Medically compromised patient
HypertensionHypertension
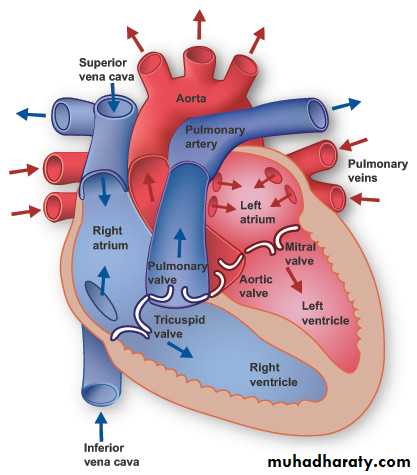
Hypertension is an abnormal elevation in arterial pressure that can be fatal if sustained and untreated.The blood pressure is the product of cardiac output and peripheral resistance and is dependent on the heart and vasculature, autonomic nervous system, endocrine system, and kidneys.

In adults, a sustained systolic blood pressure of 140 mmHg or greater and/or a sustained diastolic blood pressure of 90 mmHg or greater is defined as hypertension.
The systolic pressure is the force that the blood exerts on the artery walls as the heart contracts to pump the blood to the peripheral organs, while the diastolic pressure is residual pressure exerted on the arteries as the heart relaxes.
The difference between diastolic and systolic pressures is called pulse pressure Mean arterial pressure is roughly defined as the sum of the diastolic pressure plus one-third the pulse pressure.
Etiology :
Primary/Essential/Idiopathic HypertensionPrimary/essential hypertension is the most common type of hypertension and accounts for about 95% of all cases presenting with high blood pressure. This type of hypertension has a genetic link and is often associated with cardiovascular risk factors, smoking, obesity, lipid problems, and diabetes.
Secondary Hypertension
Secondary hypertension is always due to an underlying cause such as intrinsic renal diseases, cardiovascular disease, Pheochromocytoma, Cushing's syndrome, thyroid or parathyroid disease, heavy alcohol consumption chronic corticosteroid therapy, chronic NSAIDS therapy or long-term oral contraceptive use can lead to secondary hypertension The secondary hypertension Patient experiences symptoms quite early on compared to The primary/essential hypertension patient and the symptoms are more severe. Many patients with secondary hypertension may be cured after treatment of the underlying cause.Classification of Hypertension :
A recent classification redefines "normal" blood pressure as < 120/80 mmHg and introduces a new category of "prehypertension" (120-139/80-89 mmHg).
Blood pressure classification
Systolic bloodpressure mmHg
Diastolic blood
pressure mmHg
and < 80
<120
Normal
or 80-89
120-139
prehypertension
or 90-99
140-159
Stage 1 hypertension
or ≥100
≥l60
Stage 2 hypertension
Some authors define hypertension as Mild when the systolic blood pressure is 140-159 mmHg and the diastolic is 90-99 mmHg, Moderate -when the systolic is 160-179 mmHg and diastolic is 100-109 mmHg and Severe when the systolic pressure is ≥ 180 mmHg and the diastolic is ≥ 110 mmHg.

Lifestyle risk factors modifying hypertension
Lifestyle can play an important role in the severity and progression of hypertension; obesity, excessive alcohol intake, excessive dietary sodium, and physical inactivity are significant contributing factors.

Clinical features
One third of the hypertensive patients are asymptomatic or only have trivial complications like epistaxis.Symptoms include:
• headaches,
• visual disturbances,
• tinnitus,
• dizziness.


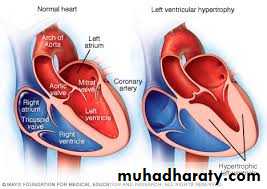
Signs include:
• hypertension on testing,• retinal changes,
• left ventricular hypertrophy,
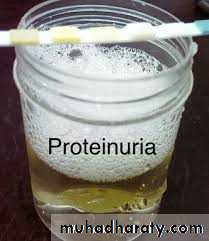
• proteinuria
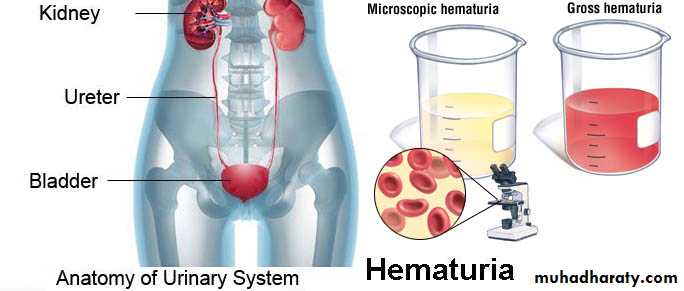
• and hematuria.


Blood pressure is measured with the use of a sphygmomanometer. The diagnosis is based on an average of two or more Properly measured' sealed blood pressure readings on each of two or more office visits. The manual technique for recording blood pressure includes the following steps:
1. Alcohol and smoking should be avoided for 30 min before measurement.
2. Allow the patient to sit at rest for as long as3. Place sphygmomanometer cuff on right upper arm with about 3 cm of skin visible at the antecubital fossa: the bladder should encircle at least two-thirds of the arm.
4. Palpate right brachial pulse..
5. Inflate the cuff slowly to about 200-250 mmHg, or until the pulse is no longer palpable.
6. Deflate cuff slowly while listening with stethoscope over the brachial artery over skin on inside of arm below cuff.
7. Record the systolic pressure as the pressure when the first tapping sounds appear (Korotkoff sounds).
8. Deflate cuff further until the tapping sounds become muffled (diastolic pressure) and then disappear.
9. Record blood pressure as systolic/diastolic pressures.
Management :
Hypertension is diagnosed by standardized serial blood pressure measurements.
Investigations to identify a 'secondary' cause and assess end-organ. damage (also called target organ damage) include:
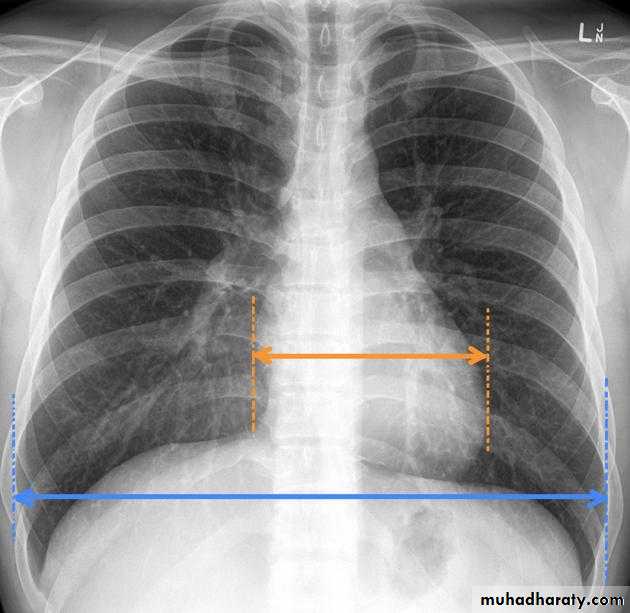
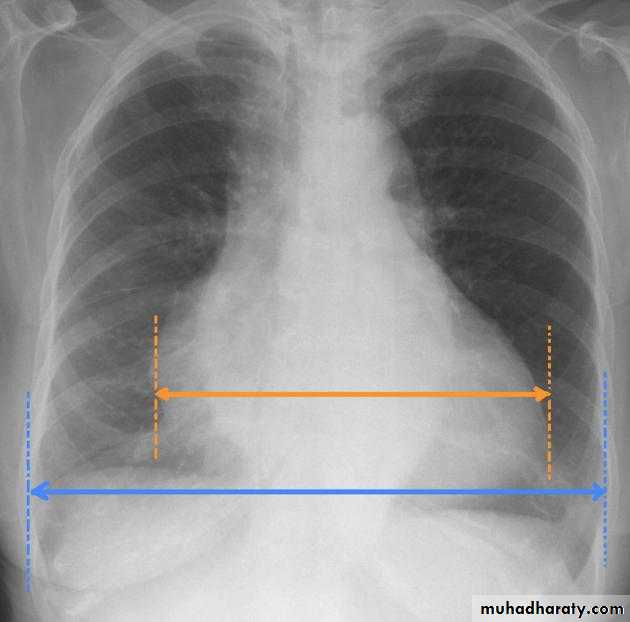
• chest radiography (cardiomegaly is suggestive of hypertensive heart disease);
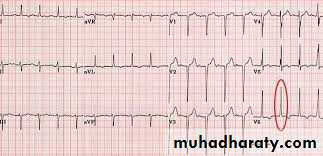
• ECG (may indicate ischemic heart diseases);
• serum urea and electrolytes (deranged in hypertensive renal disease and endocrine causes of secondary hypertension);
Measurement of cardiothoracic ratio ( CTR)
• urine testing (blood and protein suggests renal disease).
Treatment :• Relaxation, weight loss, high-fiber diet, reduction in salt intake, restricting alcohol consumption, restricting caffeine intake, stopping smoking and taking more exercise and avoidance of acute emotions.
• Antihypertensive therapy; the minimum dose should be used with minimum side effects.
Antihypertensive agents
Diuretics: these includeThiazide diuretics like Chlorothiazide,
Loop diuretics like Furosemide,
Potassium-sparing diuretics like Amiloride,
Aldosterone receptor blocker like Spironolactone, or a combination like Aldactazide.
Angiotensin-converting enzyme (ACE) inhibitors; like Captopril, Enalapril, ramipril).
Angiotensin receptor blockers (ARBs); like Candesartan and losartan.
Beta-adrenergic blockers; these are either Cardio-selective like Atenolol, or nonselective like propranolol.
Calcium-channel blockers (CCBs); like Amlodipine, Nifedipine, Verapamil.
Alpha 1-adrenergic blockers; like Doxazosin, Prazosin.
Combined alpha and beta blockers; like Carvedilol.
Central alpha2-agonists and centrally acting drugs (Sympatholytics); like (Clonidine, methyldopa).
Vasodilators; like Hydralazine,. and Minoxidil.
Malignant (accelerated) hypertension
Accelerated hypertension (systolic >200 mmHg, diastolic > 130 mmHg) typically affects young adults, especially those of African or Afro Caribbean heritage and, like essential hypertension, often causes no symptoms until complications develop. It may present with:headaches,
visual impairment,
nausea,
vomiting,
fits (seizures)
or acute cardiac failure.
The chief complication is severe ischemic damage to the kidneys and renal failure, which can be fatal within 1 year of diagnosis.
Other causes of death are cardiac failure or cerebrovascular accidents.
Life threatening accelerated hypertension requires urgent hospital admission with the aim to reduce the blood pressure slowly with oral antihypertensives. Rarely, intravenous antihypertensives (sodium nitroprusside) are used but a sudden drop in blood pressure may result in a stroke (cerebral infarction), thus it should be avoided. Vigorous treatment, if started before renal damage is too far advanced, can greatly improve the life expectancy. About 50% of such patients can now expect to live for at least 5 years.
Dental management
The first task is to identify patients with hypertension, both diagnosed and undiagnosed. A medical history, including the diagnosis of' hypertension, treatment, identification of antihypertensive drugs, compliance of the patient, the presence of symptoms associated with hypertension, and the level of stability of the disease, should be obtained.
Blood pressure measurements should be routinely performed for all new patients and at recall appointments, also for patients who are not compliant with treatment, who are poorly controlled, or who have comorbid conditions such as heart failure, previous MI, or stroke.
The main concerns when one is providing dental treatment for a patient with hypertension:
1. During the course of treatment, the patient might experience an " acute elevation in blood pressure that could lead to serious Outcome such stroke or MI. This acute elevation in blood pressure could result from the release of endogenous catecholamine in response to stress and anxiety, from injection of exogenous catecholamine in the form of vasoconstrictors in the local anesthetic, or from absorption of a vasoconstrictor from the gingival retraction cord.2. Potential drug interactions between the patient's antihypertensive medications and the drugs prescribed and oral adverse effects that might be caused by antihypertensive medications.
Based on blood pressure measurements, the dental management is as follows:
Dental managementBlood pressure
Any treatment can be provided
≤120/80
Any treatment can be provided but encourage the patient to seek medical consultation
≥120/80 but ˂140/90
Any treatment can be provided but encourage the patient to seek medical consultation
≥140/90 but ˂160/100
Any treatment; consider intraoperative monitoring of blood pressure for upper level stage 2, treatment should be treatment if blood pressure rises above 170/109. the patient should be referred to physician promptly.
≥160/100 but ˂180/110
Any elective treatment is deferred and the patient is referred to physician. Only emergency treatment is provided. ( the patient should be managed in consultation with physician, and measures such as intraoperative blood pressure monitoring, ECG monitoring, establishment of an IV line, and sedation may be used. The decision must always be made as to whether the benefit of proposed treatment outweigh the potential risks.
≥180/110
Once it has been determined that the hypertensive patient can be safely treated, the following should be considered:
• Stress/anxiety reduction.
• Establishment of good rapport.
• Short, morning appointments.
• Consider premedication with sedative/anxiolytic like Diazepam 2-5 mg the night before surgery and/or 1 hour before surgery
• Consider the use of nitrous oxide/oxygen (conscious sedation), ensure adequate oxygenation at all times, especially at the termination of administration. Hypoxia is to be avoided because of the resultant elevation in blood pressure that may occur.
• Slow position changes to prevent orthostatic hypotension.
• Consider periodic intraoperative blood pressure monitoring for patients with upper level stage 2 hypertension; terminate appointment if blood pressure rises above 179/109.
• Obtain excellent local anesthesia; adrenalin in modest amounts is acceptable. One or two cartridges of 2% lidocaine with 1:100.000 adrenalin are of little clinical significance in most patients with hypertension. Use of more than this amount may well be tolerated but with increasing risk for adverse hemodynamic changes. Intravascular injections should be avoided through the use of aspirating syringes.
• Avoid the use of adrenalin-impregnated gingival retraction cord because these cords contain highly concentrated adrenalin, which can be quickly absorbed through the gingival sulcular tissues, resulting in tachycardia and elevated blood pressure.
• Noradrenalin and levonordefrin should be avoided in patients with. hypertension because of their comparative excessive alphal stimulation.
• The use of adrenalin is generally not advised in patients with uncontrolled or severe hypertension, and indeed. However, if urgent treatment becomes necessary, a decision must be made about the use of adrenalin, which will be dictated by the situation.
• Available reports and clinical experience suggest that adrenalin small doses of one to two cartridges 100.000 adrenalin can be used safely in most patients
Oral Manifestations
No oral complications have been associated with hypertension itself.Patients with malignant hypertension have been reported to occasionally develop facial palsy.
Patients with severe hypertension have been reported to bleed excessively after surgical procedures or trauma.
Patients who take antihypertensive drugs, especially diuretics, may report dry mouth.
Lichenoid reactions have been reported with thiazides, methyldopa,
propranolol, and labetalol.
ACE inhibitors may cause neutropenia, resulting in delayed healing or bleeding, non-allergic angioedema and burning mouth.
All calcium channel blockers may cause gingival hyperplasia