Fractures Of The Femoral Neck
Commonest site of fractures in the elderlyThe typical presentation: Caucasian women in their seventh and eight decades
Risk factors :- Note that these are factors for osteoporosis
Age : 7th and 8th decade.
Sex: female (menopause).
Nutritional: malnutrition, alcoholism.
Disuse: stroke CVA.
Chronic medical disease: DM, TB.
Incidence of Osteoporotic fractures
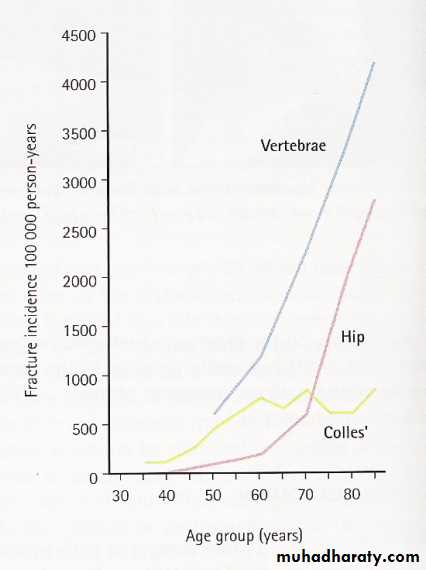
Mechanism of injury:
Fall directly on the greater trochanterIn Osteoporotic people less force is needed (catching a toe in the carpet and twisting the hip into external rotation)
Preceding stress fracture
In young (Fall from a height or RTA)
Pathological Anatomy and Classifications:
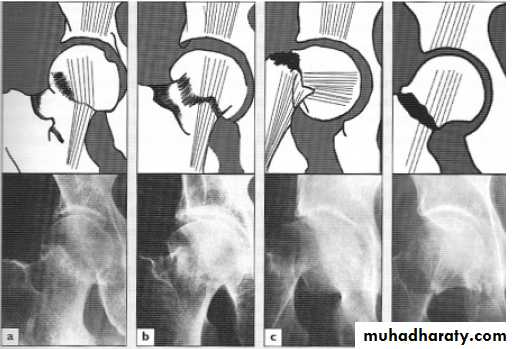
Garden’s Classification:
Based on the amount of displacement in the Pre-reduction X-ray (Radiological)
Stage І : Incomplete undisplaced Fracture (impacted or abducted)
Stage II : Complete undisplaced FractureStage ІІІ : Complete with moderate displacement
Stage IV : Complete with severe Displacement
Any downstage may progress to upstage if left untreated
Two problems affect the healing process :
1-Bone ischemia2-Tardy union
1-Bone ischemia:
Femoral head blood supply come from 3 sources
Vessles through Ligamentum teres (very scanty).
Medullary vessles (will be damaged by the fracture).
Capsular vessles (liable for comprssion by the displaced fracture).
So the blood supply of femoral head will be decreased (ischemia)
Stage І & II better prognosis (Union and viability of femoral head)
2- Tardy union:
A-Bone ischemia
B-Flimsy periosteum with no contact with soft tissue
C-Synovial fluid prevents clotting of hematoma
-Clinical Features:
classically old femaleHistory of minimal trauma
Deformity (short and externally rotated limb)
Inability to walk ( may be able to walk if impacted fracture)
May not be so obvious:
X-ray:
Is there a fracture, and is it displaced?Usually Break is obvious but impacted one can be missed
Displacement (abnormal shape of bone outline, mismatch of the trabecular lines)
Diagnosis:
fracture neck femur may be missed in:
• Stress fracture : no history of trauma.
• Impacted fracture: the patient may be able to walk.
• Painless fracture: elderly with minimal trauma usually feel minimal pain.
• Pathological fracture: patient with metastasis may be fractured during nursing.
Treatment:
In the emergency unit do skin traction + admitting the patient.No role for conservative treatment aiming for early mobilization.
Treatment depend on the age and fracture type
Type 1 & 2 : they are already reduced just do closed internal fixation.
Type 3 & 4: closed reduction + internal fixation if faileda- age <60 years ORIF
b- age >60 years partial hip replacement (Austin moore)


3-Early activity: (
-From the first day, the pt should sit up in bed or in a chair and encouraged to start walking using crutches or walker.Complications:
early general complications like:1-DVT 2- pulmonary emobolism 3- pneumonia 4- bed sore
Late:
• avascular necrosis treated by partial or total hip replacement.
• Non union treated either by (ORIF + bone graft ) or hip replacement.
• Osteoarthritis if severe symptoms treated by hip replacement.
Intertrochantric fractures
ExtracapsularSame risk factors of the femoral neck fracture
This fracture unites quite easily and seldom cause avascular necrosis
Fracture line pass between the greater and lesser trochanter . the stability (classification)of the fracture will depend on the degree of comminution.
Mechanism of injury:
Fall directly into the greater trochanter or by indirect twistingThe proximal segment tends to displace in varus (coxa vara)
Clinical features:
Pain follow a fall, the pt. is unable to stand
The leg is shorter and more externally rotated than femoral neck #
X-ray:
The fracture usually runs diagonally from the greater to the lesser trochanter
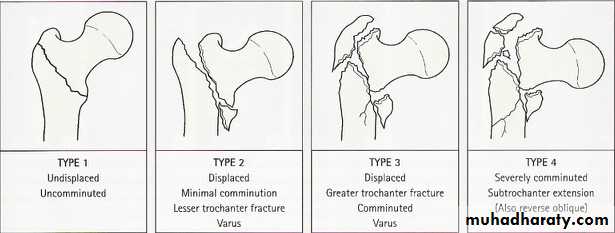
Kyle classification
Treatment:These fractures almost always treated by early internal fixation although they unite quiet easily by conservative treatment.

Complications:
Early: same of femoral neck fractureLate:
• Malunion: coxa vara (neck shaft angle <135o)
• Delayed union
• Nonunion: this is rare because it is extra capsular fracture.

Proximal Femoral Fractures In Children
Hip fractures rarely occur in childrenDue to high velocity trauma (falling, RTA)
Pathological fractures sometimes occur through a bone cyst or benign tumor
Under 2 years, the probability of child abuse should be considered
Between 4 &8 years the ligamentum teres contribute very little to the blood supply
Delbet Classifications:
Type І: is a fracture-separation of the epiphysis; sometimes the epiphyseal fragment is dislocated from the acetabulum
Type II: a transcervical fracture of the femoral neck, the commonest (50%)
Type III : is a basal (cervical-trochantric) #, the second most common injury
Type IV: Intertrochantric fracture.
Treatment:
These # should be treated as a matter of urgency, and certainly within 24 hrs of injuryUndisplaced fractures immobilization in a plaster spica
Displaced type IV closed reduction, traction and spica immobilization.
Type I,II and III fractures treated by closed reduction and then internal fixation with smooth pins or cannulated screws

• Complications: 1- AVN.2- Malunion . (coxa vara)3- Shortening .

Subtrochanteric Fractures
Occurs mostly with relatively trivial injury In an elderly pt. with osteoporosis, osteomalacia or paget’s disease.Blood loss is greater than with femoral neck or trochanteric # making healing slower
Fracture healing is slowClinical Features:
Leg lies externally rotated & shortthigh is markedly swollen.
movement is painful
X-ray:
The # is through or below the lesser trochanter & frequently comminuted.
Treatment:
Open reduction & internal fixation is treatment of choiceComplications:
Early• Shock
• vascular injury
Late
• Malunion.
• Delayed union
• Non union