1
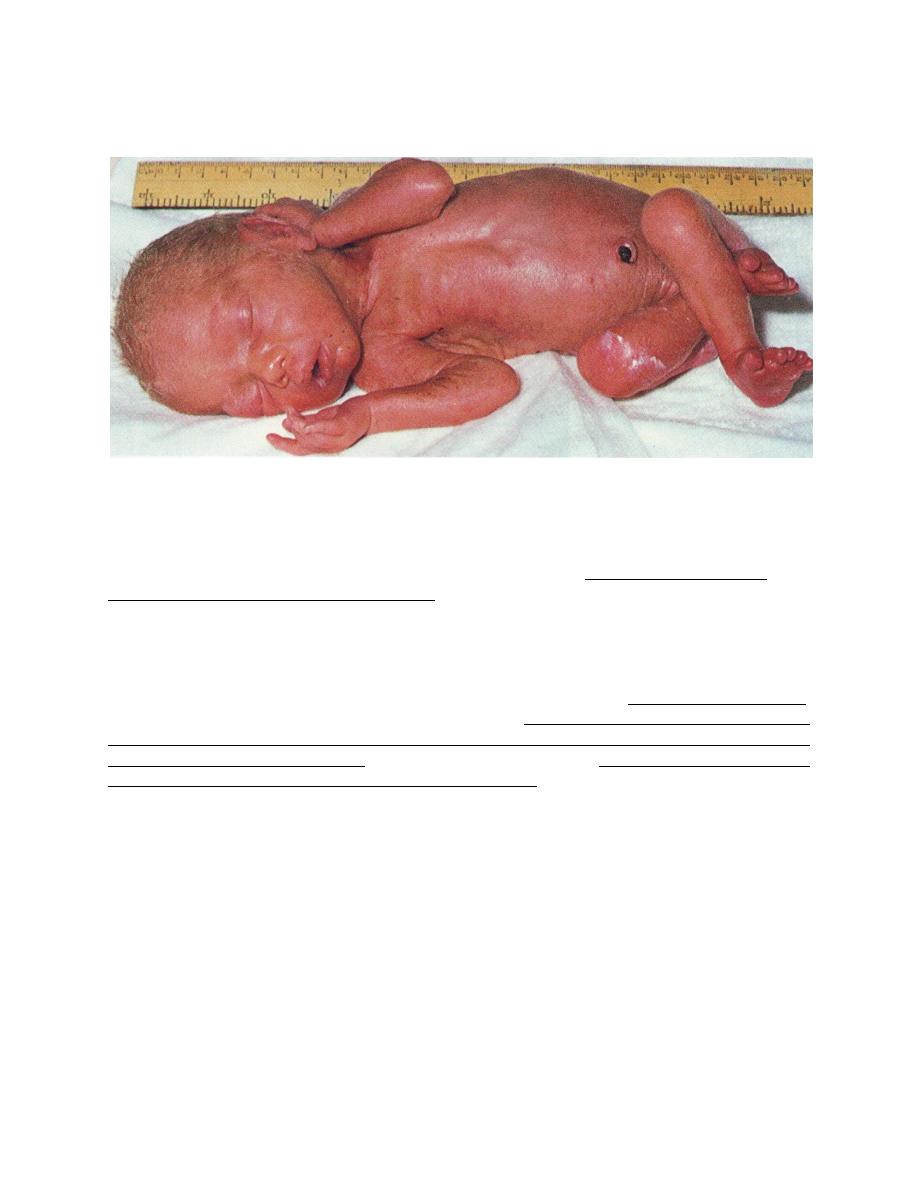
Prematurity
Premature: is live born infants delivered before 37 wk from the 1
st
day of the last menstrual
period.
Low birth weight (LBW): (birth weight <2500g) is due to either prematurity, poor intrauterine
growth (IUGR, SGA), or both. Prematurity and IUGR are associated with increased neonatal
morbidity and mortality than gestational age-matched infants.
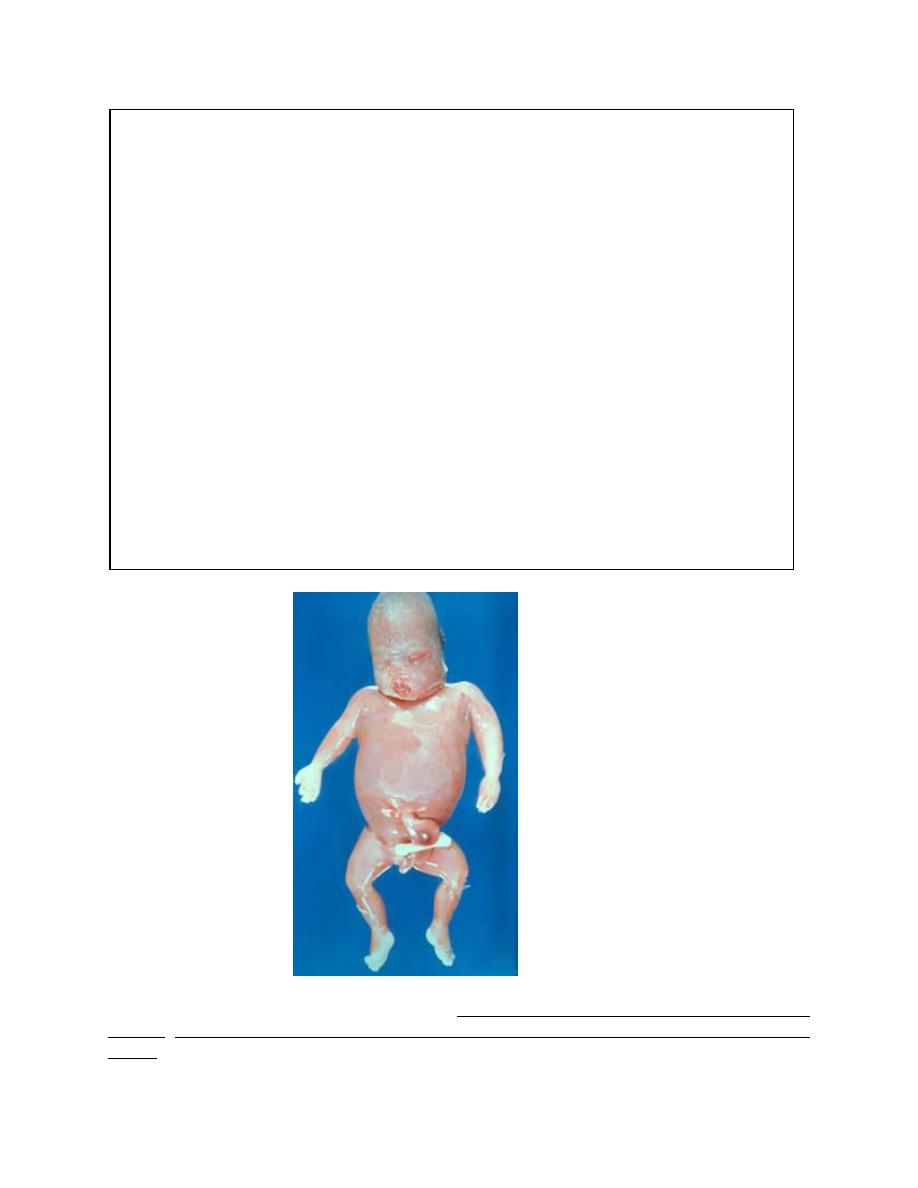
Very Low birth weight (VLBW): infants weigh <1,500g, and are predominantly premature, their
survival is directly related to birth weight. VLBW neonates have a higher incidence of re-
hospitalization during the 1
st
yr of life for sequelae of prematurity, including; infections, neurologic
complications, and psychosocial disorders.
Factors Related to Premature Birth and Low Birth weight:
A strong positive correlation exists between both preterm birth, IUGR and low socioeconomic status.
Families of low socio-economic status have higher rates of maternal under nutrition, anemia, illness,
inadequate prenatal care, drug misuse, obstetric complications, and maternal histories of abortions,
stillbirths, premature or LBW infants. Other associated factors include single-parent families, teenage
pregnancies, short inter-pregnancy interval, maternal smoking.
Premature birth of infants whose weight is appropriate for their preterm gestational age is associated
with medical conditions; inability of the uterus to retain the fetus, premature rupture of the
membranes, premature separation of the placenta.
The etiology of preterm birth is multifactorial and involves a complex interaction between fetal,
placenta, uterine, and maternal factors.
2
Identifiable Causes of Preterm Birth
1-FETAL
Fetal distress
Multiple gestation
Erythroblastosis
Nonimmune hydrops
2-PLACENTAL
Placental dysfunction
Placenta previa
Abruplio placentae
3-UTERINE
Bicornuate uterus
Incompetent cervix (premature dilatation)
4-MATERNAL
Preeclampsia
Chronic medical illness (e.g., cyanotic heart disease, renal disease)
Infection (e.g., Listens monocytogenes, group B streptococcus, urinary tract infection,
bacterial vaginosis, chorioamnionitis)
Drug abuse (e.g., cocaine)
5-OTHER
Premature rupture of membranes
Polyhydramnios
Iatrogenic, Trauma
Hydrops fetalis
IUGR is associated with medical conditions that interfere with the circulation and efficiency of the
placenta, with the development or growth of the fetus, or with the general health and nutrition of the
mother.
3
Factors Often Associated with Intrauterine Growth Restriction
1-Fetal
Chromosomal disorders(e.g. autosomal trisomies)
Chronic fetal infections (e.g. cytomegalic inclusion disease, congenital rubella, syphilis)
Congenital anomalies
Irradiation
Multiple gestation
Pancreatic hypoplasia
Insulin deficiency and Insulin-like growth factor type I deficiency
2-PLACENTAL
Decreased placental weight or cellularity, or both
Decrease in surface area
Villous placentitis (bacterial, viral, parasitic)
Infarction
Tumor (chorioangioma, hydatidiform mole)
Placental separation
Twin transfusion syndrome
3-MATERNAL
Toxemia
Hypertension or renal disease, or both
Hypoxemia (high altitude, cyanotic cardiac or pulmonary disease)
Malnutrition or chronic illness
Sickle cell anemia
Drugs (narcotics, alcohol, cigarettes, cocaine, antimetabolites)
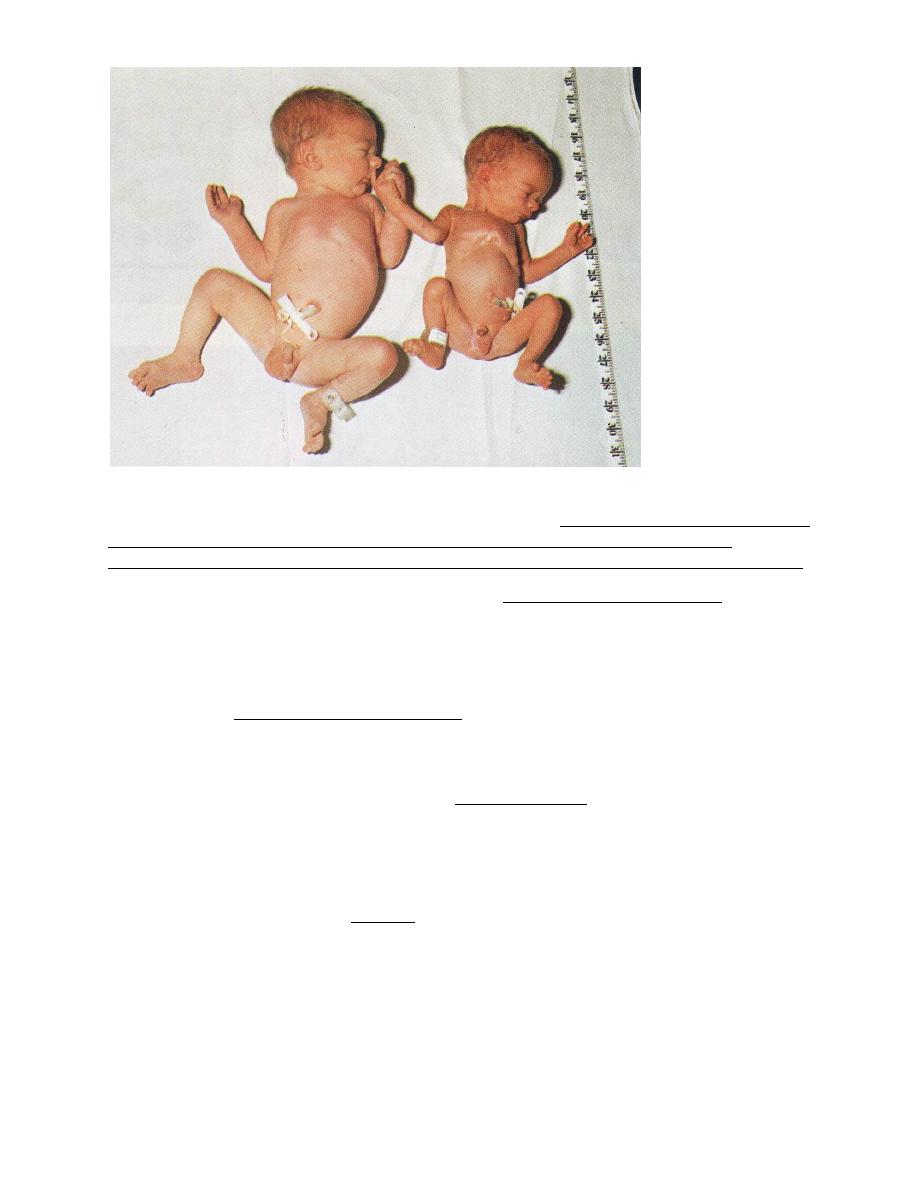
4
Twin transfusion syndrome
Spectrum of disease in low-birth weight premature infants; prematurity increases the severity
but reduces the distinctiveness of the clinical manifestations of most neonatal diseases.
Among VLBW infants (predominantly premature), morbidity is inversely related to birth weight.
Problems of LBW premature infants; These include; Respiratory distress syndrome, pulmonary
hemorrhage, aspiration syndrome, pneumothorax, apnea, hypoglycemia, hypocalcemia,
hyperbilirubinemia, anemia, hypothermia, feeding problems, bacterial sepsis, necrotizing
enterocolitis and DIC.
Causes of death in LBW premature infants; Morbidity is inversely related to birth weight.
These include; respiratory distress syndrome, intraventricular hemorrhage (IVH), sepsis,
asphyxia, birth injuries, and congenital malformations.
Problems associated with IUGR LBW infants; Perinatal asphyxia (↓placental perfusion during
labor, chronic fetal hypoxia–acidosis; meconium aspiration syndrome), hypoglycemia,
polycythemia-hyperviscosity (fetal hypoxia, erythropoietin production), hypothermia, pulmonary
hemorrhage, meconium aspiration, necrotizing enterocolitis and illnesses related to congenital
anomalies and syndromes.
Causes of death in term infants; asphyxia, infection, anomalies and aspiration pneumonia.
5
Complications of prematurity as classified by systems;
Respiratory; Respiratory distress syndrome, Broncho-pulrnonary dysplasia, Pneumothorax,
pneumomediastinum, Pulmonary hypoplasia, Pulmonary hemorrhage and apnea.
Cardiovascular; Patent ductus arteriosus, Hypotension, Hypertension, Bradycardia
Hematologic; Anemia (early or late onset), Disseminated intravascular coagulopathy, Vitamin K
deficiency.
Gastrointestinal;
Poor
function
and
motility,
Necrotizing
enterotolitis,
Hyperbilirubinemia(direct, indirect), Spontaneous gastrointestinal isolated perforation.
Metabolic-Endocrine; Hypocalcemia, Hypoglycemia, Hyperglycemia, Late metabolic acidosis,
Hypothermia.
Central Nervous System; lntraventricular hemorrhage, Periventricular leukomalacia, Seizures,
Retinopathy of prematurity, Deafness, Hypotonia, and Kernicterus.
Renal; Hyponatremia, Hypernatremia, Hyperkalemia, Renal tubular acidosis, Renal glycosuria,
Edema,
Infections; congenital, perinatal, nosocomial (bacterial, viral, fungal, protozoal)
Apnea; Apnea is defined as the cessation of airflow. Apnea is pathologic if cessation of
breathing is for longer than 20 seconds or for any duration if accompanied by cyanosis and
bradycardia.
Periodic breathing (Cheyne-Stokes rhythm) must be distinguished from prolonged apneic pauses,
because the latter may be associated with serious illnesses.
Causes of pathologic apnea include;
1
Central nervous system depression,
2
Respiratory infections
and obstructions,
3
Infections like sepsis or meningitis,
4
Metabolic causes (↓ Glucose, ↓ calcium,
↓/↑ sodium, ↑ ammonia, ↑ organic acids, ↑ ambient temperature, hypothermia),
5
Cardiovascular
like hypotension, and
6
Immaturity of respiratory center.
Cyanosis at birth;
1. Central or peripheral nervous system related hypoventilation; Intracranial hypertension,
hemorrhage, oversedation, diaphragm palsy, seizures.
2. Respiratory causes;
1
Airway; Choanal atresia/stenosis, laryngeal/tracheal stenosis, vascular compression.
2
Lung; Respiratory distress syndrome, Transient tachypnea, Meconium aspiration, Pneumonia
(sepsis), Pneumothorax, Congenital diaphragmatic hernia.
3. Cardiac (Rt Lt shunt
)
1
Abnormal connections (normal or increased pulmonary blood flow): Transposition of great
vessels, Anomalous pulmonary venous return, Truncus arteriosus, Hypoplastic left heart
syndrome, Single ventricle or tricuspid atresia.
2
Obstructed pulmonary blood flow: Pulmonary atresia with intact ventricular septum,
Tetralogy of Fallot, Critical pulmonic stenosis, Tricuspid atresia, persistent pulmonary
hypertension.
4. Methemoglobinemia
5. Others: Hypoglycemia, polycythemia, blood loss.
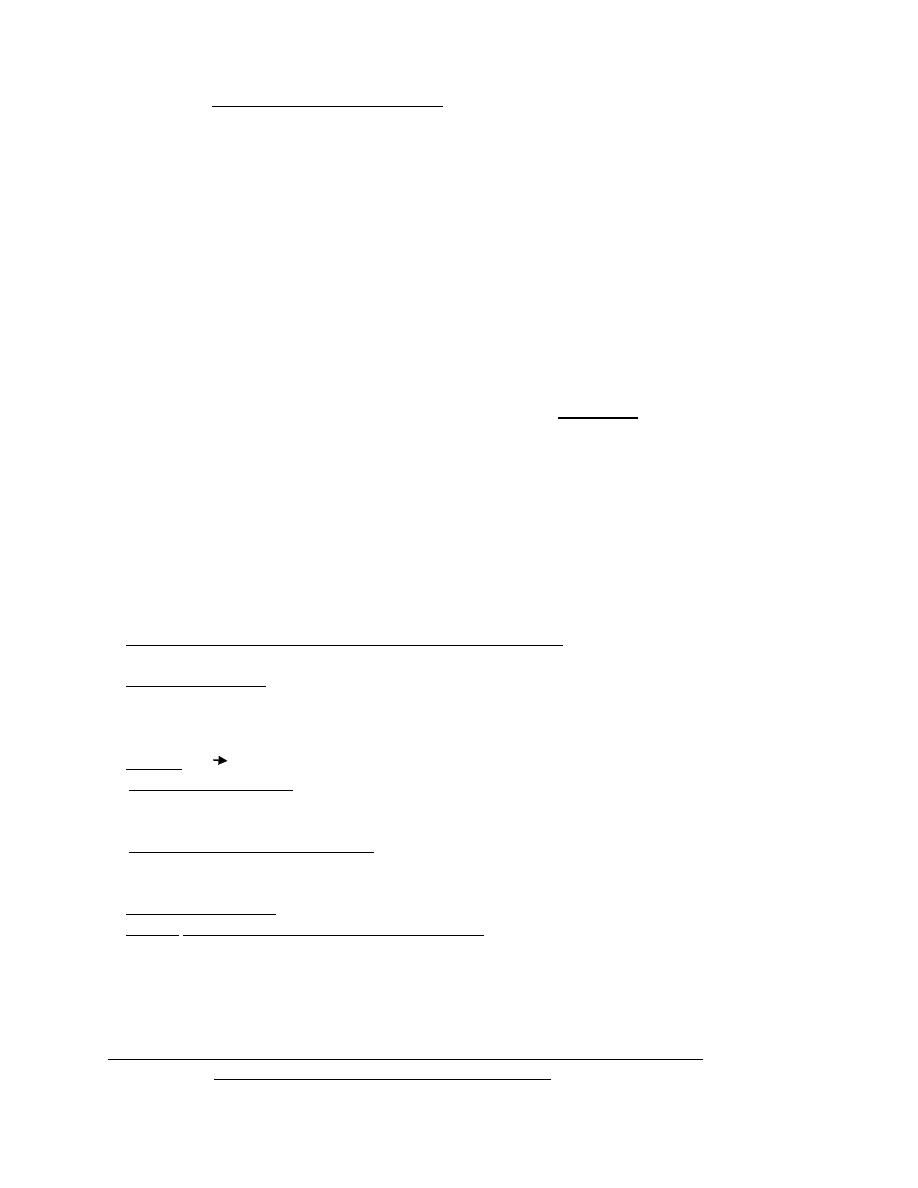
Retinopathy of prematurity (ROP):
This retinal vasculopathy occurs almost exclusively in preterm infants; it is retinal vaso-
proliferation, scarring, and potentially blinding retinal detachment.
Etiology; Prematurity is the risk factor. Hyperoxia is a major factor, but other problems, such as
respiratory distress, apnea, bradycardia, infection, hypoxia are contributory factors.
Generally, the lower the birth weight and the sicker the infant, the greater the risk for ROP.
6
Use of supplemental vitamin E as antioxidant has no proven efficacy. No safe level of oxygen
has yet been determined but each infant must be treated with whatever is necessary to sustain life
and neurologic function.
Ophthalmologic examination for ROP of infants (less than 1,500 g at birth and those born before
28 wk) at risk is recommended and performed at 4-6 wk of life.
Treatment; in selected cases is cryotherapy or laser photocoagulation.
Retinopathy of prematurity; Retinal vessels are dilated and tortuous
Nursery care of premature; At birth, measures to clear the airway, initiate breathing, care for the
umbilical cord and eyes, and administer vitamin K are the same as for normal weight and
maturity infants. Additional considerations;
1- Thermal Control. the insulating layer of subcutaneous fat is thinner in low-birth weight
infants than term infants. The survival rate of LBW and sick infants is higher when they are
cared for near their neutral thermal environment. Incubators or radiant warmers can be used to
maintain body temperature.
The optimal environmental temperature for minimal heat loss and minimal oxygen consumption
for an unclothed infant is one that maintains the infant's core temperature at 36.5-37.0
o
C. It
depends on an infant's size and maturity; the smaller and more immature the infant, the higher
the environmental temperature required.
2- Administering oxygen. to reduce the risk of injury from hypoxia and circulatory insufficiency
must be balanced against the risk of hyperoxia to the eyes (retinopathy of prematurity and
bronchopulmonary dysplasia) and oxygen injury to the lungs. Oxygen is administered via a head
hood, nasal cannula, continuous positive airway pressure apparatus, or endotracheal tube. The
concentration of inspired oxygen is adjusted in accordance with the oxygen tension of arterial
blood (PaO
2
) or noninvasive methods such as continuous pulse oximetry.
3- Prevention of Infection. Premature infants have an increased susceptibility to infection.
Prevention includes; hand-washing, avoiding crowding, meticulous skin care, and surveillance of
nosocomial infection. Routine immunizations should be given on the regular schedule at
standard doses.

7
Post-mature infants; are infants whose gestation exceeds the normal 280 days by 7 or more
days. The cause is unknown.
Post-term infants; are those born after 42 wk of gestation, as calculated from the 1
st
day of the
last menstrual period, regardless of birth weight.
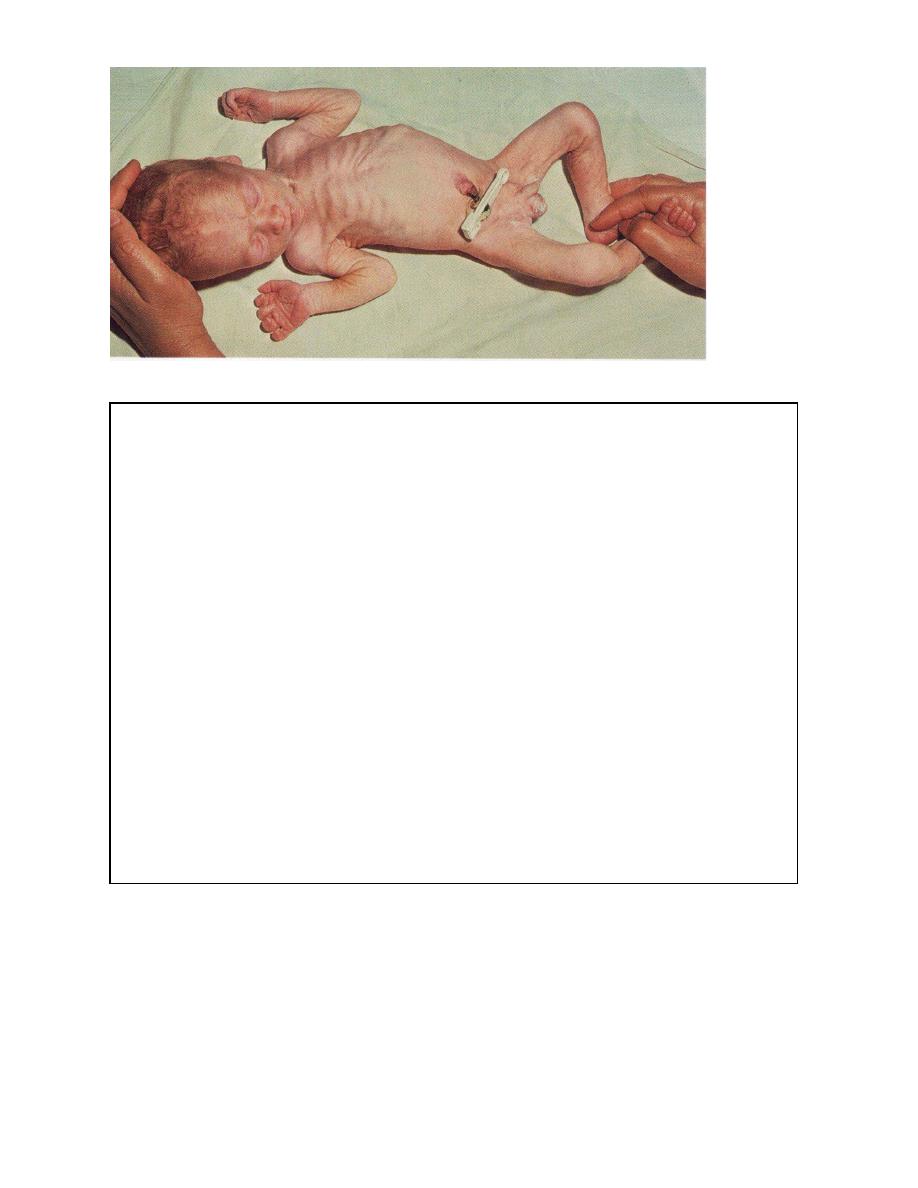
Post-term, post-mature infants often have increased birth weight and are characterized by the
absence of lanugo, vernix caseosa, long abundant scalp hair, white desquamating skin, and
increased alertness.
Post-term infant in association with presumed placental insufficiency may have; Desquamation,
long nails, abundant hair, pale skin, alert faces, and loose skin, especially around the thighs and
buttocks, give them the appearance of having recently lost weight; meconium-staining (nails,
skin, and vernix, umbilical cord, and placental membranes) may also be noted. When delivery is
delayed 3 wk or more beyond term, mortality is significantly increased.
Management; Careful obstetric monitoring, including non-stress testing, biophysical profile
usually provides a rational basis for choosing the course of delivery.
Large for gestational age; Neonatal mortality rates decrease with increasing birth weight until
approximately 4,000 g, after which mortality increases.
8
These oversized infants are usually born at term, maternal diabetes and obesity are predisposing
factors.
Infants, who are very large, regardless of their gestational age, have a higher incidence of birth
injuries such as cervical and brachial plexus injuries, phrenic nerve damage with paralysis of
diaphragm, fractured clavicles, cephalohematomas, and subdural hematoma. The incidence of
congenital anomalies, particularly congenital heart disease, intellectual and developmental
retardation is statistically more common in high-birthweight term and preterm infants.
Nasal cannula