Orthodontics
Dr.Omar S.M.J.AliPhD Orthodontic
Introduction
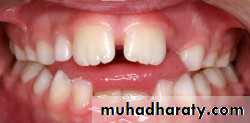
Orthodontics is a specialty of dentistry that is concerned with the study and treatment of malocclusions (improper bites), which may be a result of tooth irregularity, disproportionate jaw improved bite (occlusion).According to American Board of orthodontics
“Orthodontics is that specific area of dental practice that has as its responsibility the study and supervision of the growth and the development of the dentition and its related anatomical structures from birth to dental maturity, including all preventive and corrective procedures of dental irregularities requiring the repositioning of teeth by functional or mechanical means to establish normal occlusion and pleasing facial contours”.
Definition of Orthodontics

Orthodontic treatment of malocclusions and craniofacial abnormalities, by ensuring proper alignment of the teeth, harmonious occlusal and jaw relationship, may improve mastication, phonation, facial aesthetics, with beneficial effects on the general and oral health .
Definition of Orthodontics
Orthodontics includes the study of growth and development of the jaws and face particularly ,and the body generally as influencing the position of teeth ;the study of action and reaction of internal and external influences on the development and the prevention and correction of arrested and perverted development”
Aims of orthodontic treatment
• Functional efficiency: It depends upon correct relationship of teeth to each other and their orientation to skull as a whole to permit a satisfactory functioning of orofacial apparatus.• Structural balance :stable orthodontic treatment is best achieved by maintaining a balance between dentoalveolar system, the skeletal system and soft tissue.
• Esthetic harmony: It is a matter of proportion in shape, size and orientation of dental organs as a whole in their relationship to other facial factors.
Benefits of orthodontic treatment:
• Orthodontic treatment may aid in eliminating or reducing• three types of adverse effect for the patient:
• Psychosocial function.
• Oral function.
• Dental disease.
INDICATIONS FOR ORTHODONTIC TRETMENT:
Unattractive facial esthetic.Dysfunction of TMJ.
Susceptibility to dental caries.
Susceptibility to periodontal disease.
Impaired speech caused by malposition of teeth and\or jaws.
Trauma
Indication of orthodontic treatment
1.dentalcaries, impacted , trauma , periodontal.


Indication of orthodontic treatment
2.functional
Habit , speech ( phonation) , chewing.Indication of orthodontic treatment
3.Psychology
Esthetic , phonetic.
Indication of orthodontic treatment
4- TMJ to eliminate (TMD)
CONTRAINDICATIONS OF ORTHODONTIC TREATMENT:
• 1. Poor oral hygiene and lack of cooperation.• 2. Lack of bony support for the dentition.
• 3. Poor general or mental health.
• 4. Lack of interest.
• 5. Medical compromised.
Types of orthodontic treatment
Preventive orthodonticsPrevention in orthodontics means such arrangements contributing to favourable development of the face, jaws, teeth and establishment of normal dentofacial relations.
Preventive orthodontics
Prenatal
General developing fetus
Mother protection( radiation , infection , improper diet , wrong position , injury birth …)
Preventive orthodontics
Postnatal1-Caries control
2-Prevent early extraction deciduous teeth
3-Spacemaintainer
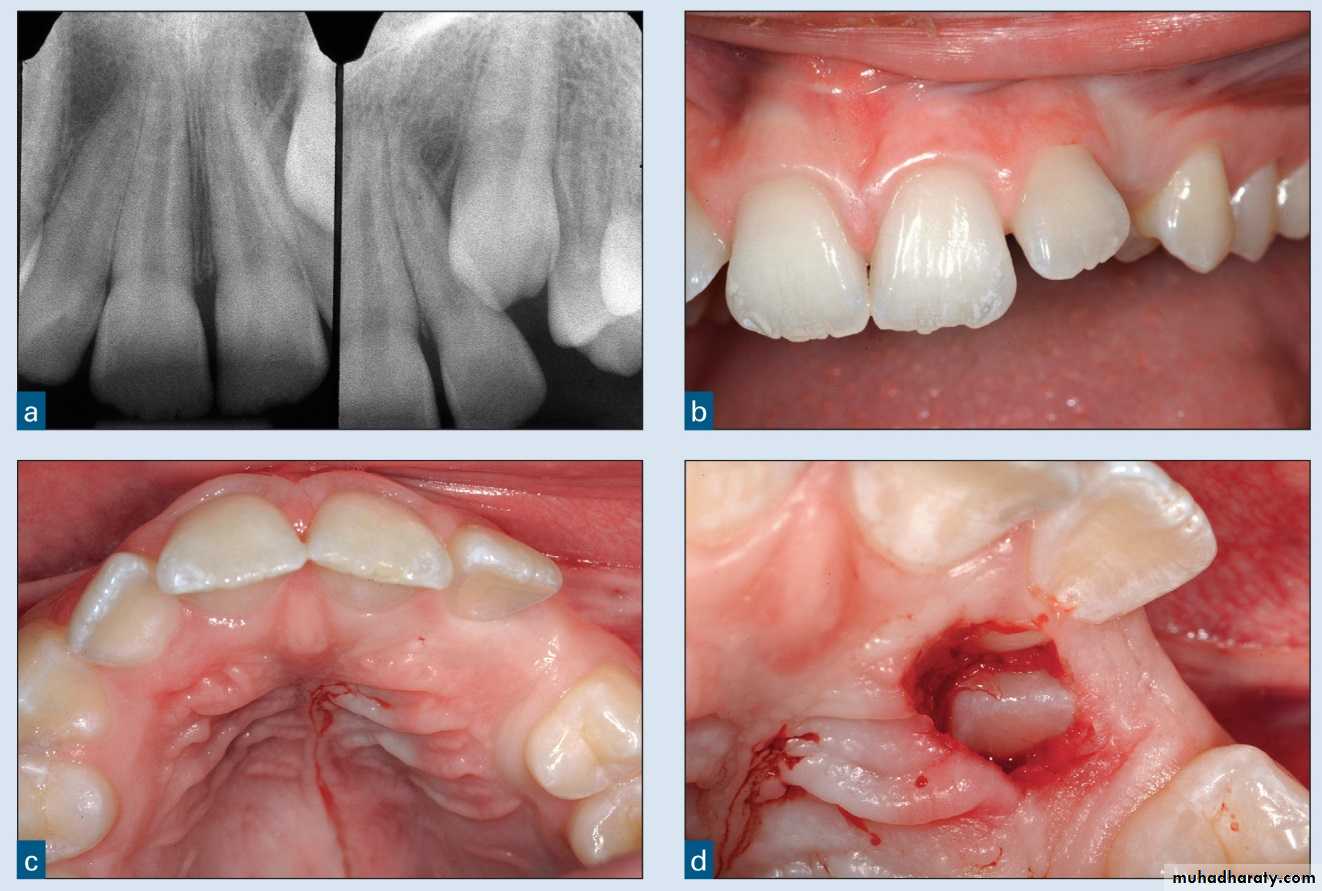
4-Extraction of supernumerary teeth
5-Extraction of prolonged retained deciduous teeth
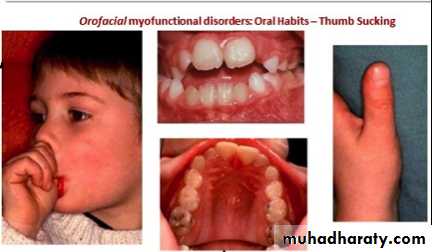
6-Eliminate bad habit
7-Fluoridation
8-Balancing extraction deciduous teeth (c ) ( midline shift )
9-Right nutrition
Types of orthodontic treatment
Interceptive orthodonticsThe phase of the science and art of orthodontics employed to recognize and eliminate potential irregularities and malpositions in the developing dentofacial complex.
Interceptive orthodontic
Serial extraction
Eliminate initial crowding and cross bit
Eliminate bad habit
Remove frenum attachment
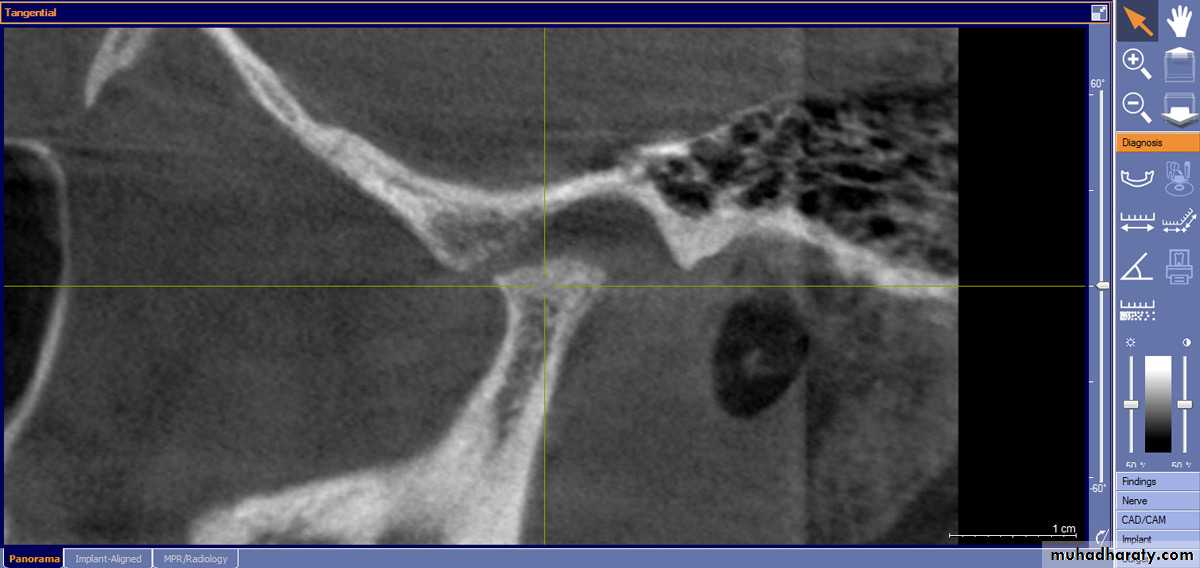
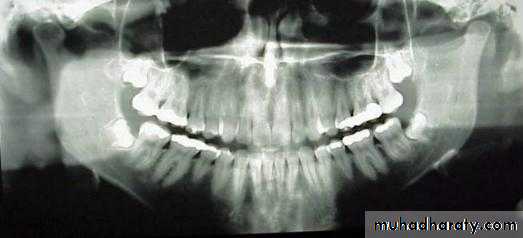
Remove pathologic condition ( cyst , lesion , granuloma …....)
Remove supernumerary teeth
Types of orthodontic treatment
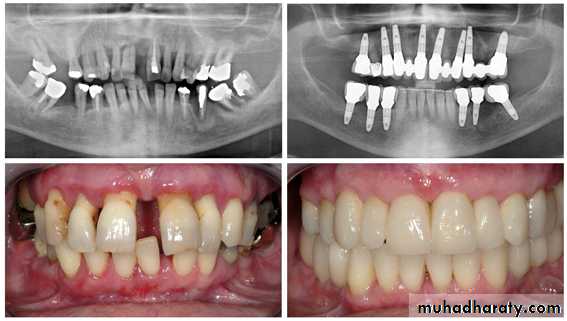
Corrective orthodonticsIt employs certain technical procedures to reduce or correct the malocclusion and to eliminate the possible sequelae of malocclusion.
Types of orthodontic treatment
Surgical orthodontics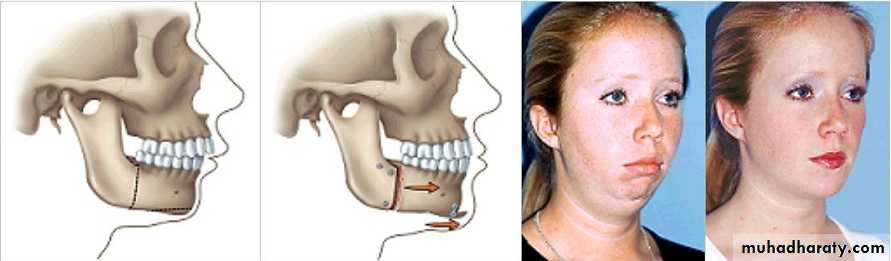
SIDE EFFECTS AND COMPLICATIONSHYPOTHETICALLY LINKED TO ORTHODONTICS
Dental crown: decalcifications, decays, tooth wear, enamel cracks and fractures;discolorations, deterioration of prosthetic crown (as fracturing a ceramic one duringdebonding). root: root resorption, early closure of root apex, ankylosis. pulp: ischemia, pulpitis, necrosis.
SIDE EFFECTS AND COMPLICATIONSHYPOTHETICALLY LINKED TO ORTHODONTICS
Periodontal gingivitis, periodontitis, gingival recession or hypertrophy, alveolar bone loss,dehiscences, fenestrations,
SIDE EFFECTS AND COMPLICATIONSHYPOTHETICALLY LINKED TO ORTHODONTICS
Temporomandibular joint condylar resorption, temporomandibular dysfunction.
Soft tissues of the oral and maxillofacial region trauma (e.g., long archwires, headgear related), mucosal ulcerations or hyperplasia,chemical burns (e.g., etching related), thermal injuries
SIDE EFFECTS AND COMPLICATIONSHYPOTHETICALLY LINKED TO ORTHODONTICS
Unsatisfactory treatment outcome inadequate morpho-functional, aesthetic or functional final result, relapse, failure to complete treatment due to treatment dropout.
Psychological
• teasing, behavioral changes of patients and parents; discomfort associated with pain.
• presence and aesthetic look discontents during orthodontic appliance usage.
SIDE EFFECTS AND COMPLICATIONSHYPOTHETICALLY LINKED TO ORTHODONTICS
Gastro-intestinalaccidental swallowing of small parts of the orthodontic device (tubes, brackets);Allergies to nickel or latex;Cardiac infective endocarditis; Cross infections from doctor to patient, patient to doctor, patient to patient.
CLASSIFICATION OF MALOCCLUSION
NEED FOR CLASSIFICATION
• Grouping of orthodontic problems.• Location of problems to be treated.
• Diagnosis & treatment plan.
• Comparison of different types of malocclusion.
• For self-communication.
• Documentation of problems.
• Assessment of treatment effects of orthodontic appliances.
QUESTIONNAIRE, INTERVIEW
CLINICAL EXAMINATIONANALYSIS OF DIAGNOSTIC RECORDS
DATA BASE
PROBLEM LIST = DIAGNOSIS
CLASSIFICATION

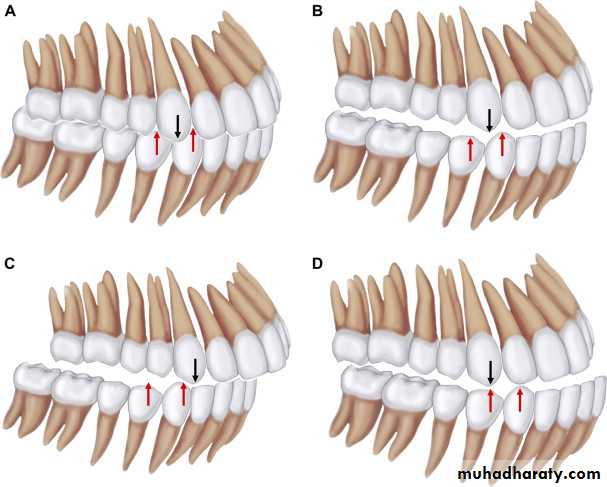
ANGLE’S CLASSIFICATION OF MALOCCLUSION
In 1899 Edward H. Angle published the first classification of malocclusion.
The classifications are based on the relationship of the mesiobuccal cusp of the maxillary first molar and the buccal groove of the mandibular first molar.
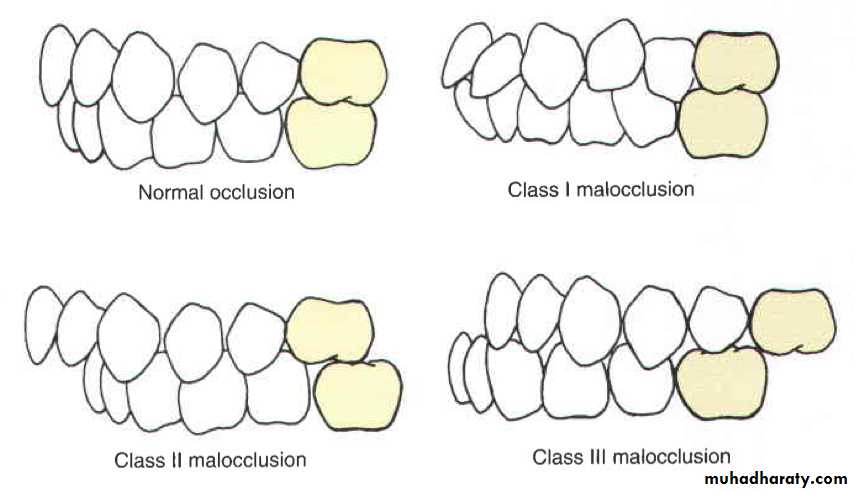
ANGLE’S CLASSIFICATION OF MALOCCLUSION
CLASS I MALOCCLUSIONCLASS II MALOCCLUSION
CLASS III MALOCCLUSION
DIVISION 1
DIVISION 2CLASS III
PSEUDO CLASS III
SUB-DIVISION
SUB-DIVISION
CLASS I MALOCCLUSION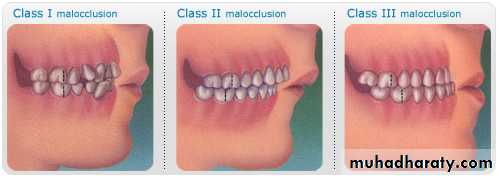
THE MESIOBUCCAL CUSP OF THE UPPER FIRST PERMANENT MOLAR OCCLUDES WITH THE MESIOBUCCAL GROOVE OF THE LOWER FIRST MOLAR, BUT LINE OF OCCLUSION IS INCORRECT BECAUSE OF MALPOSED TEETH, ROTATIONS OR OTHER DISCREPANCIES.
CLASS II MALOCLUSION
THE MESIOBUCCAL CUSP OF THE LOWER FIRST PERMANENT MOLAOCCLUDES DISTAL TO THE CLASS I POSITION.Condition when class II molar relationship is present with proclined upper central incisors.
There is an increase in overjet.

CLASS II DIVISION 1
Condition when class II molar relationship is present with retroclined upper central incisors, upper lateral incisors may be proclined or normally inclined.
Overjet is usually minimal or may be increased.

CLASS II DIVISION 2
CLASS II SUB-DIVISIONCondition when the class II molar relationship exists on only one side with normal molar relationship on the other side.
CLASS III MALOCCLUSION
THE MESIOBUCCAL CUSP OF THE LOWER FIST MOLAR OCCLUDES MESIAL TO THE CLASS I POSITION.PSEUDO CLASS III MALOCCLUSION
Due to occlusal prematurity, when the mandible moves from rest position to occlusion, it slides forward into a pseudo class III position. It’s also known as postural class III.
CLASS III SUB-DIVISION
Condition in which class III molar relationship is present only on one side with normal relation on the other side.
SKELETAL CLASSIFICATION
It considered relationship between maxilla & mandible, in antero-posterior direction.CLASS I:
Maxilla & mandible are inharmony with each other.
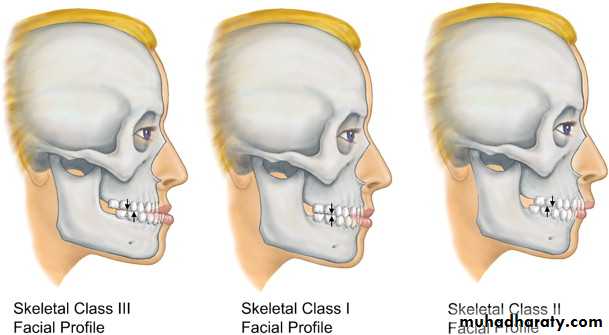
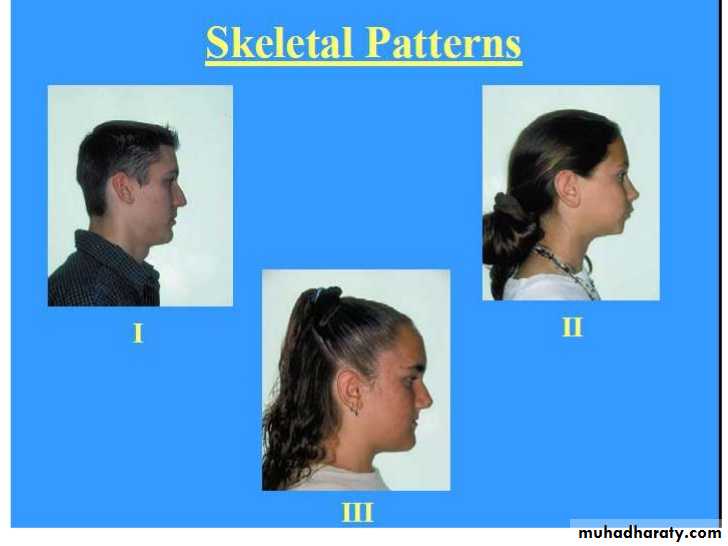
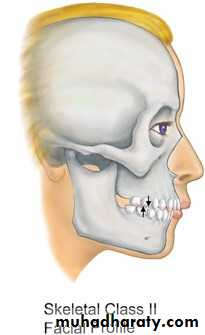
SKELETAL CLASSIFICATION
CLASS II:Maxilla lies ahead of mandible with reference to anterior cranial base. In other words maxilla is pronated.
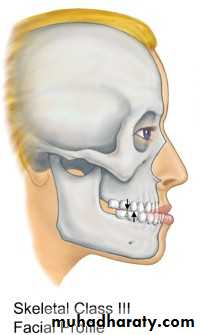
SKELETAL CLASSIFICATION
CLASS III:Maxilla lies posterior to mandible with reference to anterior cranial base. In other words maxilla is retrognathed.
BRITISH STANDARD CLASSIFICATION OF INCISOR RELATIONSHIP (1983)
Based upon incisor relationship, proposed in 1983. Do not consider molar relationship in some cases.CLASS I:
The lower incisor edges occlude withor lie immediately below the
cingulum plateau of upper central incisors.
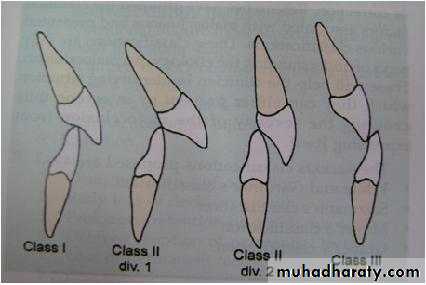
BRITISH STANDARD CLASSIFICATION OF INCISOR RELATIONSHIP
CLASS II:The lower incisor edges lie posterior to the cingulum plateau of the upper incisors.
There are two sub-divisions:
DIVISION 1:
The upper central incisors are proclined or of average inclination & there is an increase in overjet.
DIVISION 2:
The upper central incisors are retroclined. The overjet is usually minimal or may be increased.
BRITISH STANDARD CLASSIFICATION OF INCISOR RELATIONSHIP
CLASS III:The lower incisor edges lies anterior to the cingulum plateau of the upper incisors. The overjet is reduced or reversed.
CANINE CLASSIFICATION
CLASS I :
When the mesial slope of upper canine coincides with the distal slope of lower canine.
CANINE CLASSIFICATION
CLASS II :When the mesial slope of upper canine is ahead of the distal slope of lower canine.
CANINE CLASSIFICATION
Class III :When the mesial slope of the upper canine lies behind the distal slope of the lower canine.
ANDREW’S SIX KEYS (1970)
Andrew extended Angle’s classification:
Correct molar relationship.
Correct crown angulations.Correct crown inclination i.e. Class I incisor relationship.
No rotation present.
Teeth in tight contact with no spacing.
Occlusal plane/ curve of spee should be flat i.e. it should not be deeper
than 1.5mm.
