بسم الله الرحمن الرحيمUrology Symptomatology
د.أشرف إبراهيم العدول
دكتوراه بورد عربي جراحه الكلى
مدرس ـ فرع الجراحة
M.B.Ch.B., CABMS(Uro).
URINARY SYSTEM
AnatomyExtra peritoneal system, composed of two kidneys located in the upper abdomen protected by thoracic cage. - Each weighs about 150 g.Each kidney supplied by main renal artery from aorta, divided into 5 segmental branches and drained by renal vein to the inferior vena cava.
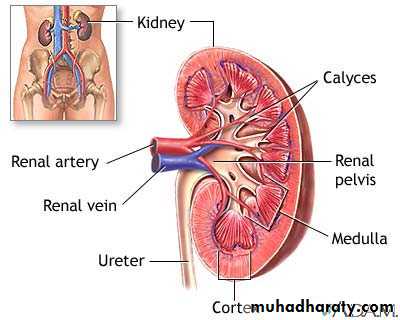
Collecting system
Composed of 3 major calyces, each drains 3-5 minor calyces, joins together to form renal pelvis which is connected to the bladder by muscular tube called the ureter.LEFT RENAL ANATOMY
Kidneys relation to the skeleton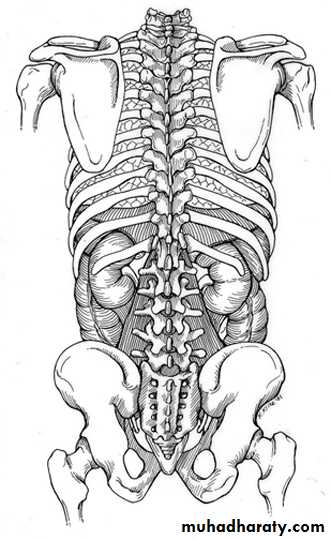
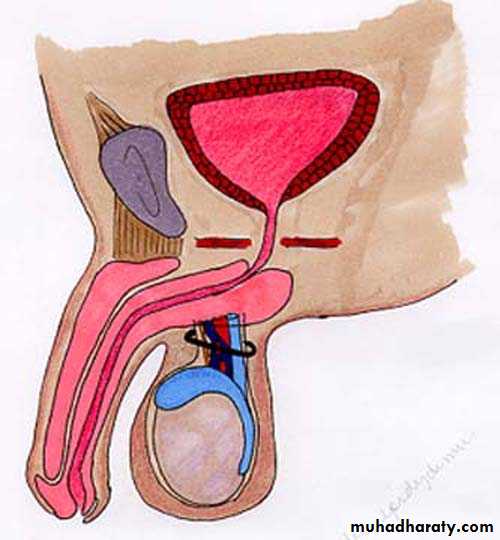
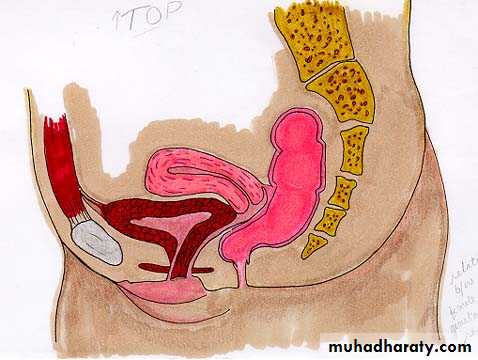
URINARY BLADDER RELATIONS IN BOTH SEXES
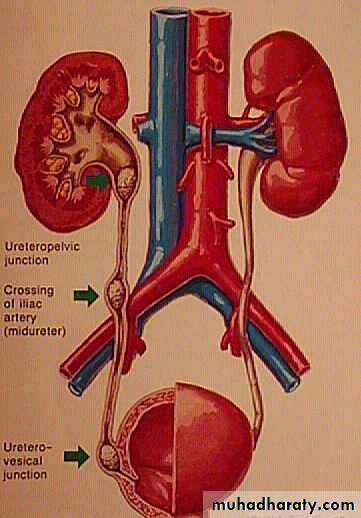
The three common sites of stone impaction in the ureters ( normal narrowing) are :
Pelviureteric junction (PUJ)Where the ureters cross the iliac vessels
Ureterovesical junction (UVJ) which is the narrowest part
FUNCTIONS
1- Excretion of metabolic end products.2- Control body fluid constituents concentration.3- Control acid base balance.4- Hormone and enzymeSymptomatology
The basic approach to the patient in urology is still dependent on taking a complete History, executing a thorough Physical Examination, and performing a Urinalysis.HISTORY
A complete history can be divided into three major components: - The chief complaint - History of the present illness - Past history.Pain
Renal Pain:
Pain is usually caused by acute distention of the renal capsule, generally from inflammation, or obstruction of minor calyx or PUJ by a stone.
- Pain due to inflammation is usually steady Dull aching at the renal angle radiate to the relevant hypochondrium usually associated with fever and general ill health.
Eg.: Pyelonephritis, pyonephrosis, and renal abscess.
- Pain due to obstruction is colicky &fluctuates in intensity.
Pain of renal origin may be associated with gastrointestinal symptoms like nausea & vomiting.
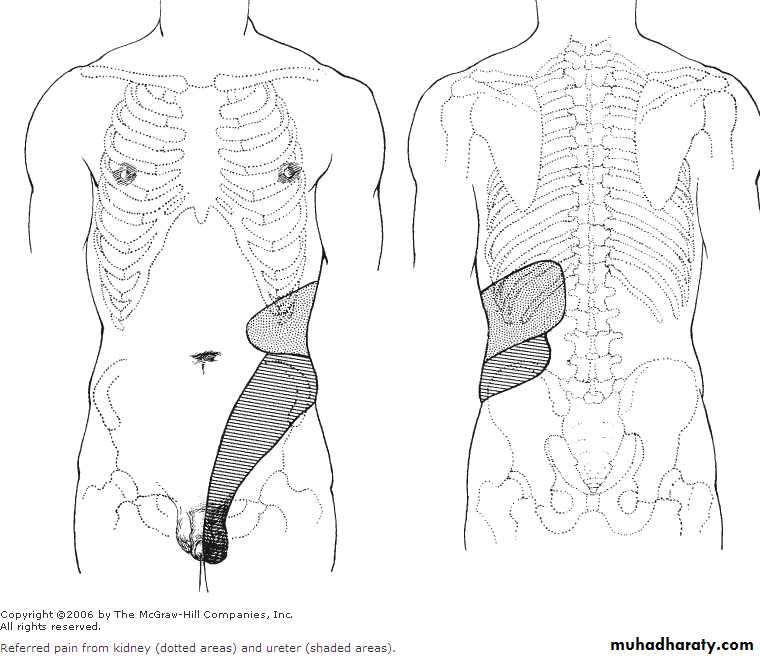
Ureteral Pain (Ureteric Colic):
Sudden severe agonizing pain, started at the loin, radiates to the ipsilateral iliac fossa, suprapubic region, and genitaliaAssociated with nausea, vomiting, and urinary symptoms like hematuria or dysuria.
The patient is rolling around. (Contrast this with the
patient suffering from peritoneal pain, who lies still to avoid exacerbating the pain by movement. )
It is ischemic pain
Usually due to acute ureteral obstruction either by stone, clot, crystals, sloughed tissue or papillae.
The site of ureteral obstruction can often be determined by the location of the referred pain. If the cause in the lower ureter the pain radiates to the testicle, labia or inner aspect of the thigh.
Vesical Pain: Suprapubic pain aggravated by vesical filling, relieved by urination. Produced either by overdistention of the bladder as a result of acute urinary retention or by Bladder inflammation (cystitis)
Prostatic pain :
It is secondary to inflammation (Prostatitis) with secondary edema and distention of the prostatic capsule.
Usually felt deep in the rectum, penis, pelvis perineum, suprapubic, low backache, & both iliac fossae.
Urethral pain:
Scalding in nature usually at the tip of the penis but sometimes at its base, usually due to urethritis, cystitis or vesical or urethral calculus.N.B.: Tumors in the GU tract usually do not cause pain unless they produce obstruction or extend beyond the primary organ to involve adjacent nerves.
Testicular Pain :
Primary pain arises from within the scrotum and most commonly secondary to acute epididymo orchitis or torsion of the testicle or testicular appendices or trauma.Because the testicles arise embryologically in close proximity to the kidneys, testicular pain may by referred to the epigastric region.
Also pain arising in the kidneys or retroperitoneum may be referred to the testicles.
Similarly, the dull pain associated with an inguinal hernia may be referred to the scrotum.
Hematuria
The presence of blood in the urine. > 3 RBC /HPF is significant.Hematuria of any degree should never be ignored and, in adults, should be regarded as a feature of urologic malignancy until proved otherwise.
The most common cause of gross hematuria in a patient older than age 50 years is bladder cancer.
Important points about hematuria
- Macroscopical or microscopical? - Initial, terminal or total? - Painless or painful.?
- Intermittent or persistent?- If the patient is passing clots, do the clots have a specific shape ( thread like + ureteric or renal origion)?
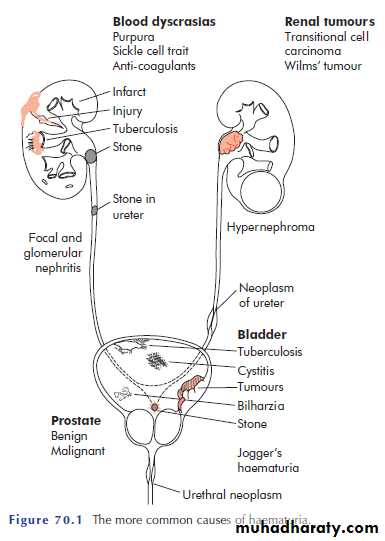
Causes:
- Local cause like stone, UTI, trauma, or malignancy.
- Systemic cause like bleeding tendency
If there is a malignant cause for the haematuria there is usually no pain.
Blood appearing at the beginning of the urinary stream indicates a lower urinary tract cause.uniform staining throughout the stream points to a cause higher up.
Terminal haematuria is typical of severe bladder irritation caused stone or infection.
• Lower Urinary Tract Symptoms
• Irritative Symptoms• Frequency : Increase in the number or times of urination.
• The normal bladder capacity is about 400-500mL
• The normal adult voids 5-6 times per day, with a volume of approximately 300mL with each void. Urinary frequency is due either to increased urinary output (polyuria) or to decreased bladder capacity.
• Causes:
• Systemic: compulsive water drinking, DM, DI or diuretics use.
• Local: stone, infection, BPH or prostatic carcinoma.
Nocturia: nocturnal frequency
Dysuria: painful urination (burning sensation) that is usually caused by inflammation
Urgency : sudden strong desire to urinate that the patient cannot postpone itObstructive Symptoms
Weak stream decreased force (flow) of urination.Urinary Hesitancy a delay in the starting (initiation) of micturition
Intermittency involuntary start-stopping of the urinary stream (interrupted urinary stream).
Postvoid dribbling the terminal release of drops of urine at the end of micturition
Straining use of abdominal musculature to urinate.
Feeling of Incomplete bladder evacuation.
Retention of urine: Inability to pass urine in spite of a full bladder ( due to outlet obstruction).
Acute & chronic
N.B.:
Anuria: complete absence of urine production.Oliguria is present when less than 300 ml of urine is excreted in a day
Incontinence
• Involuntary loss of urine or Inability to control urination.
• Continuous incontinence.
• Stress incontinence.
• Urgency incontinence.
• Overflow urinary incontinence
• Nocturnal Enuresis : Bed wetting (urinary incontinence that occurs during sleep ) Physiological during first 2-3 yr of age
• Urethral Discharge
Pyuria: presence of pus in the urine.
Chyluria: presence of lymph in the urine.Phosphaturia: presence of phosphate crystals in the urine.
Necroturia: presence of necrotic tissue in the urine as in malignancy.
Pneumaturia: presence of air in the urine.
Past History
Past Medical HistoryPast Surgical History
Family History
Smoking and Alcohol Use
Allergies
PHYSICAL EXAMINATION
With the exception of:
Renal and scrotal masses or tenderness & other pathologies.
palpable bladder
abnormal prostate on digital rectal examination.
Penis: Circumcision, Phymosis/Paraphymosis, Epispadias, Hypospadias, Urethral discharge, Superficial ulcers or vesicles, Venereal warts, Meatal stenosis, Balanitis .
urological conditions are most likely to be diagnosed from the history or by investigations.
PHYSICAL EXAMINATION
General ObservationsBimanual examination of the kidney The kidney is lifted from behind with one hand in the costovertebral angle & palpated with t
the other hand
In children and thin women, it may be possible to palpate the lower pole of the right kidney with deep inspiration.
Exam. of the Renal angle
Bladder examination:
A normal bladder in the adult cannot be palpated or percussed until there is at least 150 mL of urine in it.
Percussion is better than palpation for diagnosing a distended bladder.

Scrotal examination
A firm or hard painless mass within the testis should be considered a malignant tumor until proved otherwise.
Transillumination is helpful in diagnosing hydrocele.
Spermatic cord : ( varicocele, fusiform enlargement, thickening of the cord ), absence of vas deference .
Epididymal : size/induration/tenderness .
Prostate Examination:
Digital rectal examination (DRE) should be performed in every male after age 40 years and in men of any age who present for urologic evaluation.Normally, the prostate is about the size of a chestnut and has a firm consistency similar to that of the contracted thenar eminence of the thumb.
Pelvic Examination in the Female
Investigations
I- URINALYSIS (General urine examination: GUE)complete urinalysis includes physical, chemical, and microscopic analyses.
Physical: color, pH, & Specific Gravity
Color : yellowish
Turbidity :phosphaturia , Pyuria
Specific Gravity and Osmolality :
Specific Gravity usually varies from 1.003 to 1.030.
Osmolality is a measure of the amount of material dissolved in the urine and usually varies between 50 and 1200 mOsm/L.
pH the average pH varies between 4.5 and 8.0. Persistently alkaline urine (pH > 8.0) suggest infection with urea-splitting organism such as Proteus mirabilis
Biochemical Examination of Urine "Dipstick" = a strip coated with chemicals for measuring the urine pH and for detecting the presence of glucose, protein or blood; bilirubin, urobilinogen, ketones and nitrites can also be detected.
The abnormal substances commonly tested for with a dipstick include (1) Hemoglobin, (2) protein, (3) glucose, (4) ketones, (5) Electrolytes, (6) myoglobin , and (7) urobilinogen and bilirubin.
Protein
The amount of protein in the urine is normally less than 100 mg/24 hr. Dipstick will only detect levels greater than 300 mg/lTransient proteinuria (e.g. UTI)
persistent (glomerulopathia)
Glycosuria
Usually diabetes mellitus, rarely renal glycosuria
Microscopic analysesCells (RBC , Leukocytes , Epithelial cells , Renal tubular cells) Casts : cast is a protein coagulum that is formed in the renal tubule (The presence of protein casts suggests disease affecting the renal parenchyma)
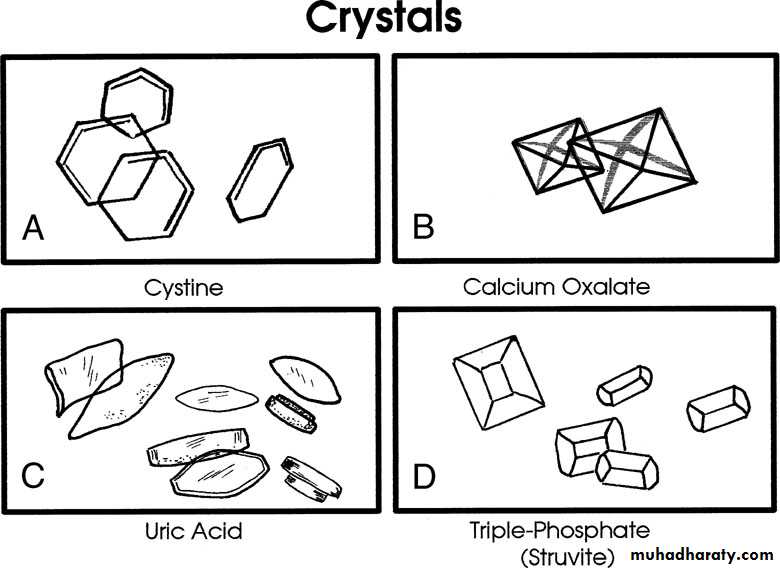
Crystal
Bacteria
Five bacteria/HPF reflects colony counts of about 100,000 bacteria/mLThe finding of any bacteria in a properly collected midstream specimen from a male should be further evaluated with a urine culture
Mid stream urine for c&s.
Early morning sample for AFB
Cytology: poorly differentiated transitional cell tumours anywhere in the urinary tract.
Yeast
Parasites : Schistosoma ovum

Bacteriological culture
Culture & sensitivity (C&S) of a clean-catch midstream specimenThe specimen should be plated out promptly or refrigerated until processing to prevent multiplication of bacteria after voiding.
Significant infection is present if there are more than 100 000 (= 10 5 ) organism/ml , whilst counts less than 10 000 (=10 3 )/ml suggest contamination.
If there are pus cells in the urine but there is no growth on the routine culture media (sterile pyuria), it is worth testing for more fastidious organisms.
Multiple early-morning urine specimens must be cultured on L0wenstein–Jensen medium to detect urinary tract tuberculosis.
Chlamydia