Postoperative care
INTRODUCTIONThe aim of postoperative care is to provide the patient with as quick, painless and safe a recovery from surgery as possible.
GENERAL MANAGEMENT
The immediate postoperative period
In the immediate postoperative period the patient is nursed in a recovery area using one-to-one nursing and continuous monitoring.The role of the recovery nurse is to ensure that the patient is protecting their airway, breathing freely and perfusing adequately (airway, breathing and circulation).
The recovery nurse should also monitor the patient’s pain as the anaesthetic wears off and ensure that there are no early complications developing, such as bleeding from the wound or loss of distal circulation and/or sensation. Blood pressure, pulse and oxygen saturation are therefore monitored regularly and the results charted. Trends seen on these charts reassure the recovery nurse that the patient is recovering well or warn that a complication is developing
Patient recovery
Once patients are fully conscious and comfortable and their vital functions are stable they are transferred to the general ward; however, patients who are at high risk may be transferred to a high-dependency or intensive care unit. While on the ward patients should be visited at least morning and evening by medical staff to ensure that there is steady progress. All staff on these rounds must wash their hands between every patient
SubjectiveAsk the patient how they are. Specifically, ask about pain, nausea and mobility. Anxiety, disorientation or a change in behaviour are often the first signs that complications are setting in.
ObjectiveCheck the patient’s charts for temperature, pulse and respiration (TPR), fluid balance and any special observations recorded by thenurses (such as colour of graft). The patient’s pressure areas should be checked but, if the wound is to be inspected. If possible, wounds should be left undisturbed for 48 hours after surgery to prevent contamination . Specific examinations also need to be recorded, such as bowel sounds after abdominal surgery or distal neurovascular status after orthopaedic procedures
PAIN CONTROL
Pain control is important not only to avoid the distress it causes. In addition, uncontrolled pain delays recovery and increases postoperative complications. Pain from chest and upper abdominal incisions inhibits both adequate respiratory effort and the clearance of secretions. Control of pain reduces the incidence of postoperative chest infections.
Pain after abdominal incisions is a factor in postoperative ileus, and the reduction of this complication in laparoscopic surgery is probably in part related to a reduction in abdominal wall wound pain. Pain is also associated with many of the troublesome postoperative nausea and hypotensive episodes which prevent satisfactory discharge after day surgery
Oral analgesia
This is the mainstay for day surgery pain relief. A combination of a non-steroidal anti-inflammatory drug (NSAID) with a preparation of paracetamol and codeine proves satisfactory in most patients
Local anaesthetic infiltration
Local infiltration of bupivicaine into the wound provides excellent pain relief in the critical first 6 hours after surgery, and may be more effective if given at the start rather than the end of the operation
Intramuscular opiates
These are administered as bolus injections when required every 4–6 hours, and were for many years the mainstay of postoperative inpatient pain relief. The patient frequently requires intramuscular or intravenous pain relief in the recovery area, and this is followed by further injections as necessary
Intravenous opiates
This is the fastest method of bringing severe pain under control. A 2.5 mg dose of intravenous morphine is safe for an adult in severe pain, and can be repeated at 5-minute intervals, if necessary up to a total of 10 mg.
Patient-controlled analgesia (PCA)
This is a system of delivery of intravenous opiate, the dose ofwhich is controlled by the patient. The patient can administera bolus (usually of 1 mg in adults) by pressing the control button
Epidural analgesia
This is an extremely satisfactory method of ensuring a painfree early postoperative period after major abdominal or thoracic surgery, without the sedation of systemic opiates. An epidural catheter is placed in situ by the anaesthetist and analgesia is maintained by continuous infusion of local anaesthetic agents or opiates into the Overdosage can be responsible for hypotension, and failure of delivery from a blocked or misplaced catheter can result in severe breakthrough pain which is sometimes difficult to get under controlepidural space.
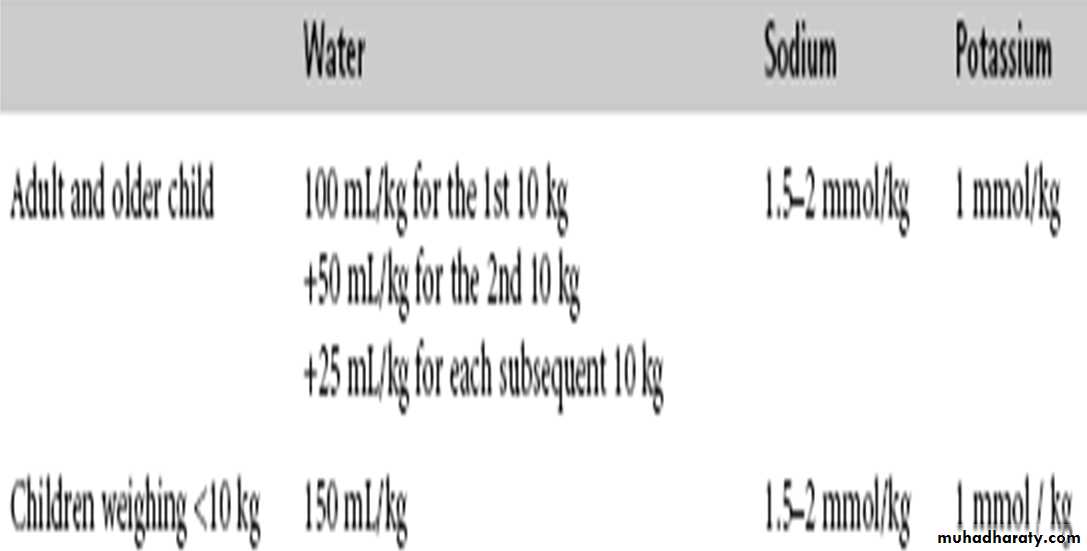
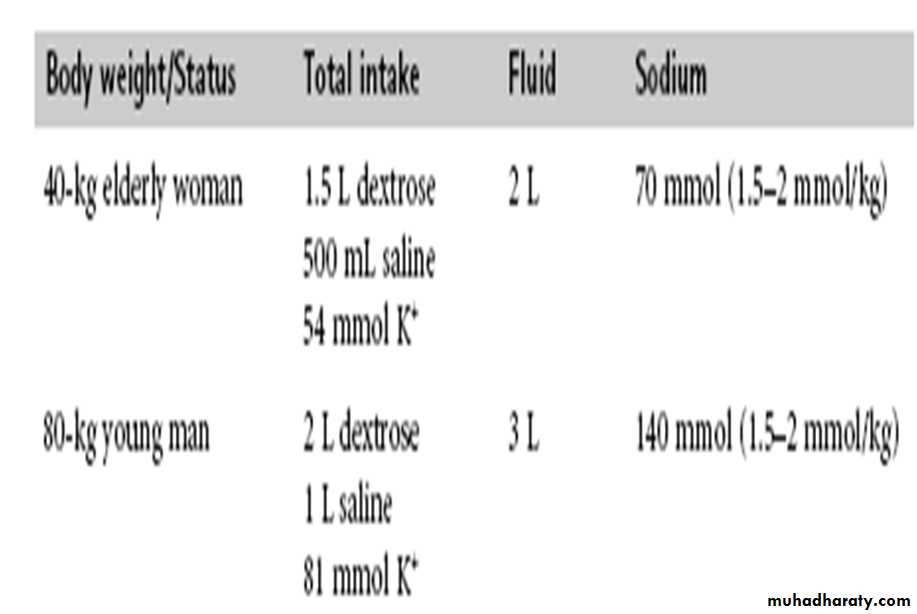
INTRAVENOUS FLUID REQUIREMENTS
Many postoperative patients, especially those who have had intra-abdominal surgery, will be unable to take oral fluids for several days. Maintenance fluid and electrolytes are given intravenously
POSTOPERATIVE COMPLICATIONS
COMPLICATIONS ASSOCIATED WITH THE INTRODUCTION OF INFUSIONAir embolismThis may occur when more than 15 ml of air is accidentally introduced during or after insertion of a venous catheter. The air enters the right atrium preventing adequate right heart filling and causing a drop in the blood pressure, a rise in the pulse rate and distension of the jugular venous pressure (JVP). It can be avoided by running fluids through the giving sets before connecting them to the patient. Patients should also be head-down
PhlebitisA needle or catheter inserted into a vein will eventually result in inflammation around the area (phlebitis
Finger necrosis
Arterial lines are usually inserted in patients who require continuous monitoring of pulse, blood pressure and arterial blood gases. They are usually inserted into the radial or femoral arteries. In some patients the blood supply to the hand arises predominantly from the radial artery, with little contribution from the ulnar artery. In these cases cannulation of the radial artery may disrupt the blood supply to the hand causing ischaemic necrosis of the finger
SPECIFIC POSTOPERATIVE COMPLICATIONS
Respiratory complications
Respiratory complications may be reduced by:• using adequate analgesia, including epidurals, and using analgesia that depresses respiration carefully (e.g. opioids);• administering oxygen using face masks or nasal prongs;• arranging regular physiotherapy in patients with asthma and chronic obstructive airway disease;• postponing surgery in patients with upper respiratory tract infections
1.Shortness of breath
The commonest cause of postoperative dyspnoea (shortness of breath) and rapid shallow breathing is alveolar collapse or atelectasis. The diagnosis is confirmed by clinical examination and radiography Abdominal surgical wounds may compromise respiratory function by splinting the diaphragm. Sudden onset of shortness of breath and tachypnoea (increased respiratory rate) may be caused by pulmonary embolism
A further cause of more gradual-onset postoperative shortness of breath is acute respiratory distress syndrome (ARDS). This may follow chest trauma, acute pancreatitis or sepsis, and results in poor oxygen transfer in the lungs even when the patient is given supplementary oxygen and is well perfused Any foreign bodies in the mouth, including dentures and vomitus, should be removed. The neck should be extended and the jaw pulled forward to allow the tongue to come forward, freeing the airway. The oral airway should be maintained and protected by an airway
2-CyanosisIn patients whose airway is clear but who develop cyanosis the problem may be in the lungs or in the circulation. Common problems in the lung may be acute bronchospasm as a result of an asthmatic attack or there may be a pneumothorax detected by loss of air entry into the upper chest. Circulatory problems include sudden blood loss causing a decreased venous return, myocardial infarction or a massive pulmonary embolism
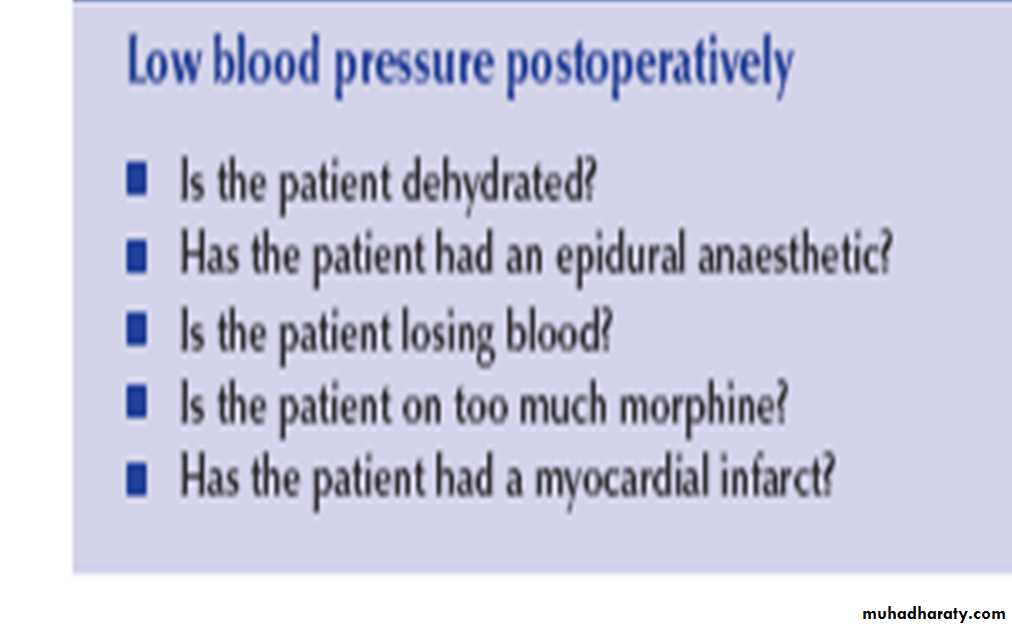
Cardiovascular complicationsHypotension
HypertensionHigh blood pressure may be dangerous in patients with ischaemic heart disease or cerebrovascular disease as it may precipitate infarction or stroke. Most causes of hypertension relate to inadequate pain relief or anxiety
Deep vein thrombosis:There are several risk factors for deep vein thrombosis (DVT
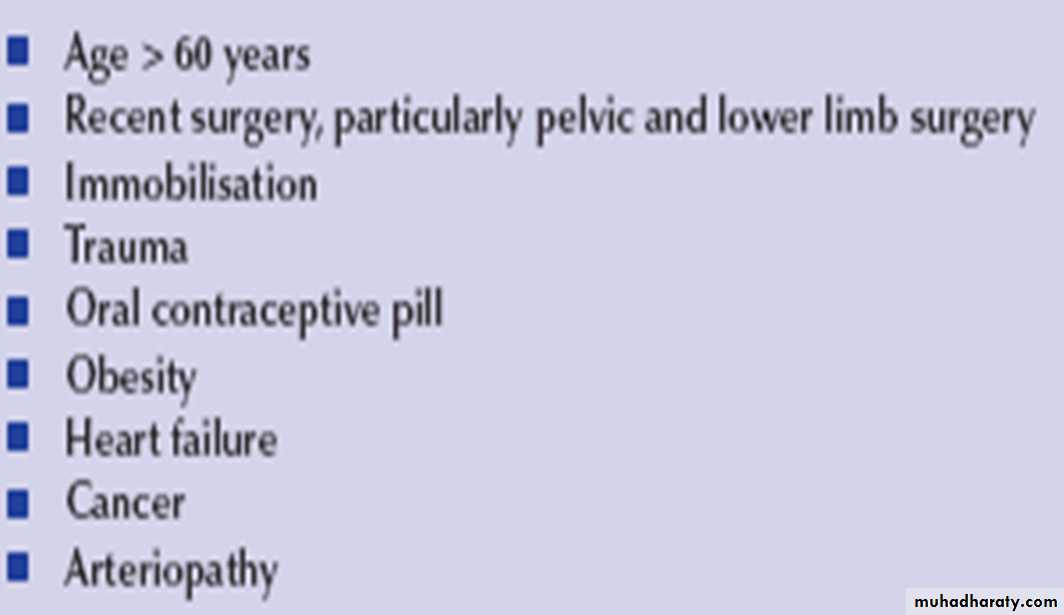
Most hospitals have a DVT prophylaxis protocol. This may include the use of stockings, calf pumps and pharmacological agents such as low molecular weight heparin
Gastrointestinal complications
Postoperative nausea and vomiting
This is a common problem It may have an adverse effect on the outcome of surgery including wound dehiscence and pulmonary aspiration if the patient’s airway is unprotected. Prolonged nausea and vomiting results in increased pain levels and a prolonged hospital stay
The following are predisposing factors for nausea and vomiting in postoperative patients:• poorly controlled pain;• use of opioids;• surgery on the gastrointestinal tract, orthopaedic surgery or ear, nose and throat (ENT) surgery;• female sex;• young adult;• history of preoperative vomiting;• history of motion sickness or migraine;• acute gastric dilatation
Urinary complications
Urine output (oliguria/anuria)
Oliguria may be defined as urine output less than (0.5 ml kg–1h–1). The commonest cause of oliguria postoperatively is reduced renal perfusion resulting from perioperative hypotension or inadequate fluid replacement. If untreated, acute renal failure may develop.
The serum levels of urea and creatinine should be measured daily until the patient is fully recovered. The fluid chart must be checked daily by the medical staff and the fluid balance calculations checked
Urinary retention
This is frequently seen in postoperative patients, particularly men who are bed-bound postoperatively. The inability to void after surgery is particularly common with pelvic and perineal operations or after procedures performed under spinal anaesthesia Retention may be confirmed by ultrasound and may require catheterisation. Catheterisation should be performed prophylactically when an operation is expected to last 3 hours or longer or when large volumes of fluid are administered
Urinary infection
This is the one of the most commonly acquired infections in the postoperative period. Patients who are immunocompromised or diabetic, or who have pre-existing urinary tract contamination, urinary retention or a history or presence of catheterisation
The diagnosis is confirmed by dipsticking the urine and sending samples for culture and sensitivity. Treatment involves adequate hydration and proper bladder drainage together with the use of relevant antibiotic