
Hearing impairment,
deafness
, or
hearing loss
refers
to
the
inability to hear things, either totally or partially. Symptoms may be
mild, moderate
,
severe or profound
. A patient with mild hearing
impairment may have problems understanding speech, especially if there is a
lot of noise around, while those with moderate deafness may need a hearing
aid. Some people are severely deaf and depend on lip-reading when
communicating with others.
People who are profoundly deaf can hear nothing at all
. In
order to communicate spontaneously and rapidly with people, they are
totally
reliant on lip-reading and/or sign language
.

What is the difference between hearing loss and deafness
?
Hearing loss
refers to a
diminished ability
to hear sounds like other people
do,
while
Deafness
refers to
the inability
to understand speech through hearing even
when sound is amplified
.
Profound deafness =totally deaf
means the person cannot hear
anything at all; they are unable to detect sound, even at the highest volume
possible
.

A few facts and figures about deafness in UK
•10 million people (approx.) in the UK are affected by
hearing loss (1 in 6).
•6.5 million of these are aged
60
and over.
•3.7 million are of
working age
.
•Around 2 million people
use hearing aids.
•About 800,000 are
severely or profoundly deaf
.
•Many people with hearing loss also
have tinnitus
. They
may also have
balance difficulties
.
•Hearing loss increases sharply with age - about a third of
people aged 70+ have a hearing loss
.
But 10 million people
make deafness the second largest disability in the UK.
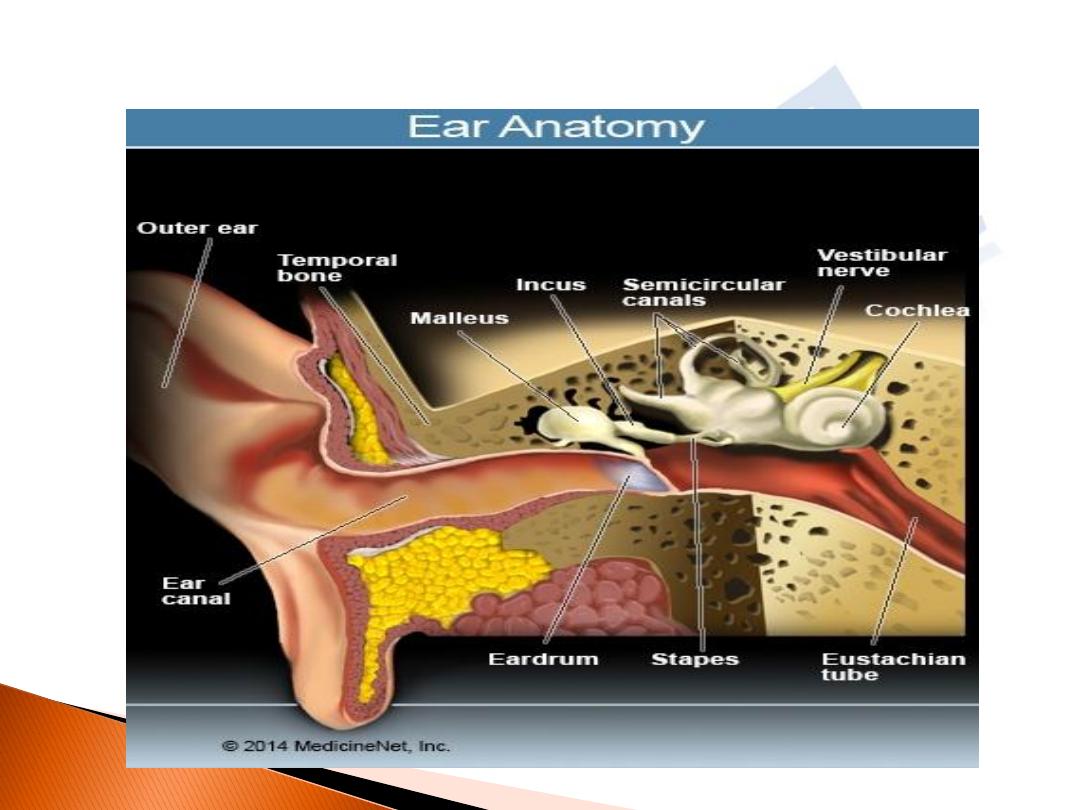
How do we hear things
?

Three Types of Hearing Loss
•Conductive hearing loss
-
when hearing loss is due to
problems with the ear canal, ear drum, or middle ear and its little
bones (the malleus, incus, and stapes).
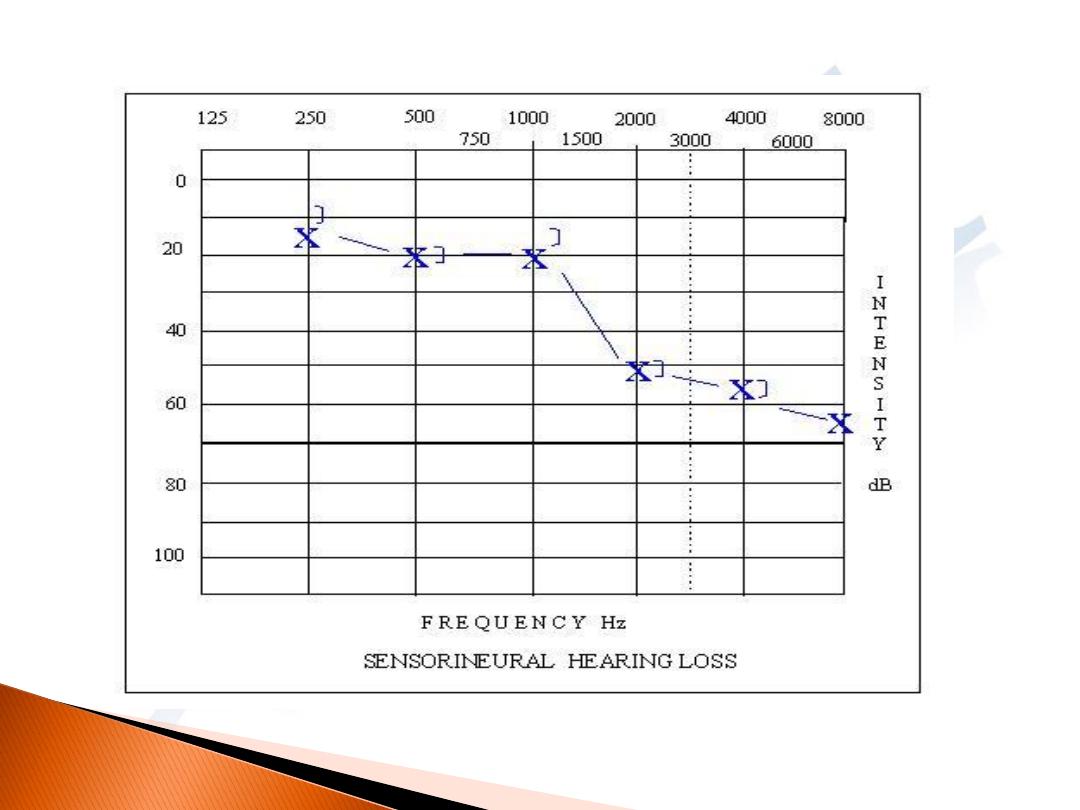
•Sensorineural hearing loss (SNHL
)
- when hearing loss
is due to problems of the inner ear, also known as nerve-related
hearing loss.
•Mixed hearing loss
- refers to a combination of conductive
and sensorineural hearing loss. This means that there may be
damage in the outer or middle ear and in the inner ear (cochlea)
or auditory nerve.

Conductive Hearing Loss
Causes
:
•Malformation
of outer ear, ear canal, or middle ear structures
•Fluid in the middle ear
from colds (OME).
•Ear infection
( Acute & Chronic suppurative otitis media -
•Allergies
•Poor Eustachian
tube function.
•Perforated
eardrum.
•Benign or malignant tumors in external canal and middle ear.
•Impacted earwax.
•Infection in the ear canal (Otitis externa).
•Foreign body in the ear.
•Otosclerosis.
•Tympanosclerosis,,adhesive otitis media.

Treatments of Conductive Hearing Loss
According to underlying cause:
-
congenital cause
by surgery or hearing may be improved
with amplification with a bone conduction hearing aid, or a
surgically implanted, osseointegrated device (for example, the
Baha or sound bridge), or a conventional hearing aid, depending
on the status of the hearing nerve.
Infection
treated medically or surgery
Tumor
by surgery ,radiotherapy
Genetic like otosclerosis
by drug flouride ,surgery
,or hearing aids

Sensorineural Hearing Loss
Causes
:
Head trauma.
Exposure to loud noise (noise induced hearing loss, Acaustic trauma).
INFECTION
S:-
.
Viral causes
: such
as
Chicken pox ,Cytomegalovirus ,Mumps, Meningitis,
AIDS - offspring of mothers who had AIDS during pregnancy have a much
higher risk of being deaf by the age of 16 years
*
Syphilis *Lyme disease *Tuberculosis (TB
),
experts believe that the
medication, streptomycin, used to treat TB may be the key risk factor
Sickle cell disease .
Diabetes
- studies have shown that up to 40% of diabetic patients suffer
from some kind of hearing loss **
Hypothyroidism , Arthritis
Ototoxic drugs
Autoimmune disease
.
Hearing loss that runs in the family (hereditory).
.
Aging (presbycusis
(
.
Malformation of the inner ear.
Meniere
’s Diseae.
Otosclerosis - a hereditary disorder in which a bony growth invade the
cochlea damage the hair cell.
Tumors

Treatment of Sensorineural Hearing Loss
:
•SND from acoustic trauma
(or exposure to excessively loud noise
)
, by
corticosteroids
ot noitammalfni dna gnillews llec riah aelhcoc ecuder ot
serutcurts rae renni derujni eseht fo gnilaeh evorpmi
.
•SND from head trauma or abrupt changes in air pressure such as in airplane
descent, which can cause inner ear fluid compartment rupture or leakage,
which can be toxic to the inner ear. There has been variable success with
emergency surgery
when this happens
.
•SND be of viral origin
, is an otologic emergency that is medically treated with
corticosteroids
.
•Bilateral progressive hearing loss
sa desongaid osla ,shtnom lareves revo
autoimmune inner ear disease,
is managed medically
with long-term
corticosteroids
ypareht gurd htiw semitemos dna
..
•Fluctuating sensorineural hearing loss
ro esuac nwonknu morf eb yam
htiw detaicossa
Meniere
’s
Disease may be treated medically with a low-
sodium diet, diuretics, and corticosteroids. If the vertigo is not medically
controlled, then various surgical procedures are used to eliminate the vertigo
.
Treatment of SND
•Sensorineural hearing loss from disease
lartnec eht ni
eht rof tnemeganam lacidem ot dnopser yam metsys suovren
,elpmaxe roF .metsys suovren eht gnitceffa esaesid cificeps
desrever eb yam sisorelcs elpitlum ot yradnoces ssol gniraeh
sisorelcs elpitlum rof tnemtaert htiw
.
•Sensorineural hearing loss from tumors
of vestibular nerve
(Acaustic neuroma)
, by surgery.
Irreversible sensorineural hearing loss
,
nommoc tsom eht
deganam eb yam ,mrof
with hearing aids
sdia gniraeh nehW .
yllacigrus eb nac ssol gniraeh fo epyt siht ,hguone ton era
htiw detaert
cochlear implants

Mixed Hearing Loss
Treatments for Mixed Hearing Loss
•Recommends taking care of the conductive
component first
.(medically or surgical( .
To make the person a better hearing aid candidate
,
.

Degree of deafnes ,Hearing impairment
There are
four
levels of deafness (possibly 5 in some countries), they
are
:
•
Mild deafness or mild hearing impairment
- the patient can only detect
sounds from between
25 to 39
decibels
.(
•
Moderate deafness or moderate hearing impairment
- the patient can
only detect sounds from between
40dB and 69dB
.
•
Severe deafness
- the person only hears sounds above
70db to
89dB
. .
•
Profound deafness
- anybody who cannot hear a sound below
90dB
is
profoundly deaf
;
•
Obviously, if the hearing impaired or deaf person can read and write,
they may also communicate by reading and writing

Others degree
Mild
:
for adults: between
26 and 40
dB HL
for children: between
20 and 40
dB HL
Moderate: between 41 and 54 dB
HL
Moderately severe: between 55 and 70 dB
Severe: between 71 and 90 dB
Profound: 91 dB HL or greater
Totally deaf: Have no hearing at all. This is called
anacusis

How deafness diagnosed
?
Patients who suspect something is wrong with their hearing will usually
go and see their GP (general practitioner, primary care physician)
initially
.or ENT doctors.
-
Start with history of the symptoms
, when they started, whether or not
they have gotten worse, whether there is any pain, etc
.
A physical examination
- the doctor will look into the patient's ear using
an otoscope (auroscope). The finding should be recorded
Doctors may ask questions regarding the patients hearing
,
which will probably be similar to the ones below
:
•Do you often find yourself asking people to repeat what they said?
•Do you find it hard to understand people on the telephone?
Does the doorbell ring and you did not hear it? If so, does this happen
frequently

•When you chat to people face-to-face, do you have to focus
carefully
?
•Has anybody ever mentioned to you that you might have a
problem with your hearing
?
•When you hear a sound, do you often find it hard to determine
where it is coming from
•When several people are talking, do you find it hard to
understand what one of them is telling you
?
•Are you often told that the TV, radio or any sound-producing
device is too loud
?
•Do you find the speech of men easier to understand than
women's or children's
?
•Have you often found yourself misunderstanding what other
people say to you
• Have you hear ringigng,rushing ,hissing sounds in ears(Tinitus).
•?
Anybody who answers "yes" to most of the above
questions should see their doctor and have their hearing
checked
.

The diagnosis of deafnes depend on folowing tests:
.
Whispered speech test
.
The doctor will whisper a combination
of numbers and letters from behind the patient and ask him to
repeat the combination to check if he can hear anything .Each ear
should be tested separately.
Tuning fork test
.
Pure tone audiometry
.
.
Otoacoustic emissions
.
This test is used to measure your
cochlear function
by recording signals produced by the hair cells.
Auditory brainstem response
.
This test measures the
activity of cochlea, auditory nerve and brain when a sound is
heard

If your hearing loss has a sensorineural cause, a
number of other tests can be done to pinpoint
where the problem lies
.
**
In cases of unilateral sudden sensorineural
deafness
need to do CT
scan and MRI scan
. This is to
rule out rare causes of hearing loss such as an
acoustic
neuroma or cholesteatoma
or other intracranial (cerebellopontine
angle) tumour

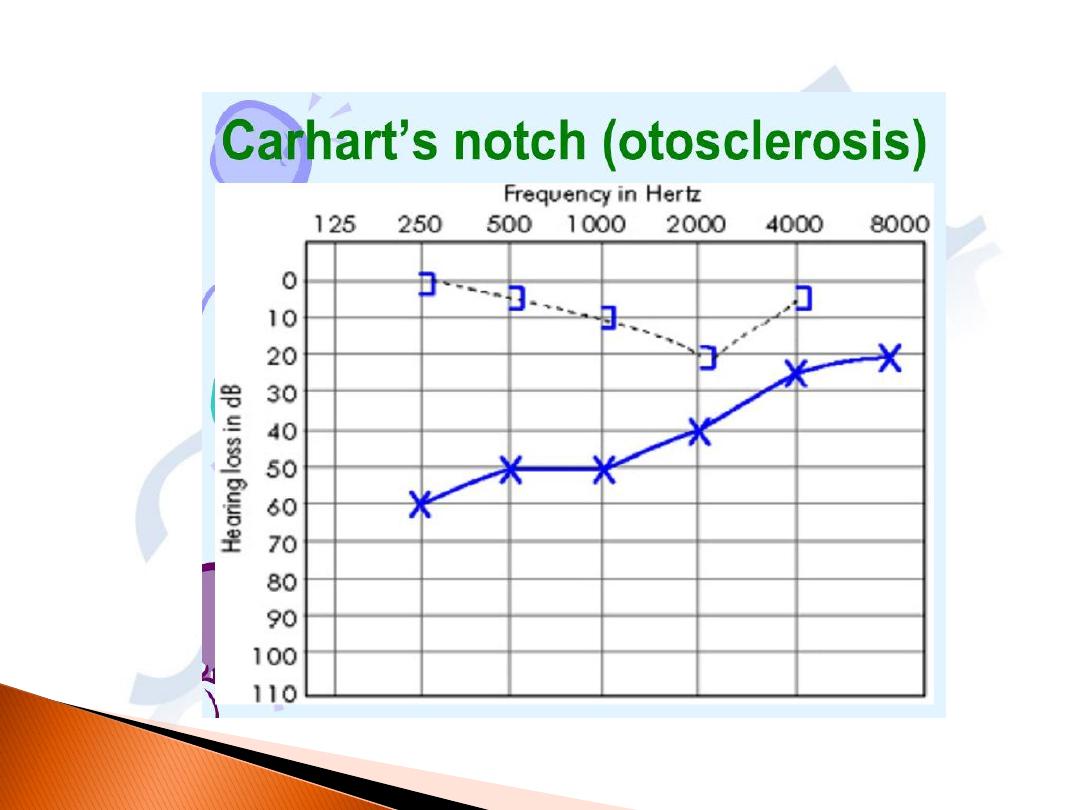
Otosclerosis
Definition:
a localized disease of the
otic capsule in which new spongy
bone causes ankylosis of the
footplate of stapes or invades the
cochlea.
.

Aetiology
:
exact causes unknown, many theories
.
-
Measles virus RNA
is found in otosclerotic foci in
footplates removed during surgery. Measles
virus infection may activate the gene responsible
for otosclerosis. -
-
Hereditary
(50%
+ve family history) inhereted as autosomal
dominant pattern with incomplete penetrance
-
Incidence
: more in white races, female two time
more male
- Age of onset
20-30 years of age.
-
Effect of pregnancy
accelerate the condition but
never cause it (pill have the same effects)

Pathology
:
normal bone absorbed and
replaced by new spongy osteoid bone. The
commonest site 80-90% is on the anterior
margin of the footplate of the stapes at its
attachment to the oval window called
(fissula ante fenestram) and spread via
vascular channels leads to ankylosis
(fixation) of the stapes footplate. It may
involve the cochlea and labyrinth in8% so
called labyrinthine otosclerosis, 2% both
stapes and cochlea
.

Clinical features:
-
Deafness
is the predominant symptom, usually gradual
bilateral (80%) and it's conductive in type.
Patients exhibit low volume-speech.(hear their voice
louder).
Usually takes many years to becom obvious .
Sensorineural deafness if the cochlea involved
.
*
Paracusis welleci
(the patient hears better in
a background noise).
-
Tinnitus
--Vertigo
symptom appear at any age from 15-45yrs mostly at
twenties.
On Examination:
-
Normal tympanic membrane. Flamingo-
pink tinge (reddish –blue hue)
(
Schwartze's sign)
may be seen through the
TM due to hyperemia of the promontory
due to hyper vascular immature bone.
-
Conductive deafness by tuning fork
tests

I
nvestigation
:
-
PTA
show low frequency conductive loss. Then involve high
frequency with widening of airbone gap
Carhart's notch = dip at 2 KHz
which is characterized by elevation of bone
conduction thresholds of 5 dB at 500 Hz, 10 dB at
1000 Hz, 15 dB at 2000 Hz, and 5 dB at 4000 Hz. A
Carhart notch may also be seen in cases of
incudostapedial joint detachment and incus or
malleus fixation.
-
Tympanometry
=(type A)
normal middle ear pressure with
reduced compliance and absent stapedial reflex
-
Tomography
may show thickening of the footplate
of the
stapes.
D.Dx
1-Chronic non- suppurative OM
2- Ossicular disconnection or fixation
How is Otosclerosis Treated
1
-Do nothing (conservative approach
2--
Amplification Hearing aids
are
usually effective for conductive hearing
loss
3--
Medical treatment
To date, the only proposed medical treatment has been
sodium fluoride,
which is a
dietary supplement (not a drug). This treatment is not widely accepted, and has not
been proven to be effective
4-surgical treatment
:
***
The stapedotomy operation..
Do opening (fenestra) in footplate of stapes.
***
The stapedectomy operation .
when thick sclerosed footplate.
Complication
1-Loss of hearing due to sensory hair cell damage.
2-Dizzenes loss of balance
3-Taste disturbance chorda tympani damage
4-Tinitus
5-**Cohlear implant

Meniere's Disease
WHAT IS MÉNIÈRE`’S DISEASE
?
M
énière`’s disease describes a set of episodic symptoms including
vertigo ,intermittent hearing loss, tinnitus
.
Episodes of
vertigo (spinning sensation)
typically
last
from 20 minutes up to 4 hours
.
Hearing loss
is
often intermittent
, ,lattr on
becomes
permanent
.
Tinnitus:-
A roaring,
buzzing, or ringing sound in the ear
)
,
.rae detceffa eht ni ssenlluf fo noitasnes a dna
emoc yam
tsuj ro gnirud rucco ,gniraeh ni segnahc htiw og dna
tnatsnoc eb ro ,skcatta erofeb
.
M
énières disease
is also called idiopathic endolymphatic
hydrops and is one of the most common causes of dizziness .The
disease mostly unilateral ,only 15% both ears
.

Cause of Meniere's
disease
isn't well understood
Due to
abnormal volume
or
composition of fluid in
the inner ear
.
Inner ear consist of bony labyrinth and inside it
membranous labyrinth contain endolymph, there is
sensory cell response for fluid movement ,pressure
,composition.
In order to function properly, the fluid needs to retain a
certain volume, pressure and chemical composition
.
Too
much fluid may accumulate either due to excess
production or inadequate absorption
.
.Alteration of the
properties of inner ear fluid may help cause Meniere's
disease
.

Anumbers of potential causes or triggers,
gnidulcni
:
•
Faulty water metabolism
or Improper fluid drainage, perhaps
because of a blockage or anatomic abnormality
•
Sodium retention
•Disturbance of hormonal control of water and electrolyte
transport
•
Abnormal immune response.
•
Allergies (Histamine sensitivity).
•Sympathetic over activity
•
Viral infection
•
Genetic predisposition
•
Head trauma
•
Migraines
Because no single cause has been identified, it's likely
that Meniere's disease is caused by a combination of
factors

Pathology:
-Distension of membranous
labyrinth (especially in scala media
of the cochlea and saccule).
Distension of the scala media
causes bulging of reissner's
membrane into scala vestibule. The
distended saccule may spread over
the stapedial footplate. Rupture of
distended parts.
-Degeneration of sensory elements.

Clinical features
:
Usually unilateral at first. Slightly more common in
males. Onset usually between 35-55 years.
-
Vertigo in attacks
, the duration varies from few
minutes to two hours. Horizontal nystagmus
usually to opposite side may be seen.
-Sensorineural
deafness at first affects the lower
frequencies early reversible but progress with
each attack and the higher frequencies are
increasingly involved and become permanent at
the end. Recruitment (abnormal rapid growth of
loudness, due to cochlear damage) also may be
found.
-

--
Tinnitus
.
-
Vagal disturbances
: nausea, vomiting
even diarrhea, pallor, cold sweat and
lowered blood pressure.
-
Headache
(Associated migraine in 7-
20%)
-
Anxiety.
Diagnosis:
-PTA: SND
-Caloric test: between the attacks shows
canal paresis. (What is caloric test?)

DIAGNOSIS
1-HISTORY
2-•
An audiometric examination
(hearing test PTA) indicates a sensory
type of hearing loss in the affected ear. Speech discrimination is often
diminished in the affected ear.
3-For balance
•An ENG (electronystagmogram
) with caloric test. In about 50 percent
of patients, the balance function is reduced in the affected ear.
4-Other tests
•
Electrocochleography (ECoG
) may indicate increased inner ear fluid
pressure in some cases of Ménière’s disease.
The auditory brain stem response
(ABR),
, computed tomography
(CT),
or magnetic resonance imaging
(MRI)
may be needed to rule out a tumor
occurring on the hearing and balance nerve. Such tumors are rare, but they
can cause symptoms similar to Ménière’s disease.

Differential diagnosis
:
1-Labyrinthitis
2-Cogan's disease
3-Vestibular neuronitis
4-BPPV
5-Acoustic neuroma
6-Disseminated sclerosis
7-Epilepsy

T
reatment
:
Conservative
: -
Reassurance
TO REDUCE THE FREQUENCY OF EPISODES BY
Avoid stress and excess salt ingestion, caffeine, smoking,
and alcohol. Get regular sleep and eat properly. Remain
physically active, but avoid excessive fatigue.
Attacks of vertigo can controlled by
-
Sedation (diazepam)
- Labyrinthine sedatives (Cinnarizine, promethazine)
- Vasodilators (Betahistine hydrochloride)
- Removal of toxic foci
- Diuretics (if the attacks are related to menstrual cycle)
- Restriction of salts and fluid intake
-
Intratympanic injection with either
gentamicin or dexamethasone through
temporary opening or placing a tube in the eardrum. But
gentamycin cause SND
-An air pressure pulse generator
a
mechanical pump that is
applied to ear
canal for 5 minutes 3 times a day
-

WHEN IS SURGERY RECOMMENDED
?
Surgery is needed in only a small minority of patients with
Meniere’s disease
.
If vertigo attacks are not controlled by
conservative measures and are disabling, one of the following
surgical procedures might be recommended:
••
Endolymphatic sac shunt or decompression
relieves attacks of
vertigo in one-half to two-thirds of cases
••
Selective vestibular neurectomy
:- .
While vertigo attacks are
permanently cured in a high percentage of cases, patients may continue to
experience imbalance, hearing function is usually preserved
.
••
Labryrinthectomy and eighth nerve section
:
.
snoc si sihT
idered
when the patient with M
énière’-s disease has poor hearing in the affected
ear .This procedure will result in the highest rates for control of vertigo attacks
.

Presbycusis
Presbycusis (also spelled presbyacusis
,
from Greek presbys ”redle“
+akousis
”gniraeh“
ega ro ,)
-
detaler
hearing loss
,
evitalumuc eht si
no gniga fo tceffehearing lacirtemmys laretalib evissergorp a si tI .
ega
-
detaler
sensorineural hearing loss
tsom si ssol gniraeh ehT .
ta dekram
seicneuqerf rehgih
.
There are four pathological types of presbycusis
:
•Sensory
:
characterised by degeneration of organ of corti
.
•Neural
:
characterised by degeneration of cells of spiral ganglion
.
•Strial/metabolic:
characterised by atrophy of stria vascularis in all
turns of cochlea
.
•Cochlear conductive
:
due to stiffening of basilar membrane thus
affecting its movement

Presentation
Bilateral high frequency sensorineural deafness,
poor discrimination.
Deterioration in hearing has been found to
start very early
morf ,
fo ega eht tuoba18 years.
egA
seicneuqerf hgih stceffa
naht erom
dna ,wol
nemow naht yltneuqerf erom nem
.
ga fo stceffe ehT
ing can
be exacerbated by
exposure to environmental noise
si sihT ,
noise-
induced hearing loss
sisucybserp morf tcnitsid si dna )LHIN(
.
Over time, the detection of high-pitched sounds becomes more
difficult, and speech perception is affected, particularly of
sibilants
dna
fricatives
detceffa eb ot dnet srae htoB ..

Pathophysiology
Degeneration due to vascular insufficiency: Atrophy
of epithelial, neural tissues and stria vascularis in
the cochlea.

CAUSES
Factors that can cause hearing loss
•
Heredity
eht fo ytilibitpecsus dna aelhcoc eht fo gniga ylrae ekil srotcaF :
denimreted yllaciteneg era stlusni gurd rof aelhcoc
.
•
Atherosclerosis
ybereht ,aelhcoc eht fo ytiralucsav hsinimid yaM :
ylppus negyxo sti gnicuder
.
•
Dietary habits
fo ekatni desaercnI :
saturated fat
etarelecca yam
ega dlo ni segnahc citorelcsorehta
.
•
Diabetes
doolb eht ni noitarefilorp lailehtodne dna sitilucsav esuac yaM :
ylppus doolb sti gnicuder ybereht ,aelhcoc eht fo slessev
.
•
Noise trauma
ot erusopxE :
loud noise
/
music
sesserts sisab gniunitnoc a no
sisucybserp eht gninetsah ,aelhcoc cixopyh ydaerla eht
.
•
Smoking
:
doolb ni segnahc citorelcsorehta etautnecca ot detalutsop sI
sisucybserp gnitavargga slessev
.
•
Hypertension
doolb ni noitcuder ekil ,segnahc ralucsav tnetop sesuaC :
sisucybserp gnitavargga ybereht ,aelhcoc eht ot ylppus
.
Ototoxic drugs
ekil sgurd cixototo fo noitsegnI :
aspirin
eht netsah yam
sisucybserp fo ssecorp

Treatments
]
Devices like
hearing aids
and
cochlear
implants
fo gniraeh evorpmi pleh ydaerla
ylredle ynam
.
Though still in their early stages,
several treatments for presbycusis are in development.
Included in these are the water-soluble coenzyme Q10
formulation, fetal thymus grafting, and the
prescription drug Tanakan ni demrofrep yduts a nI .
2010 ,it was found that the water-soluble formulation
of coenzyme Q10( CoQ10 )caused a significant
improvement in liminar tonal audiometry of the air
and bone thresholds at 1000 Hz ,2000 Hz ,4000 Hz,
and 8000 Hz.
lairt lacinilc regral a taht ylekil si tI
demrofrep eb lliw

Ototoxicity
..
The extent of ototoxicity varies with the drug, the dose, and other
conditions. In some cases, there is full recovery after the drug has been
discontinued. In other cases, the extent of damage is limited, and may
even be too small to be noticed. This may occur in highfrequency hearing
loss,, there may be permanent and complete deafness
.
.
Symptoms of ototoxicity include
partial or profound hearing loss
,
vertigo
,
and tinnitus.
Definition
:
damage of the cochlear and or the vestibular part of the
inner ear and or the vestibulocochlear nerve by drugs and
chemical agent

Causes and symptoms
Many drugs can cause ototoxicity
.
Antibiotics
•amikacin (Amikin)
•streptomycin
•neomycin
•gentamicin (Garamycin(
•erythromycin .
•kanamycin(
•tobramycin(
•netilmycin (Netromycin)
•vancomycin (Vancocin
)
Anti-cancer drugs
•cisplatin (Platinol AQ)
•bleomycin (Blenoxane)
•vincristine (Oncovin
)
Diuretics
•acetazolamide (Diamox)
•furosemide (Lasix)
•bumetanide (Bumex)
•ethacrynic acid (Edecrine
)
.
Aspirin
overdose causes ringing in the ears. The
antimalarial drugs
quinine and
chloroquine may also cause ear damage. environmental chemicals that can cause ear
damage
are tin, lead, mercury, carbon monoxide, and carbon disulfide
.

Treatment
There are no current treatments to reverse the effects of
ototoxicity
.
Preventive: Avoid or discontinue ototoxic drugs
Monitor treatment.
Monitor hearing (How?)
Therapeutic: no medical or surgical treatment is effective
.
People who suffer permanent hearing loss may elect to use
hearing aids
,etairporppa nehw ,ro ,
receive a cochlear
implant.
For
those who
have balance problems
,
physical therapy
may often be helpful.
htiw elpoep pleh nac stsipareht lacisyhP
snoitasnes eht dna noisiv no erom yler ot nrael smelborp ecnalab
ecnalab eveihca ot selcsum morf
.