معالجة / رابع اسنان
14/11/2016معالجة / رابع اسنان
14/11/2016
Dental caries
Dental caries can be defined as demineralization of the tooth surface caused by bacteria. The term dental caries is used to describe the results of a localized chemical dissolution of the tooth surface caused by metabolic events taking place in the biofilm (dental plaque) covering the affected area. The destruction can affect enamel, dentin and cementum.
Dental caries lesions may develop at any tooth site in the oral cavity where a biofilm (Dental plaque) develops and remains for a period of time.
The dissolution (demineralization) when pH drops below a certain level in the biofilm (Dental plaque) and the redeposition (remineralization) of minerals when pH goes up take place in the enamel surface at the interface between the biofilm and the tooth surface. These processes occur numerous times during a day and can be modified extensively.
Dental plaque
Dental plaque is an adherent deposit of bacteria and their products, which forms on all tooth surfaces and cause caries.
Dental plaque is (biofilm) community of microorganisms attached to a surface. The organisms are organized into a three-dimensional structure enclosed in a matrix of extracellular material.
Dental plaque formation can be described as:
1- Formation of pellicle: an acellular, film, derived from saliva, which forms on a tooth surface.
2- Within 4 hours, single bacterial cells colonize the pellicle. A large proportion of these are streptococci There are also Acintomyces species and Gram-negative bacteria.
Only about 2% of the initial streptococci are mutans streptococci.
3- next 24 hours formation of distinct microcolonies.
4- In 14 days the Streptococcus-dominated plaque changes to a plaque dominated by Actinomyces. Thus the population shifts; this is called microbial succession.
5- In 2weeks the plaque is mature but there are considerable site-to-site variations in its composition.
Factor that influences the metabolic processes:
1-the composition and thickness of the biofilm(Dental plaque).
2-the salivary secretion rate and composition .
3-the diet .
4-fluoride ion concentration in the oral fluids .
Enamel and dentine structure
Enamel consists of crystals of hydroxyapatite packed tightly together in an orderly arrangement (the enamel prisms). enamel has a glass-like appearance and it is translucent, allowing the colour of the dentine to shine through it. Even though crystal packing is very tight, each crystal is actually separated from its neighbours by tiny intercrystalline spaces or pores. These spaces are filled with water and organic material. When enamel is exposed to acids produced in the microbial biofilm, mineral is removed from the surface of the crystal which shrinks in size. Thus, the intercrystalline spaces enlarge and the tissue becomes more porous. This increase in porosity can be seen clinically as a white spot.
Dentine is a vital tissue permeated by tubules containing the cell processes of the odontoblasts. This vital tissue defends itself from any assault, such as caries, by tubular sclerosis. This is the deposition of mineral along and within the dentinal tubules resulting in their gradual occlusion. In addition, the odontoblasts form tertiary dentine at the pulp–dentine border in response to the stimulus.
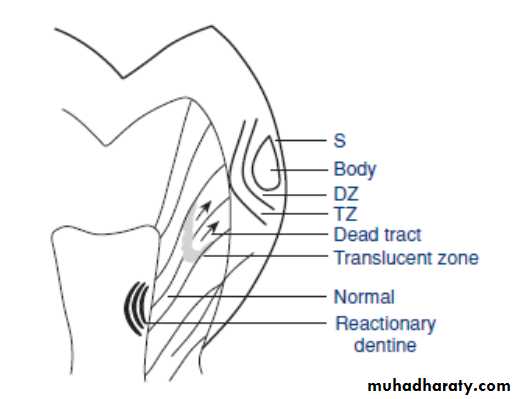
histological changes in enamel before cavitation (white spot dental caries lesion).
1-Surface zone.
2-body of lesion.
3-dark zone.
4-translucent zone.
The shape of dental caries lesion in enamel
1- smooth surface: the lesion is classically triangular in shape. It follows the direction of the enamel prisms. The shape of the lesion and the activity of the lesion entirely reflect the specific environmental conditions of the overlying biofilm.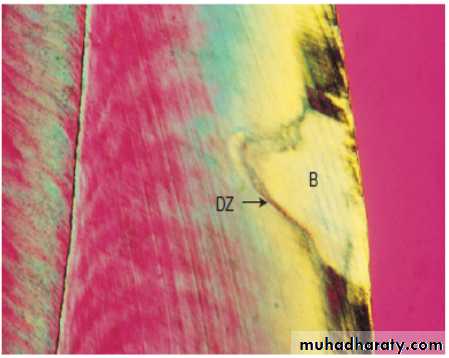
2-Occlusally: purely because of the sloping fissure walls and the direction of the enamel prisms, the lesion assumes an undermining character. This explains why in the more advanced lesion, where there appears to be a small hole in the tooth, something apparently so small on the surface can be so large when entered with a burr . Once a cavity forms on this surface it is narrower at the top than at the base.
histological changes in dentine
The dentine has been reacting to the carious process in the biofilm(dental plaque)long before a cavity forms. Dentine is a vital tissue, permeated by the tubules containing the cell processes of the odontoblasts, and it defends itself by the tubular sclerosis within the dentine and the formation of tertiary dentine (also called reactionary dentine or reparative dentine) at the pulp-dentine border.Tubular sclerosis is the deposition of mineral within the dentinal tubules and it requires the presence of a vital odontoblast. It can be seen in the light microscope where a traverse through the centre of the enamel lesion crosses the enamel–dentine junction. The enamel demineralization has increased the enamel porosity and permeability and this dentine reaction corresponds to the most porous part of the enamel lesion, which in turn corresponds to the activity of the biofilm .
When contact between the enamel lesion and the enamel–dentine junction is established, the first sign of dentine demineralization can be seen along the junction as a brownish discolouration within the contact area of the enamel lesion and the junction. Demineralization of outer dentine is now surrounded by sclerotic reactions corresponding to the less advanced peripheral parts of the enamel lesion.
Dentine changes in cavitated lesion
1-the zone of destruction: following exposure of dentine to the mass of bacteria in the cavity, the most superficial part of the dentine is decomposed by the action of acids and proteolytic microorganisms.2-the zone of penetration: tubular invasion of bacteria is frequently seen beneath the first zone.
3- Area of demineralized: dentine which does not yet contain bacteria .
4- Dead tracts : the odontoblast processes have been destroyed without producing tubular sclerosis.
5-liquefaction foci: tubules are invaded by bacteria and groups of tubules coalesce.
6-transverse clefts: destruction may also advance along the incremental lines of growth which are at right angles to the tubules.
The defence reactions of tubular sclerosis and tertiary dentine formation continue as a response to these destructive processes. Both processes reduce the permeability of the dentine, although tertiary dentine is less well mineralized than primary or secondary dentine and contains irregular dentinal tubules.
Caries lesions can be classified according to their anatomical site.
1-pits and fissures.2-smooth surfaces.
lesions may start on enamel (enamel caries) or on the exposed root cementum and dentin (root caries).
Caries lesions may also be classified to:
1-Primary caries
Which is caries on natural, intact tooth surfaces.
2-recurrent or secondary caries
Which define as a lesion developing at a tooth surface adjacent to a filling , its etiology is similar to that of primary caries.
3-Residual caries
Which is demineralized tissue that has been left behind before a filling is placed.
Another Classification of dental caries
1- cavitated lesion .
2- non-cavitated.
classification according to their activity
1-active caries lesion.
A lesion considered to be progressing .
2-arrested caries lesions or inactive caries lesions.
lesions that may have formed years previously and then stopped further progression.
the clinical distinction between active and inactive (arrested) lesions is sometimes difficult.
white-spot, early, initial or incipient caries
Definition of incipient is ‘beginning’; an initial stage. In other words, an initial lesion appears as a white, opaque change (a white spot). carious lesion on enamel that can be detected with the naked eye.Root-surface caries
Active lesions were described as soft or leathery and were usually found at plaque-retention sites next to the gingival margin or along the cement-enamel junction. Inactive lesions were typically located at some distance from the gingival margin, felt hard on gentle probing and often presented with a shiny appearance.
Rampant caries
The name given to multiple active carious lesions occurring in the same patient. This frequently involves surfaces of teeth that do not usually experience dental caries. These patients with rampant caries can be classified :
bottle or nursing caries.
early childhood caries.
radiation caries or drug-induced caries.
Hidden caries
A term used to describe lesions in dentin that are missed on a visual examination but are largeenough and demineralized enough to be detected radio graphically.