Stomach and duodenum
Blood supply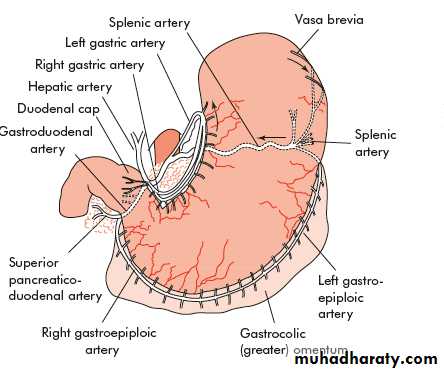
The stomach and duodenum possess both intrinsic and extrinsic nerve supplies
The intrinsic nerves exist principally in two plexuses, the myenteric plexus of Auerbach and the submucosal plexus ofMeissner.The extrinsic supply is derived mainly from the vagus nerves(CN XI
The sympathetic supply is derived mainly from the coeliac ganglia.
Parietal cells
These are in the body (acid-secreting portion) of the stomach and line the gastric crypts, being more abundant distally. They are responsible for the production of hydrogen ions to form hydrochloric acid.Chief cells
These lie principally proximally in the gastric crypts and produce pepsinogen. Two forms of pepsinogen are described: pepsinogen I and pepsinogen II.
Endocrine cells
In the gastric antrum, the mucosa contains G cells, which produce gastrin. Throughout the body of the stomach, enterochromaffin-like (ECL) cells are abundant and produce histamine, a key factor in driving gastric acid secretion.In addition, there are large numbers of somatostatin-producing D cells throughout the stomach, and somatostatin has a negative regulatory role.
Duodenum
The duodenum is lined by a mucus-secreting columnar epithelium. In addition, Brunner’s glands lie beneath the mucosa and are similar to the pyloric glands in the pyloric part of the stomach. Endocrine cells in the duodenum produce cholecystokinin and secretin.
Gastritis
Type A gastritisThis is an autoimmune condition in which there are circulating antibodies to the parietal cell. This results in the atrophy of the parietal cell mass, hence hypochlorhydria and ultimately achlorhydria. As intrinsic factor is also produced by the parietal cell there is malabsorption of vitamin B12, which, if untreated, may result in pernicious anaemia. In type A gastritis, the antrum is not affected and the hypochlorhydria leads to the production of high levels of gastrin from the antral G cells. This results in chronic hypergastrinaemia. Patients with type A gastritis are predisposed to the development of gastric cancer.
Type B gastritis
There are abundant epidemiological data to support the association of this type of gastritis with H. pylori. Most commonly, type B gastritis affects the antrum, and it is these patients who are prone to peptic ulcer disease. Helicobacter-associated pangastritis is also a very common manifestation of infection. Patients with pangastritis seem to be most prone to the development of gastric cancer.Reflux gastritis
This is caused by enterogastric reflux and is particularly common after gastric surgery.it is occasionally found in patients with no previous surgical intervention or who have had a cholecystectomy.
Erosive gastritis
This is caused by agents that disturb the gastric mucosal barrier; NSAIDs and alcohol are common causes. The NSAID-induced gastric lesion is associated with inhibition of the cyclo-oxygenase type 1 (COX-1) receptor enzyme, hence reducing the production of cytoprotective prostaglandins in the stomach.Stress gastritis
This is a common sequel of serious illness or injury and is characterised by a reduction in the blood supply to superficial mucosa of the stomach. Although common, this is not usually recognised unless stress ulceration and bleeding supervene, in which case treatment can be extremely difficult.Ménétrier’s disease
This is an unusual condition characterised by gross hypertrophy of the gastric mucosal folds, mucus production and hypochlorhydria. The condition is premalignant and may present with hypoproteinaemia and anaemia. There is no treatment other than a gastrectomy.Lymphocytic gastritis
This type of gastritis is seen rarely. It is characterised by the infiltration of the gastric mucosa by T cells and is probably associated with H. pylori infection. The pattern of inflammation resembles that seen in coeliac disease or lymphocytic colitis.
Other forms of gastritis
Eosinophilic gastritis appears to have an allergic basis, and is treated with steroids and cromoglycate.
Granulomatous gastritisis seen rarely in Crohn’s disease and also may be associated with tuberculosis.
Acquired immunodeficiency syndrome (AIDS) gastritis is secondary to infection with cryptospiridiosis.
Phlegmonous gastritis is a rare bacterial infection of the stomach found in patients with severe intercurrent illness. It is usually an agonal event
Peptic ulcer
Common sites for peptic ulcers are the first part of the duodenum and the lesser curve of the stomach, but they also occur on the stoma following gastric surgery, the oesophagus and even in a Meckel’s diverticulum, which contains ectopic gastric epithelium.In general, the ulcer occurs at a junction between different types of epithelia, the ulcer occurring in the epithelium least resistant to acid damage.
Aetiology
It is now widely accepted that infection with H. pylori and the consumption of NSAIDs are the most important factors in the development of peptic ulceration. In combination, H. pylori and NSAIDs act synergistically to promote ulcer development and ulcer bleeding. Cigarette smoking predisposes to peptic ulceration and increases the relapse rate after treatment, with either gastric antisecretory agents or, in the past, elective surgery.Pathology
Most occur in the first part of the duodenum. A chronic ulcer penetrates the mucosa and into the muscle coat, leading to fibrosis and pyloric stenosis. Sometimes there may be more than one duodenal ulcer. The situation in which there is both a posterior and an anterior duodenal ulcer is referred to as ‘kissing ulcers’. Occasionally, the ulceration may be so extensive that the entire duodenal cap is ulcerated and devoid of mucosa.Histopathology
Microscopically, destruction of the muscular coat is observed and the base of the ulcer is covered with granulation tissue, the arteries in this region showing the typical changes of endarteritis obliterans. Sometimes the terminations of nerves can be seen among the fibrosis.Gastric ulcers
IncidenceAs with duodenal ulceration, H. pylori and NSAIDs are the important aetiological factors. Gastric ulceration is also associated with smoking. Gastric ulceration is substantially less common than duodenal ulceration. The sex incidence is equal and the population with gastric ulcers tends to be older. It is more prevalent in low socioeconomic groups and is considerably more common in the developing world than in the West.
Pathology
This is essentially similar to that of a duodenal ulcer, except that gastric ulcers tend to be larger. Fibrosis, when it occurs, may result in the now rarely seen hourglass contraction of the stomach. Large chronic ulcers may erode posteriorly into the pancreas and, on other occasions, into major vessels such as the splenic artery.
Malignancy in gastric ulcers
Chronic duodenal ulcers are not associated with malignancy and, in contrast, gastric ulcers are. Widely varying estimates are made of the incidence of gastric malignancy in gastric ulcers.It is fundamental that any gastric ulcer should be regarded as being malignant, no matter how classic the features of a benign gastric ulcer. Multiple biopsies should always be taken, perhaps as many as ten well-targeted biopsies.
Further biopsies are taken while the ulcer is healing and when healed. Modern antisecretory agents can frequently heal the ulceration associated with gastric cancer but, clearly, are ineffective in treating the malignancy itself.
Clinical features of peptic ulcers
PainThe pain is epigastric, often described as gnawing and may radiate to the back. Eating may sometimes relieve the discomfort. The pain is normally intermittent rather than intractable.
Periodicity
Symptoms may disappear for weeks or months to return again. This periodicity may be related to the spontaneous healing of the ulcer.
Vomiting
While this occurs, it is not a notable feature unless stenosis has occurred.
Alteration in weight
Weight loss or, sometimes, weight gain may occur. Patients with gastric ulceration are often underweight but this may precede the occurrence of the ulcer.Bleeding
All peptic ulcers may bleed. The bleeding may be chronic and presentation with microcytic anaemia is not uncommon. All such patients should be investigated with endoscopy. Acute presentation with haematemesis and melaena
Clinical examination
Examination of the patient may reveal epigastric tenderness.
Investigation of the patient with suspected peptic ulcer
Gastroduodenoscopy
This is the investigation of choice in the management of suspected peptic ulceration and in the hands of a well-trained operator is highly sensitive and specific.
Treatment
H2-receptor antagonists and proton pump inhibitorsEradication therapy: is therefore the mainstay of treatment for peptic ulceration. It is extremely economical by comparison with prolonged courses of antisecretory agents or surgery. It is also considerably safer than surgical treatment.
Endoscopic re-evaluation should be regarded as mandatory to confirm healing of gastric ulcers. Furthermore, endoscopy permits the differentiation between a refractory ulcer and persistent symptoms despite ulcer healing.
Operations for duodenal ulceration
Procedures devised for the treatment of duodenal ulcers have the common aim of excluding the damaging effects of acid from the duodenum.Billroth II gastrectomy
Billroth I gastrectomy
Gastrojejunostomy
Truncal vagotomy and drainage
Highly selective vagotomy
Sequelae of peptic ulcer surgery
Recurrent ulcerationRecurrent ulcers may present with bleeding and perforation. In this respect, the complication of gastrojejuno-colic fistula requires a particular mention. In this rare condition, the anastomotic ulcer penetrates into the transverse colon. Patients suffer from diarrhoea that is severe and follows every meal. They have foul breath and may vomit formed faeces. Severe weight loss and dehydration are rapid in onset, and for this reason the condition may be mistaken for malignancy.
Small stomach syndrome
Early satiety follows most ulcer operations to some degree, including highly selective vagotomy. In this latter circumstance, although there is no anatomical disturbance of the stomach there is loss of receptive relaxation. Fortunately, this problem does tend to get better with time.
Bile vomiting
Bile vomiting can occur after any form of vagotomy with drainage or gastrectomy. Commonly, the patient presents with vomiting a mixture of food and bile or sometimes some bile alone after a meal. Often, eating will precipitate abdominal pain and reflux symptoms are common. Bile chelating agents can be tried but are usually ineffective. In intractable cases, revisional surgery may be indicated.Early dumping
Early dumping is found in about 10 per cent of patients following gastrectomy or vagotomy and drainage. The small bowel is filled with foodstuffs from the stomach, which have a high osmotic load, and this leads to the sequestration of fluid from the circulation into the gastrointestinal tract. The principal treatment is dietary manipulation. Small, dry meals are best, and avoiding fluids with a high carbohydrate content also helps. Revisional surgery may occasionally be requiredLate dumping
This is reactive hypoglycaemia. The carbohydrate load in the small bowel causes a rise in the plasma glucose, which, in turn, causes insulin levels to rise, causing a secondary hypoglycaemia. This can be easily demonstrated by serial measurements of blood glucose in a patient following a test meal. The treatment is essentially the same as for early dumping. Octreotide is very effective in dealing with this problem.Postvagotomy diarrhoea
Most patients will suffer some looseness of bowel action to some degree but, in about 5 per cent, it may be intractable. It is related, to some degree, to rapid gastric emptying. It may be severe and explosive, the patient experiencing a considerable degree of urgency.Malignant transformation
Gastrectomy or vagotomy and drainage are independent risk factors for the development of gastric cancer.Nutritional consequences
Nutritional disorders are more common after gastrectomy than after vagotomy and drainage. Weight loss is common after gastrectomy and the patient may, in fact, never return to their original weight. Anaemia may be due to either iron or vitamin B12 deficiency.