1
Hypoxic-ischemic encephalopathy (HIE);
(cont.)
Clinical manifestations;
*Intrauterine;
1
growth restriction and
2
increased vascular resistances may be the 1
st
manifestation of fetal hypoxia.
*During labor;
1
Variable or late deceleration pattern
of continuous heart rate recording, fetal heart rate slows down,
and beat-to-beat variability declines.
2
Fetal scalp blood analysis may show a pH <7.20.
These signs should lead to the administration of high concentrations of
1
oxygen to the mother and
2
immediate delivery to avoid fetal death or CNS damage.
*At delivery;
1
the presence of yellow, meconium-stained amniotic fluid is evidence that fetal distress had occurred.
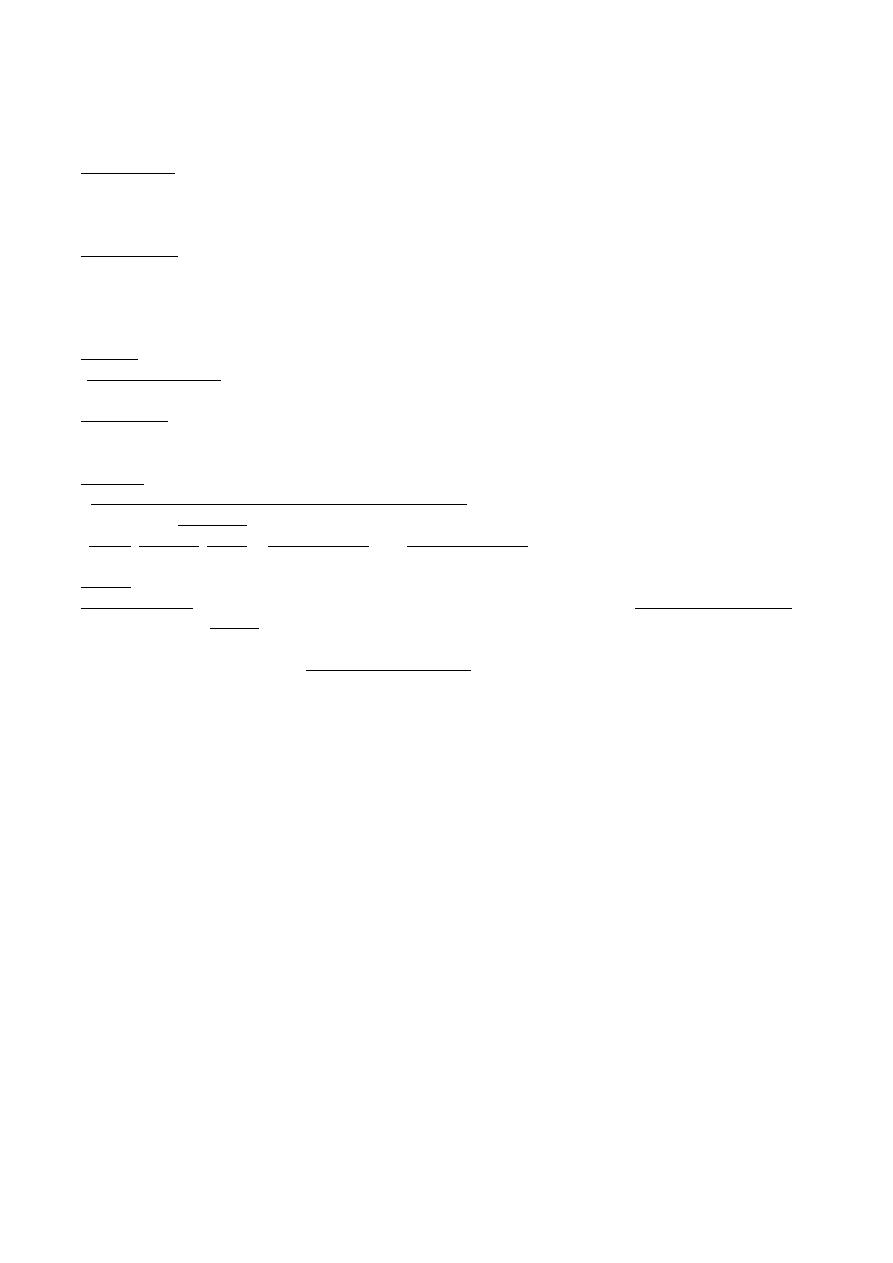
*At birth; these infants are
1
frequently depressed and fail to breathe spontaneously. During the ensuing hours, they
2
may remain hypotonic or change from hypotonic to hypertonic, or their tone may appear normal.
3
Pallor, cyanosis, apnea, a slow heart rate, and unresponsiveness to stimulation.
*Later;
Cerebral edema may develop during the next 24 hr and result in profound brain stem depression.
During this time, seizure activity may occur; it may be severe and refractory to the usual doses of
anticonvulsants.
In addition to CNS dysfunction, systemic hypoperfusion occurs in 80% of cases including;
heart failure and cardiogenic shock, hypotension, persistent pulmonary hypertension, respiratory
distress syndrome, gastrointestinal perforation, hematuria, and acute tubular or cortical necrosis,
adrenal hemorrhage, inappropriate secretion of antidiuretic hormone, and metabolic derangements.
After delivery, hypoxia is due to respiratory failure and circulatory insufficiency. During the initial
hours after an insult, infants have a depressed level of consciousness. Periodic breathing with apnea or
bradycardia is present, but cranial nerve functions are often spared with intact papillary responses and
spontaneous eye movement. Seizures are common with extensive Injury. Hypotonia is also common as
an early manifestation.
2
HIE in term infants:
Signs
Stage 1
Stage 2
Stage 3
Consciousness
Hyper-alert
Lethargic
Stuporous, coma
Muscle tone
Normal
Hypotonic
Flaccid
Posture
Normal
Flexion
Decrebrate
Tendon reflexes/ clonus
Hyperactive
Hyperactive
Absent
Myoclonus
Present
Present
Absent
Moro reflex
Strong
Weak
Absent
Pupils
Mydriasis
Miosis
Poor light reflex
Seizures
None
Common
Decerebration
EEG
Normal
Low voltage changing to
severe seizure activity
Burst suppression
to iso-electric
Duration
<24hr if progresses;
or may remain
normal
24hr to 14 days
Days to weeks
Outcome
Good
Variable
Death, severe
deficits
Decrebrate
positioning
Pathological correlation of preterm infant with hypoxic ischemic encephalopathy
Pathology
Clinical sign
Periventricular leukomalacia
Spastic diaplegia
Status marmoratus of basal ganglia
Dystonia, choreoathetosis
Thalamus
Mental retardation
Cerebral cortex
Mental retardation
Pathological correlation of full term infant with hypoxic ischemic encephalopathy
Pathology
Clinical sign
Parasagittal cortical and subcortical neuronal necrosis
Spastic quadriplegia, especially arms. Intellectual deficits
and cortical atrophy, focal seizures and hemiplegia
Cerebellum
Ataxia
Brain stem
Pseudobulbar palsy
Diagnosis;
*Diffusion-weighed MRI: is the preferred imaging modality because of its increased sensitivity and
specifity.
*CT scans: are helpful in identifying focal hemorrhage, diffuse cortical injury, and damage to the basal
ganglia; CT has limited ability to identify cortical injury within the 1
st
few days of life.
3
*Amplitude integrated EEG (aEEG): has a good reliability & positive predictive value of 85% for
infants who will have adverse neurodevelopmental outcome.
*Ultrasound: has limited utility in evaluation of hypoxic injury in the term infant; it is preferred in
evaluation of the preterm infant.
Treatment;
*Phenobarbital is the drug of choice, is given with an intravenous loading dose (20 mg/kg); additional
doses of 5-10 mg/kg (up to 40-50 mg/kg total) may be needed. Phenytoin (20 mg/kg loading dose) or
lorazepam (0.1 mg/kg) may be needed for refractory seizures. Phenobarbital levels should be
monitored 24 hr after the loading dose and maintenance therapy (5mg/kg/24 hr) are begun. Seizures in
HIE may also be due to hypocalcaemia, hypoglycemia, or infection.
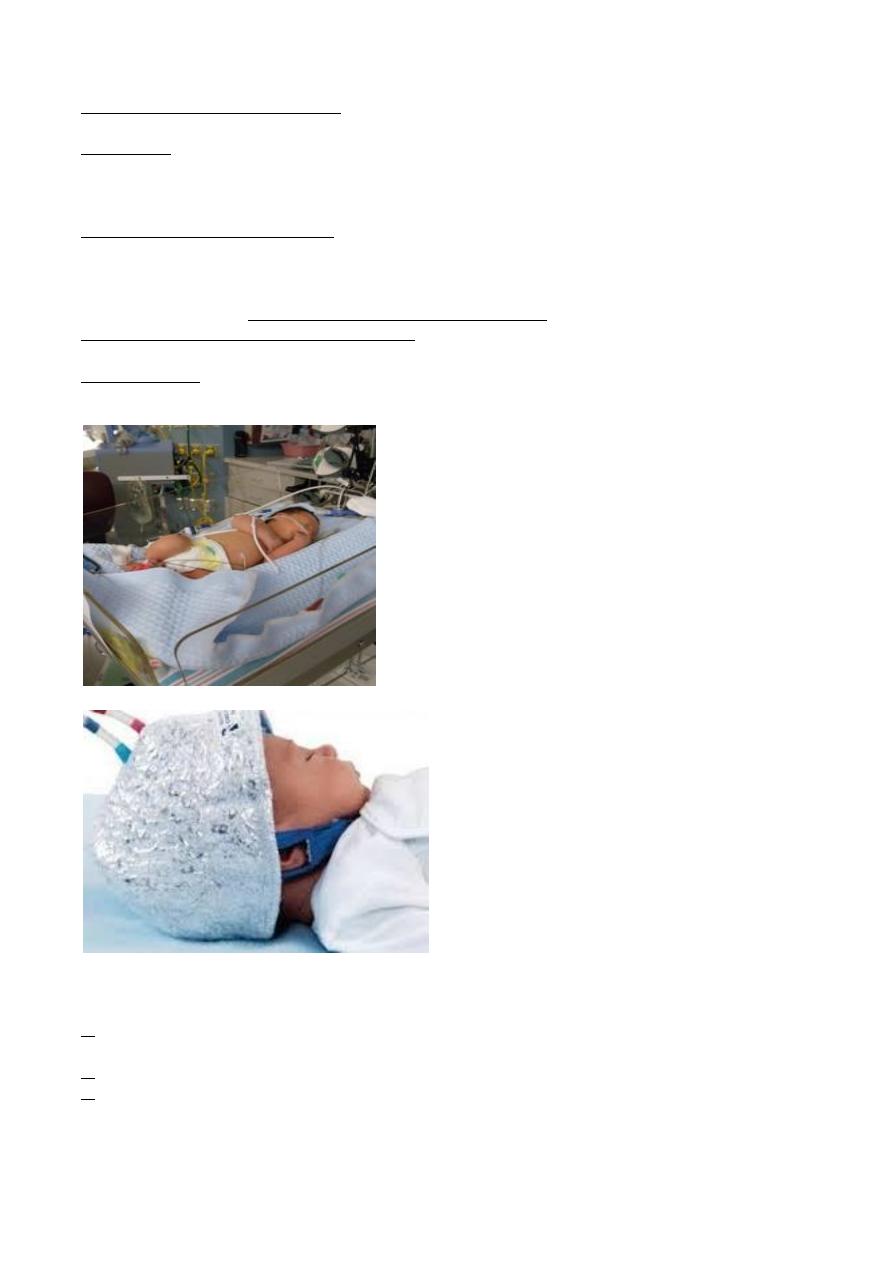
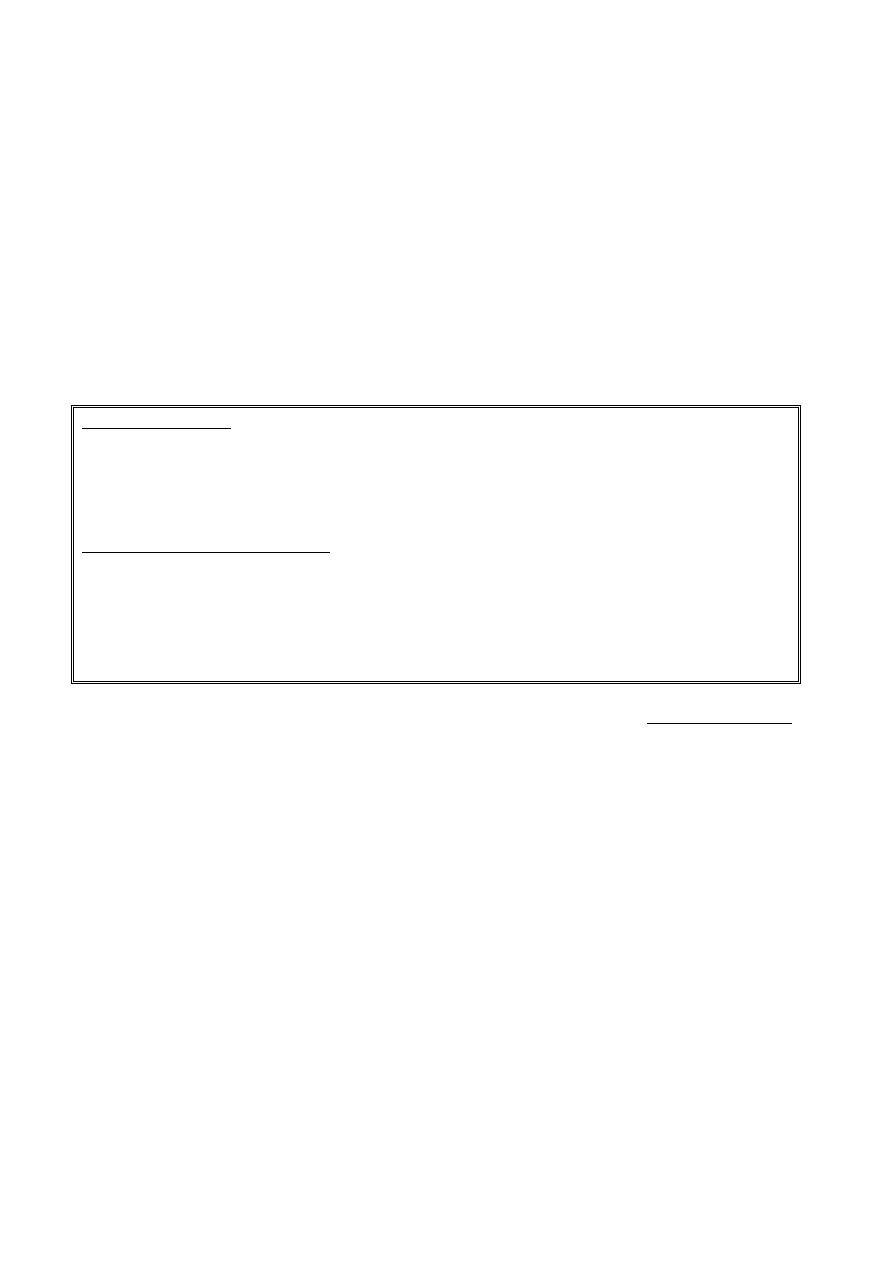
*Systemic or selective cerebral hypothermia for acute management of HIE is promising, as it
decrease metabolism and suppress production of mediators known to be neurotoxic.
*Others include; supportive care for organ dysfunction, careful ventilation, control of blood
pressure, acid-base balance and of possible infection.
Cool-Blanket body hypothermia
Cool-cap body hypothermia
Prognosis;
it varies depending on
1. whether the metabolic & cardiopulmonary complication (hypoxia, hypoglycemia, shock) are
treated,
2. the infant's gestational age (outcome is poorest if the infant is preterm), and
3. the severity of the encephalopathy.
Severe encephalopathy is characterized by flaccid coma, apnea, and refractory seizures, and is
associated with a poor prognosis.
4
*Low Apgar score at 20 min, absence of spontaneous respirations at 20 min of age, and persistence
of abnormal neurological signs at 2 weeks of age also predict death or severe cognitive or motor
deficit.
*Normal MRI and EEG findings are associated with a good recovery, whereas severe MRI and
EEG abnormalities predict a poor outcome.
*Microcephaly and poor head growth during 1
st
year of life also correlate with injury to the basal
ganglia and white matter and adverse developmental outcome at 12 month.
THE PRINCIPLES OF NEONATAL RESUSCITATION;
Preparation for Resuscitation
Immediate, effective resuscitation of the newborn infant can reduce or prevent morbidity and mortality
and to establish adequate spontaneous respiration and cardiac output. Conditions requiring skilled
resuscitation to be available at delivery are;
Intrapartum Problems
• Fetal distress (Persistent late decelerations, severe variable decelerations without baseline variability,
scalp pH <7.25, meconium-stained amniotic fluid and cord prolapse).
• Prolonged, unusual or difficult labor
• Emergency operative delivery
• Vaginal Breech delivery
Medical/Obstetric/Genetic Problems
• Diabetes mellitus • Suspected or confirmed maternal infection
• Substance abuse i.e. drugs • Third trimester bleeding
• Pregnancy-induced hypertension • Abnormal amniotic fluid volume
• Prolonged rupture of membranes • Multiple gestation
• Low-birth-weight infant (<2.5Kg) • Prematurity (<37weeks gestation)
• Isoimmunization i.e.Rh factor incompatibility • Fetal congenital anomalies
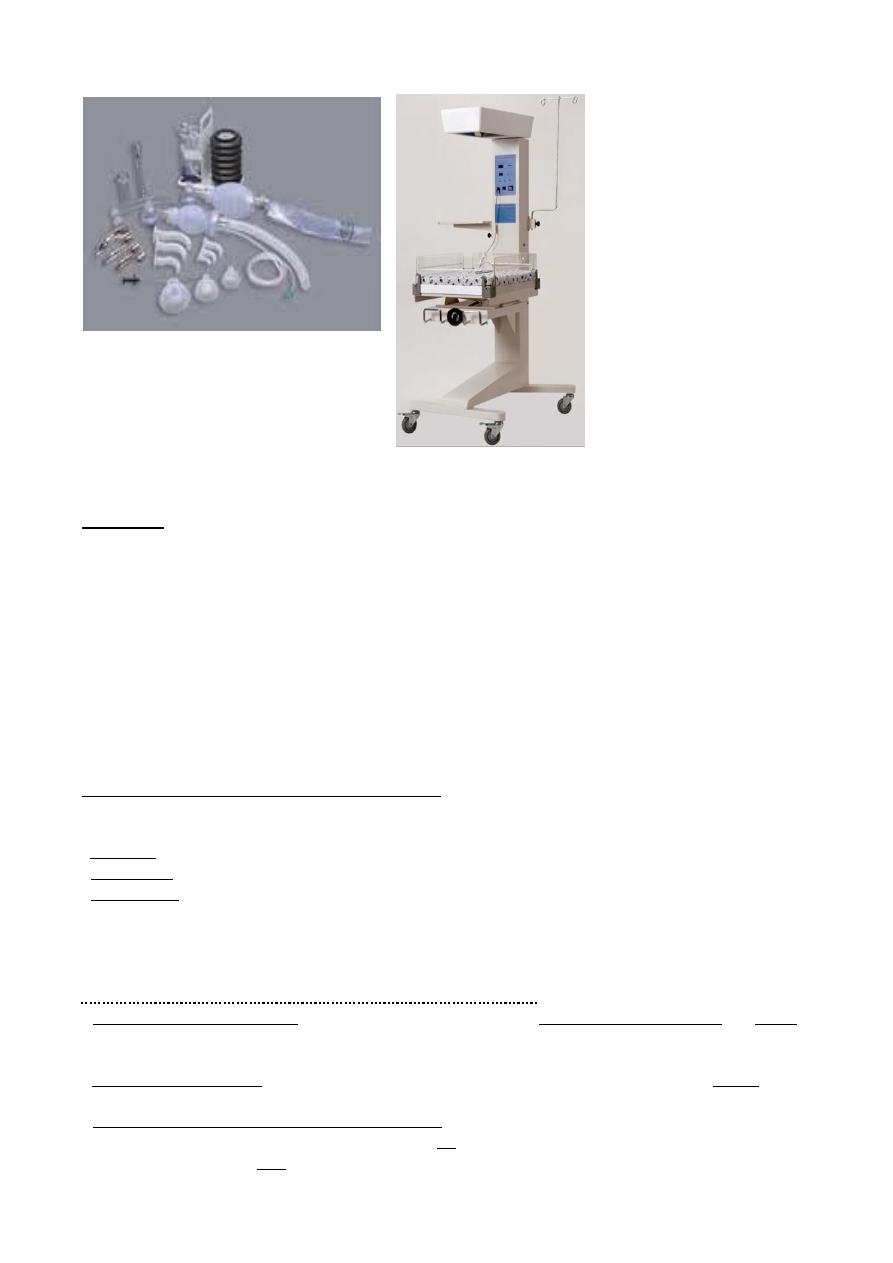
Resuscitation equipment and drugs should always be readily available in resuscitation trolley,
functional, and assembled for immediate use in the delivery room.
1. Radiant warmer with procedure table, stopwatch, light 2. Oxygen source (100%), pulse
oximetry 3. neonatal resuscitation bag 4. Face mask(s) 5. A bulb syringe for suctioning with
feeding tubes 6. Stethoscope 7. Transport incubator with battery-operated heat source and
portable oxygen supply 8. Equipment for continuous monitoring of cardiopulmonary status.
9. Equipped emergency box containing; Laryngoscope, blades, batteries, endotracheal tubes,
airways, Drugs(epinephrine, sodium bicarbonate, naloxone, albumin 5% and N/S), Umbilical
catheterization tray, Syringes, needles, sutures, gloves, alcohol and tape.
5
Immediate steps after birth in an infant in need of resuscitation;
(1) Prevention of heat loss
• Place the infant under a radiant heat source.
• Dry the infant thoroughly and remove the wet linen.
(2) Clearing the airway
• Position the infant supine and flat with the neck slightly extended.
• Suction the mouth then the nasopharynx to clear the airway.
• Turn the head to the side to allow secretions to pool, and then remove with a bulb syringe or
suction catheter. Deep pharyngeal suction (in a child not requiring positive-pressure ventilation or
intubation) should not be performed during the first few minutes after birth to avoid vagal
depression and resultant bradycardia.
(3) Initiation of breathing
• Provide tactile stimulation by rubbing the back or gently slapping the feet
Assess the heart rate, respiratory effort and color.
The steps of neonatal resuscitation following the standard ABCs of resuscitation:
Endotracheal intubation if necessary).
Suctioning and
,
Positioning
Establish an airway,
(
Airway
-
A
•
).
Positive pressure ventilation
tactile stimulation,
(Initiate breathing,
Breathing
-
B
•
).
Medications
Chest compressions,
Maintain circulation,
(
Circulation
-
C
•
At each step of the resuscitation procedure, evaluation is based on the infant's respirations, heart rate, and
color.
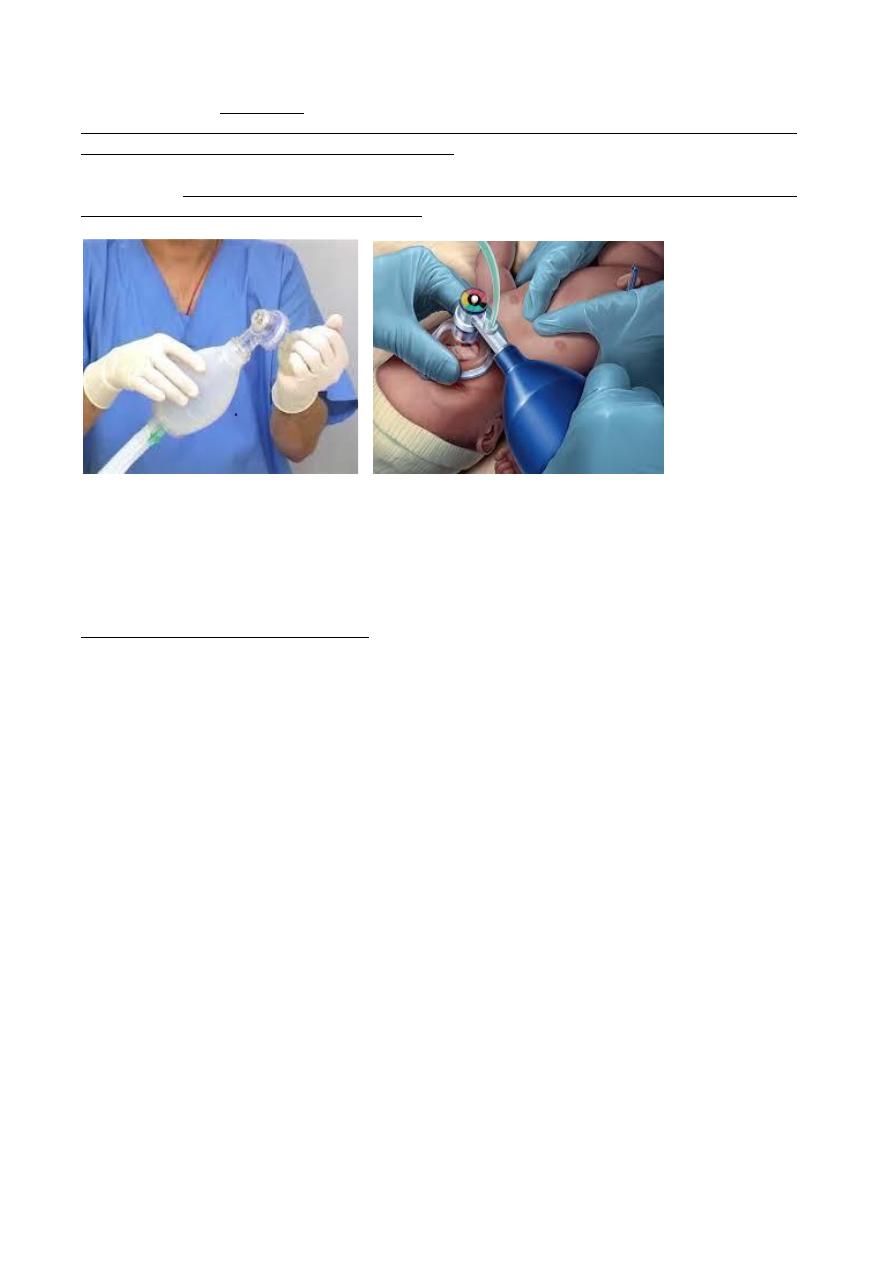
If no respirations are noted or if the heart rate is below 100/min,
1
positive pressure ventilation is given through a tightly fitted face mask and ambu bag for 15-30
sec. In Infants with severe respiratory depression who do not respond to positive pressure
ventilation via ambu bag and mask,
2
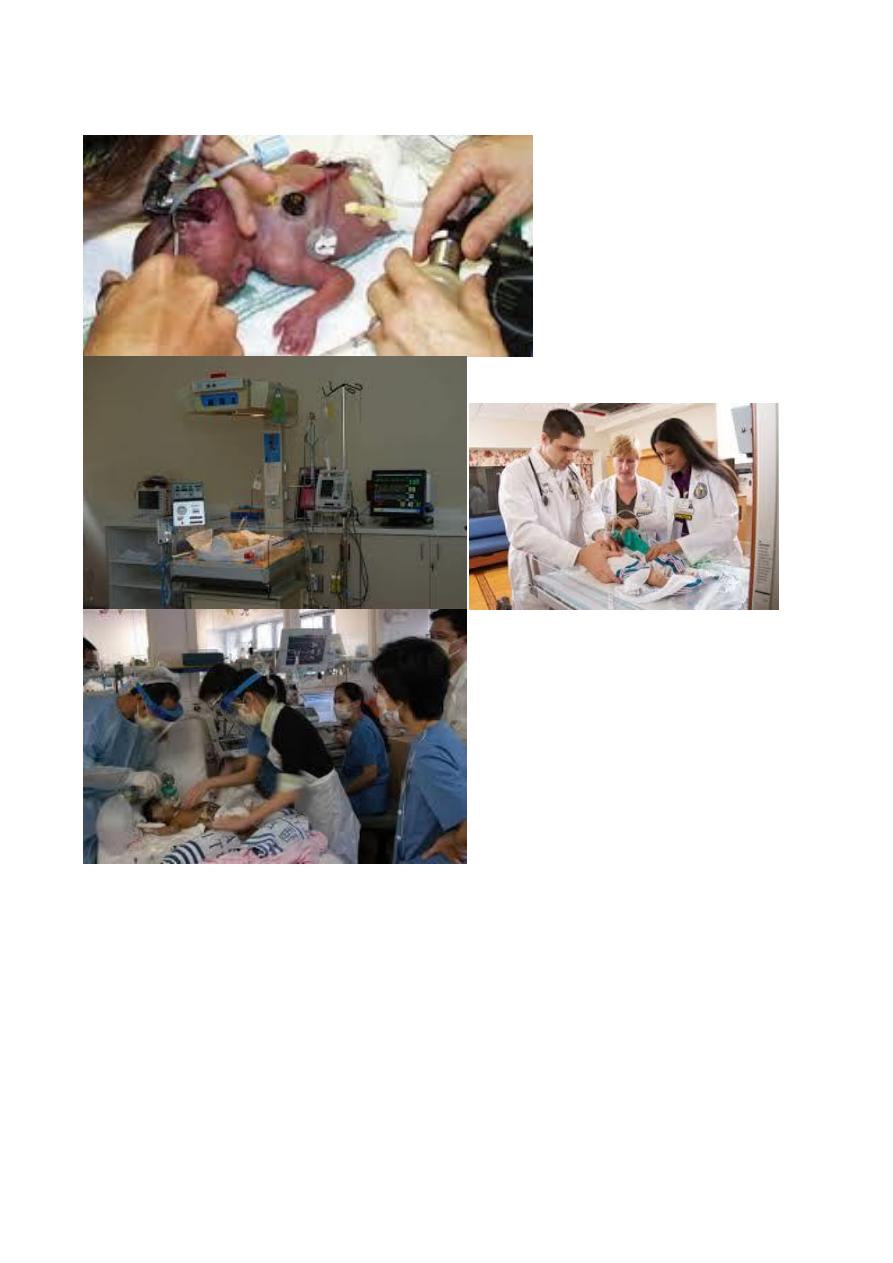
endotracheal intubation should be performed. If the heart rate does not improve after 30 sec with
bag and mask (or endotracheal) ventilation and remains below 100/min,
3
ventilation is continued and chest compression should be initiated over the lower third of the
sternum at ratio of compressions to ventilation is 3:l.
If the heart rate remains <60 despite effective compressions and ventilation,
6
4
administration of epinephrine should be considered.
Persistent bradycardia in neonates is usually due to hypoxia resulting from respiratory arrest and
often responds rapidly to effective ventilation alone. Persistent bradycardia despite what appears to
be adequate resuscitation suggests more inadequate ventilation technique or severe cardiac
compromise. Traditionally, the inspired gas for neonatal resuscitation has been 100% oxygen.
Resuscitation with room air is equally effective.
Although the 1
st
breath normally requires pressures as low as 15-20 cm H
2
O, pressures as high as
30-40 cm H
2
O may be needed. Subsequent breaths are given at a rate of 40-60/min with a pressure
of 15-20 cm H
2
O.
Successful ventilation is determined by;
1. adequate chest rise, 2. symmetric breath sounds, 3. improved pink color, 4. heart rate >100/min,
5. spontaneous respirations, 6. presence of end-tidal CO
2
, and 7. improved tone.
If the infant has respiratory depression and the mother has a history of analgesic narcotic drug
administration within 4 hr prior to delivery, naloxone hydrochloride (0.1 mg/kg) is given while
adequate ventilation is maintained, repeated doses of naloxone may be needed.
Medications are rarely required but should be administered when the heart rate is < 60/min after 30
sec of combined ventilation and chest compressions or during asystole. The umbilical vein can
generally be readily cannulated and used for immediate administration of medications during
neonatal resuscitation.
*Administration of epinephrine (0.1- 0.3 ml/Kg of 10 000 solution, 0.01mg/Kg) via endotracheal
tube or IV may be used, may be repeated every 3-4 min.
*Volume expanders: in acute bleeding and hypovolemia; poor response to other resuscitative
measures(0.9% N/S, 10ml/Kg, IV).
*Sodium bicarbonate: in documented or suspected metabolic acidosis in the presence of
adequate ventilation (2meq/Kg, IV).
*Dobutamine and fluids should be started to improve cardiac output in an infant with poor
peripheral perfusion, weak pulses, hypotension, tachycardia, and poor urine output.
If any meconium staining is present in the amniotic fluid, the obstetrician should suction the
mouth, nose, and hypopharynx immediately after delivery of the head and before delivery of
shoulders.
If the baby is vigorous, with good respiratory effort & Heart rate >100/min, tracheal intubation to
aspirate meconium should not be attempted, otherwise in a depressed infant with poor muscle tone
and or a heart rate < 100/min, tracheal intubation and suctioning should be performed.
7