1
HYDATID DISEASE
L8
Introduction and pathology
ⱴ Commonly called dog tapeworm, hydatid disease is caused by Ecchinococcus
granulosus. While it is common in the tropics, in the UK, the occasional patient may
come from a rural sheep farming community.
ⱴ The dog is the definitive host and is the commonest source of infection transmitted
to the intermediate hosts – humans, sheep and cattle. In the dog, the adult worm
reaches the small intestine, and the eggs are passed in the faeces.
ⱴ These eggs are highly resistant to extremes of temperature and may survive for long
periods. In the dog’s intestine, the cyst wall is digested, allowing the protoscolices to
develop into adult worms.
ⱴ Close contact with the infected dog causes contamination by the oral route, with the
ovum thus gaining entry into the human gastrointestinal, tract.
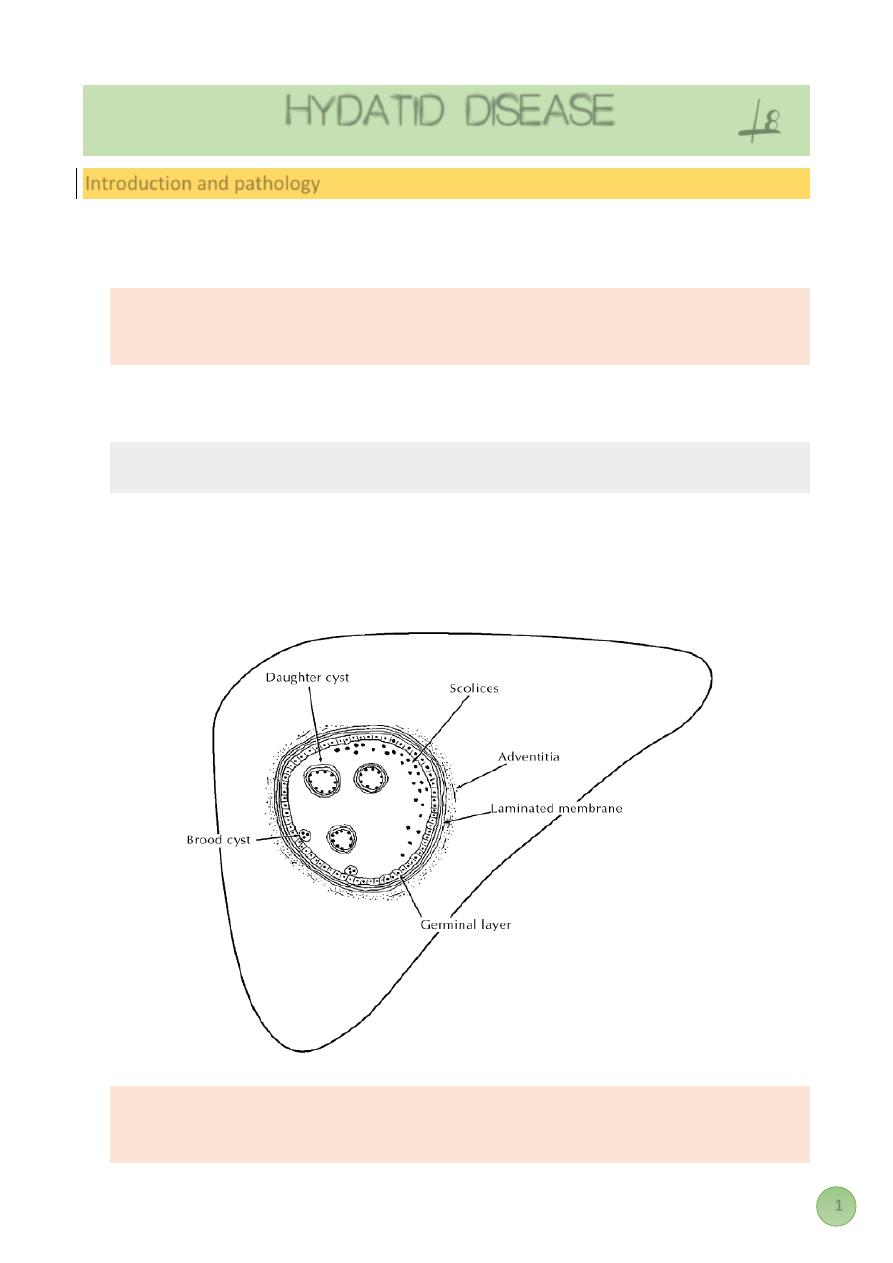
ⱴ The cyst is characterised by three layers, an outer pericyst derived from compressed
host organ tissues, an intermediate hyaline ectocyst which is non-infective and an
inner endocyst that is the germinal membrane and contains viable parasites which
can separate forming daughter cysts.
ⱴ A variant of the disease occurs in colder climates caused by Echinococcus
multilocularis, in which the cyst spreads from the outset by actual invasion rather
than expansion.
2
Classification
In 2003, the WHO Informal Working Group on Echinococcosis proposed a standardised
ultrasound classification based on the status of activity of the cyst. This is universally
accepted, particularly because it helps to decide on the appropriate management. Three
groups have been recognized:
Group 1: Active group – cysts larger than 2 cm and often fertile.
Group 2: Transition group – cysts starting to degenerate and entering a transitional
stage because of host resistance or treatment, but may contain viable scolices.
Group 3: Inactive group – degenerated, partially or totally calcified cysts; unlikely to
contain viable scolices.
Clinical features
As the parasite can colonise virtually every organ in the body, the condition can be protean
in its presentation. When a sheep farmer, who is otherwise healthy, complains of a gradually
enlarging painful mass in the right upper quadrant with the physical findings of a liver
swelling, a hydatid liver cyst should be considered.
The liver is the organ most often affected. The lung is the next most common. The parasite
can affect any organ or several organs in the same patient.
The disease may be asymptomatic and discovered incidentally at post mortem or when an
ultrasound or CT scan is done for some other condition. Symptomatic disease presents with
a swelling causing pressure effects. Thus, a hepatic lesion causes dull pain from stretching
of the liver capsule, and a pulmonary lesion, if large enough, causes dyspnoea.
Daughter cysts may communicate with the biliary tree causing obstructive jaundice and all
the usual clinical features associated with it in addition to symptoms attributable to a
parasitic infestation
Features of raised intracranial pressure or unexplained headaches in a patient from a sheep-
rearing community should raise the suspicion of a cerebral hydatid cyst.
The patient may present as an emergency with severe abdominal pain following minor
trauma when the CT scan may be diagnostic. Rarely, a patient may present as an emergency
with features of anaphylactic shock without any obvious cause.
Such a patient may subsequently cough up white material that contains scolices that have
travelled into the tracheobronchial tree from rupture of a hepatic hydatid on the
diaphragmatic surface of the liver.
Diagnosis
There should be a high index of suspicion. Investigations show a raised eosinophil count;
serological tests such as ELISA and immunoelectrophoresis point towards the diagnosis.
3
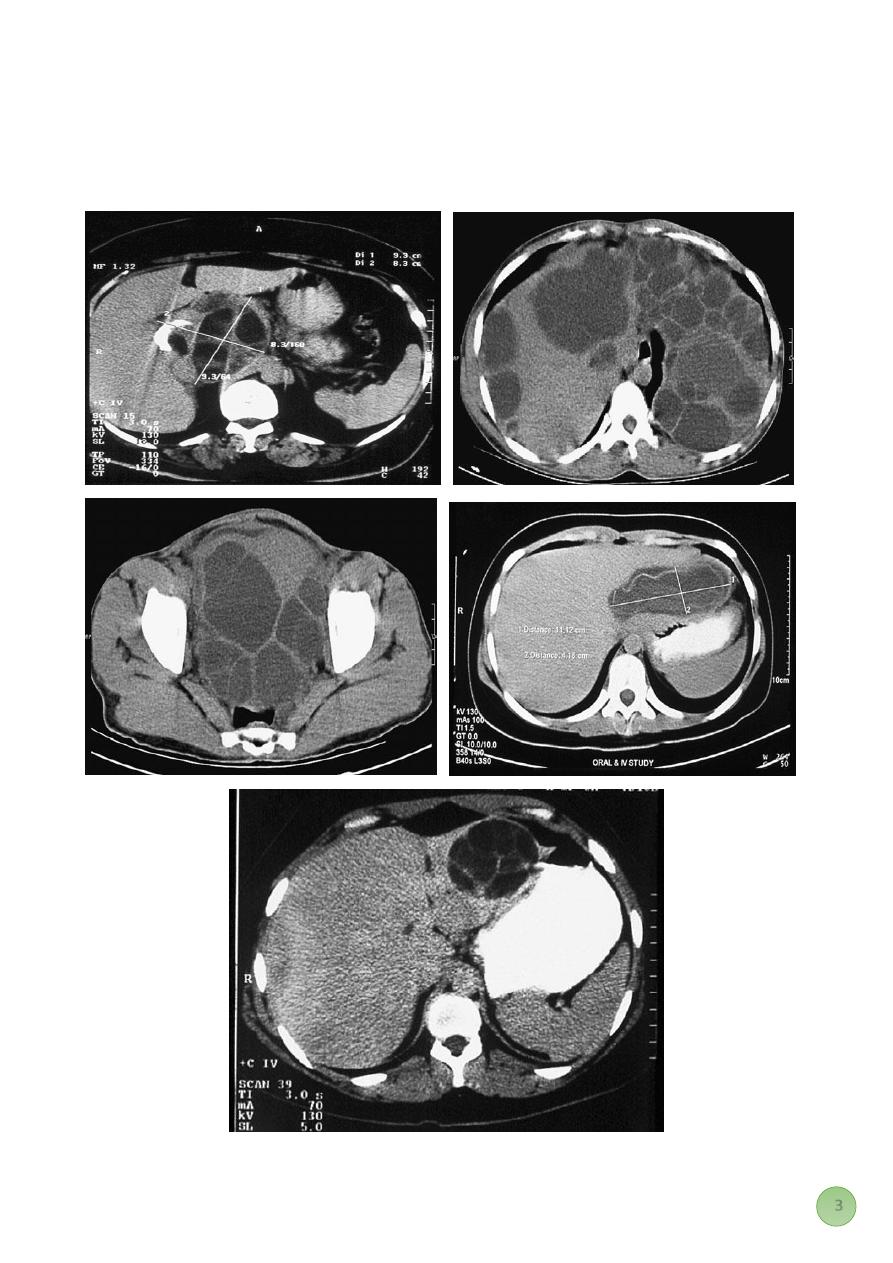
Ultrasound and CT scan are the investigations of choice. The CT scan shows a smooth space-
occupying lesion with several septa.
An ultrasound of the biliary tract may show abnormality in the gall bladder and bile ducts.
Hydatid infestation of the biliary system should then be suspected.
4
Treatment
Here, the treatment of hepatic hydatid is outlined as the liver is most commonly affected,
but the same general principles apply whichever organ is involved.
Medical treatment
Whether the patient is treated only medically or in combination with surgery will depend
upon the clinical group (which gives an idea as to its activity), the number of cysts and their
anatomical position.srart by albendazole 200mg single daily for three months .other
mebendazol or praziquantel has also been used.
Surgical treatment by minimal access therapy is best summarised by the mnemonic PAIR –
puncture, aspiration, injection and reaspiration. This is done after adequate drug treatment
with albendazole or praziquantel.
Surical treatment
Radical total or partial pericystectomy with omentoplasty or hepatic segmentectomy
(especially if the lesion is in a peripheral part of the liver) are some of the surgical options.
During the operation, scolicidal agents are used, such as hypertonic saline (15–20%), ethanol
(75–95%) or 1% povidone iodine, although some use a 10% solution,This may cause
sclerosing cholangitis if biliary tree are in communication with the cyst wall.
A laparoscopic approach to these procedures is being tried.
Regarding hydatid disease, which one of the following is incorrect?
A. The human is an end host, which breaks the development cycle of the parasite .
B. Initial infection occurs through the alimentary tract and is asymptomatic.
C. The natural history of a hydatid cyst in the human is one of slow progressive growth.
D. Rupture of a hydatid cyst is a common event.
E. Most symptoms are related to pressure effects on the liver and surrounding organs.
Which one of the following statements regarding the management of hydatid cysts is false?
A. Extremely small cysts may be managed conservatively provided they are followed up
to monitor growth.
B. Medical management is successful in the majority of cases.
C. Medical therapy is usually used to supplement surgical intervention.
D. The most common surgical technique is that of evacuation of the content and de-
roofing of the cyst and the placement of an omental patch in the cavity.
Mubark A. Wilkins