritis.
Ulcerative Colitis:
Inflammatory disease of the colon characterized by ulcerations
Aetiology:
unknown, immunologic, genetic, & environmental factors could be causes.
Pathology:
1 . The disease begins at the dentate line of the anal canal and extends
proximally.Extension is continuous with no skip areas of normal bowel.
The extent of the disease varies from rectal involvement alone
(proctitis), to w hole colon and rectum affection (pancolitis )
2. Unlike Grahn's disease, only the mucosa and submucosa are involved.
3. The mucosal affection varies from granularity to extensive ulceration.
4. The characteristic histological feature is the formation of crypt
abscesses in the depths of the glandular tubules with surrounding
inflammation.
5. The abscesses fuse to form ulcers.6 Pseudopolyps are likely to be found.
Complication:
Intestinal:
1
.Toxic mega colon 3-5% 2.Hemorrhage
3.Colon cancer: patient with pan colitis more than 10 years at a higher risk
Extra intestinal
include a1ihritis, uveitis, cholangitis, liver cirrhosis, and skin lesions as
pyodemia gangrenosum, and erythema nodosum.

Small & Large bowel
د.محمد هشام
11
Clinical Picture:
1.
The disease is more common in females
.
2. Age 3
rd
4
th
decade
3. Presented with watery diarrhea mixed with blood,pus,mucous & tenesmus
4. Pain, fever, weight loss, & dehydration'.
5. Remission & relapse.
Toxic mega colon
1 .Serious complication, severe diarrhea, with p[assage of blood &
mucus,and the patient is very toxic, high fever 39 – 40c .
2 Abdominal examination reveals severe abdominal distension due to
markedcolonic atony need urgent treatment it is Fatal
Treatment
Medical treatment:
1 Correction of anemia and hypokalaemiabyb proper dieting, supplementary
vitamins & minerals
2 Sulphasalazine 2-6 gm/day according to severity. Salazopyrine is a
combination of Sulpha and salicylate is an effective therapy.
3 Attacks of exacerbation treated by corticosteroid either systemic or by enema
in localized cases to rectum.
4 Metronidazole also used.
Investigation
1.Laboratory finding:
Anemia, Leukocytosis, hypoproteinemia, & hypokalemia in severe cases.
2.Ba enema:
Mucosal irregularity and ulcers, colonic shortening and loss of haustration.
3.Colonoscopy:
Ulcers can be seen and biopsy taken.
Colonoscopy, biopsy ,& Ba enema are contraindicated in toxic mega colon.
Surgical treatment:
Indications:
1. Failure of medical treatment
2. Development of complications as toxic mega colon with perforation (Urgent)
or cancer
3. Long standing pancolitis where biopsies show dysplasia.
4. Stricture formation.
Surgery:
Excision of whole colon and rectum [panproctocolitis] with permanent
ileostomy.
Colectomywith ileo-rectal anastomosis, follow up for rectum for fear of
developing cancer
Proctocolectomywith distal rectal mucosectomy with ileal pouch and ileoanal
anastomosis
Small & Large bowel
د.محمد هشام
12
Crohn's Disease
It is idiopathic, chronic transmural inflammatory bowel disease that can involve any
area in G.I.T.
Aetiology
Unknown, heredity can play role; focal ischemia is postulated as cause.
Pathology
1. The commonest site is distal ileum hence the old name is Regional Ileitis, any paet
from the mouth to the anus can affected, colon next affected, followed by anal canal.
2. Chronic disease with granuloma formation
3. The affected bowel segment the wall from mucosa to serosa thickened,the
mesentery thickened and contains large lymph nodes.
4. Skip lesion area affected between two normal areas.
5. In long standing cases multiple fissures occur between which the mucosa is
edematous giving a coble stone appearance.
6. Microscopically there is non caseating granulomatous infiltration of the lymphatics
of submucosa with presence of giant cells, in late cases fibrosis extends in to and
obliterates the submucosa.
Complications:
Intestinal
:
1. stricture of small bowel intestinal obstruction.
2. Abscess & fistula to other loop, bladder, vagina, skin.
3. Perianal abscess, anal fistula & fissure.
4. Malabsorption in extensive disease.
Extra Intestinal:
Ocular, joint, skin & hepatobiliary.
Clinical Picture :
Age 2
nd
to 4
th
decades, male = female.
Symptoms
diarrhoea, abdominal pain, weakness, weight loss, anorectal disease.
In old standing cases the patient present with intestinal obstruction.
Signs include: Anemia, malnutrition & possibly a mass in R.I.F.
Investigations:
Ba meal & follow through for small bowel & Ba enema for colon disease.
Radiography shows stricture, skip lesion, cobble stone appearance, internal or
external fistula, the finding of a narrowed terminal ileum is known as String Sign of
& Kantor .
Colonoscopy & Biopsy of large bowel lesions to prove diagnosis
Biopsy of suspected anal fissures & fistula.
Treatment:
Low residue diet, high protein, high caloric diet with supplementary vitamins
& minerals.
Antispasmodics for pain
Corticosteroid & antibiotic (Sulphasalazine or Flagyl) are also given.
Immunosuppression like Azathioprim drug.

Small & Large bowel
د.محمد هشام
13
Surgery in Crohn's disease:
Is reserved for complications
1. The tendency is to perform limited resection of the affected area ,removal of big
segment may lead to malabsorption.
2. Localized stricture need surgery.
Intestinal T.B
.: it is in two forms
1. Ulcerative: secondary to pulmonary TB due to swallowing of bacilli. Multiple
ulcers in terminal ileum, the long axis of ulcer lie transversely perforation is
rare but stricture is possible.
Clinically: diarrhoea, abdominal pain, weight loss, in chronic cases may present
with intestinal obstruction
Treatment: in early cases AntiTB ,if intestinal obstruction surgery needed
2. Hyperplastic Ileocaecal T.B.:
Due to ingestion of bacilli by patient with high resistance, the site is the
ileocaecal region, there is thickening of the wall with narrowing of the lumen
with lymph nodes involvement which may caseate, abscess, and fistula formation
are rare, if untreated lead to Intestinal obstruction .
Clinically: -abdominal pain, intermittent diarrhea, or mass in RIF with
general ill health.
- Ba-enema show narrowing of the lumen of affected segment
Treatment :Anti T.B., Right hemi colectomy in cases of obstruction and if
malignancy not excluded.
Surgical complication of Typhoid and Para Typhoid
:
1 Intestinal haemorrhage as a result of ulceration of the affected Peyer's
patches in the lower ileum. The ulcer is parallel to the long axis of the
gut. Bleeding usually occurs 2-3 weeks after the onset of the disease. It
usually presents as passage of dark blood per rectum, but may be bright
red if bleeding is profuse.
2 Perforation of a typhoid ulcer may occur around the third week
with resulting peritonitis. The condition calls for urgent exploration
under cover of chloramphenicol. Pus is evacuated, and either the
perforation is closed or the diseased ileal segment is resected.
3 Acute non-calcular cholecystitis.
4 Chronic cholecystitis (carrier state).'
5 Deep venous thrombosis of the lower limbs is a complication of
prolonged recumbence.
Bilharzial Colitis
: The disease often affect young male
Aetiology:- Infestation by Schistosoma Mansoni & less commonly by S.haematobium
Pathology: * Site sigmoid colon and rectum.
Chronic inflammatory cells surround the deposited ova leading to the
formation of Bilharzial granuloma .
The disease occur in two forms:
Small & Large bowel
د.محمد هشام
14
1/Pathology in mucosa and submucosa, the mucous membrane become
odematous, with hypertrophy, excess bleeding and mucous secretion,
multiple polyps & ulceration
2/Diffuse involves the whole colon and mesentery.
* The condition is not precancerous & does not produce stricture.
Possible Complication:
Anemia due to blood loss
Hypoproteinemia due to chronic protein loss
Partial rectal prolapse
Prolapse and strangulation of polyps
Clinical:
o Tenesmus, diarrhoea, blood & mucous in stool.
o Weakness, dyspepsia, colic, pallor, clubbing of finger in chronic cases .
rectal examination reveal multiple polyps.
o Mass in LIF due to thick wall sigmoid colon.
Investigations:
Stool analysis blood and mucous, ova.
Urine associated with renal bilharzial affection
Blood picture may show anemia
Liver function test hypoalbuminemia.
Sigmoidoscopy mucosal changes, fresh biopsy, scrubbing of ulcer may
show viable ova.
Ba-enema multiple round filling defect due to polyps.
Treatment:
Antibilharzial drugs (Oxaminquine ,or praziquantel) are effective.
Polyps colonoscopy polypectomy
Surgery: excision of affected segment rarely needed.
Intestinal Ischemia:
Acute & Chronic
Chronic type due to narrowing of Superior mesenteric artery and sometimes
celiac artery due to atherosclerosis.
Aetiology
Atherosclerosis is the main cause narrowing of sup. Mesenteric artery.
Rarely the celiac axis is compressed by median arcuate ligament.
Clinical:
1. Post prandial pain 15-30 min. after meal last for 1 hr.( Abdominal Angina)
2.Afraid of eating .
3. Upper abdominal bruit is heard, signs of atherosclerosis of arteries.
Investigation:
Exclude other causes of abdominal pain by U.S and endoscope.
Confirm the narrowing of the vessel by Aortography which show narrowing and
collaterals.

Small & Large bowel
د.محمد هشام
15
Treatment:
By end arterectomy (coring out of thickened intima) or by Dacron graft to the
Sup. Mesenteric artery.
Median arcuate ligament compression is treated by division of the ligament.
Acute Intestinal Ischemia
Serious surgical emergency (fatal)
It is due occlusion of one or more of mesenteric vessels .it is usually the
superior mesenteric artery and vein which is occluded , it lead to acute
ischemia of large segment of intestine, small segment could be affected due to
local ischemia.
Aetiology :-
1. Mesenteric artery embolism from heart
o
Atril fibrillation
o
Mural thrombus
2.Mesenteric artery thrombosis:- atherosclerosis complicated by embolism.
3.Mesenteric venous thrombosis: idiopathic or due to
a) Portal hypertension
b) Intra abdominal sepsis
c) Hyper coagulable state
d) Intake of contraceptive pills
Pathology
The most sensitive part to ischemia is mucosa within three hours of obstruction
mucosa slough, ulcerate & bleeds in lumen bacteria get access to blood stream due
to loss of mucosal barrier.
Within few hours the whole wall involved with exudation of serosanguinous
fluid to peritoneum .there is significant blood loss.
The intestine become gangrenous lead to perforation and peritonitis
Dead bowel no peristalsis lead to obstruction and distension due to paralytic
ileus
Clinical picture:
Severe acute abdominal pain not responding to analgesic or nasogastric suction
Vomiting, bleeding per rectum.
Hypovolemia due to blood loss, peritonitis due to perforation which lead to shock
with rigid tender abdomen later on distension.
Differential diagnosis:
Acute pancreatitis severe pain with vomiting, minimal local sign, later on
shock. Managed conservatively while in mesenteric occlusion urgent surgery
Intestinal strangulation

Small & Large bowel
د.محمد هشام
16
Investigations
Clinical, patient atherosclerotic with cardiac arrhythmia.
Blood picture (leukocytosis, anemia, due to blood loss).
Serum amylase high in 50% but not as acute pancreatitis.
Palin x-ray air fluid level in proximal loop, intramural gas in intestinal wall,
and portal vein due to necrosis.
Angiography may be diagnostic , its use is controversial.
Treatment
: urgent surgery.
Preoperative
Blood and i.v.fluid
Antibiotics and nasogastric suction
Laparotomy :
Gangrenous segment resected with ileostomy (double barrel)two ends out.
Resection with anastomosis may be done with 2
nd
look operation after 24
hours.
Restore arterial flow by embolectomy or end arterectomy or bypass
Mesenteric venous thrombosis clots in mesenteric vein, gangrene excised.
Heparin to all patients.
Prognosis
High mortality 30-50%
resection of up to 70% of small bowel can be done without major
nutritional consequences, short bowel syndrome malabsorption.
Early on TPN later on to Oral till bowel accommodate.
Ischaemic Colitis
50-70 years, chronic vascular disease of mesenteric vessels.
Splenic flexure mostly affected pain and bleeding per rectum
Plain x-ray show thumb prints due to odematous mucosa.
Either complete resolution or gangrenous with perforation and peritonitis,
sometimes stricture.
Treatment: conservative, I.V. fluid, analgesia, antibiotic, surgery for
complication.
Intestinal Tumors:
Small bowel tumors are rare.
Benign tumors cause intussusception or may bleed.
Adenoma, sub mucous lipoma, leiomyoma.
jegher's syndrome consist of:
*Multiple familial intestinal hamartomatous polyps mainly affecting jejunum.
*melanosis of oral mucous membrane & lips.
*the disease is not pre-cancerous, only complicated polyps require removal or
excision of the affected intestinal segment.

Small & Large bowel
د.محمد هشام
17
Malignant Tumors:
Non Hodgkin Lymphoma
Adenocarcinoma
Carcinoid tumors of the small intestine which is less common than that of the
appendix but tends to be more malignant.
Colorectal tumors:
Benign Tumors: usually for polyps
Epithelial:
- Neoplastic adenoma solitary or multiple (Familial polyposis & Gardner synd.)
-hamartomas
-juvenile polyps solitary or multiple.
Mesenchymal : lipoma , leiomyoma or hemangioma may project as polyp
Malignant tumors:
Primary:-carcinoma, carcinoid & sarcoma.
Secondary:- These are the result of direct invasion of nearby malignant tumors.
Familial Polyposis Coli (FPC)
It is autosomal dominant disease.
Only the affected persons with polyps can transmit the disease, male>female , the
disease transmitted to 50% of children of diseased persons.
Pathology:
The colon & rectum full of polyps {more than 100} sessile or pedunculated, the
sigmoid colon and rectum are common site.
If left untreated carcinoma develop in 100% of cases in 5
th
decade, size polyp is
important more than 2 cm. villous adenoma has higher risk of malignancy.
Gardner's syndrome: is FPC in addition there are polyps in the rest of GIT,
Osteomas of the mandible and skull. Cysts soft tissue tumors, and desmoid
tumors of abdominal wall.
Clinical Picture:
Patient discovered 10-15 years old.
Common symptoms diarrhoea, abdominal pain, and bleeding.
Investigations:
Ba-enema:- Multiple round filling defects throughout the colon and rectum.
Sigmoidoscopy & colonoscopy with biopsy.
Treatment:
Pancolectomy with permanent ileostomy is the standard treatment.
The rectum is spared and in ileoproctostomy with endoscopic fulguration of the
remaining rectal polyps with lifelong surveillance of the rectum.
Proctocolecctomy with distal rectal mucosectomy ileal pouch is fashioned to
act as reservoir and anastomosed to ileum.
Family should periodically be examined by colonoscopy and similarly treated if
they developed polyps.

Small & Large bowel
د.محمد هشام
18
Carcinoma of Colon and Rectum
:
It is one of the commonest carcinoma in human being.
Age 50 -70 years.
Aetiology:-
Solitary villous adenoma.
Familial polyposis coli and Gardner's Syndrome,risk of conversion to malignancy
is 100% if un treated ,cancer is more prone to develop in large adenoma more
than 2 cm.
Ulcerative colitis, pan colitis with more than 10 years duration, the risk is high.
More common in west due to lack of high fiber diet & increase animal fat.
Uretro-colic anastomosis.
Pathology:
Microscopic picture:
Histology : adenocarcinoma from columnar epithelium.
Well, moderately or poorly differentiated tumor.
Sometime a colloid structure occur in younger patient and poor prognosis.
Gross Picture:-
65% in rectum & sigmoid.
10% In caecum.
The remainder distributed all over the colon, Multiple tumors in 5% of cases.
Gross types:-
Cauliflower- like polypoid variety
Ulcerative type
Obstructive type {strictures} in sigmoid
Spread :
Direct to adjacent organ (Urinary Bladder).
Lymphatic spread to sup & Inf. Mesenteric nodes ,to preAortic LN.
40% with nodal involvement when come to surgery.
Blood stream to liver, 20%of patient coming to surgery.
Trans peritoneal spread to peritoneal nodules and ascites.
Staging:- Duke's staging:-
Stage A a growth is limited to bowel wall.
Stahge B growth extend outside the bowel wall but no metastases to L.N.
Stage C there is 2
ndry
deposit in regional lymph nodes.
* C1 local para rectal or paracolic lymph nodes alone are involved
*C2the nodes accompanying the supplying blood vessels affected .
* Stage D there is distant metastasis.
Small & Large bowel
د.محمد هشام
19
Complication:
1. Intestinal Obstruction in 20% of cases especially in left hemi side due to narrow
lumen, solid stool, obstructive variety of tumor.
2. Perforation leads to enterocolicor vesicocolic fistula.
3. Bleeding chronic bleeding, massive bleeding.
4. Liver Failure as complication of metastasis , Ascites.
Clinical Feature:
Carcinoma of rectum more in male, carcinoma of cecum more in female.
Clinical features depend on location of tumor, its size and the presence of
metastasis.
Right Side Colon Cancer
The usual presentation is anemia, loss of weight, with anorexia (3A).
Recurrent attacks of RIF pain.
Mass in RIF
Rarely intestinal obstruction.
Left Side Colon Cancer
Changes in bowel habits, constipation with diarrhoea.
Large bowel obstruction , acute or subacute or chronic large bowel obst.,
There is constipation, severe abdominal distension, but no vomiting ca. of
sigmoid is a common cause of I.O. in elderly.
Bleeding per rectum, not massive.
Mass in LIF or left side of the abdomen due to tumor or sometimes impacted
fecal material prior to obstruction.
Rectal Cancer:
Rectal bleeding which is usually (slight)
There may be tenesmus{painful incomplete evacuation}& passage of mucous
The tumor is usually painless unless it has spread outside the rectal wall or
infiltrated the anal canal.
Digital rectal examination allows palpation of lesions that lie within 10cm of the
anal verge. Higher tumor revealed by sigmoidoscopy.
Investigation:
1. Blood Picture reveal microcytic hypochromic anemia
2. Sigmoidoscopy and Biopsy, any patient with bleeding per rectum above 40yrs,
sigmoidoscopy should be done, colonscopy for higher lesions.
3. Ba-enema show irregular fixed filling defect, annular type show stricture ,even in
palpable rectal cancer, contrast radiography is useful to exclude second higher
tumor.
4. To detect spread liver function tests, abdominal U/S or CT scan and CXR are
done, IVU if tumor near the bladder or urethra.
5. CEA is tunuor marker it is high in colorectal cancer ;but not specific, it is of
prognostic value, to detect recurrence (increase after treatment).
Small & Large bowel
د.محمد هشام
20
6. For patient with intestinal obstruction plain X-ray of the abdomen , blood
picture, blood urea, and Electrolyte are needed.
Treatment:
General principles:
Radical resection is the only curative measure.
Inoperable tumor resection also offers the best palliation.
Treatment depends on whether the tumor present with acute I.O. or not
Inoperability can be judged before surgery for example the presence of liver
secondaries by U/S.
Others may prove inoperable during exploration because of liver secondaries,
peritoneal nodules, or fixation of the tumor to important irremovable structures.