1
Fifth stage
Medicine
Lec 2
د.خالد نافع
2016-2017
Bleeding Disorders
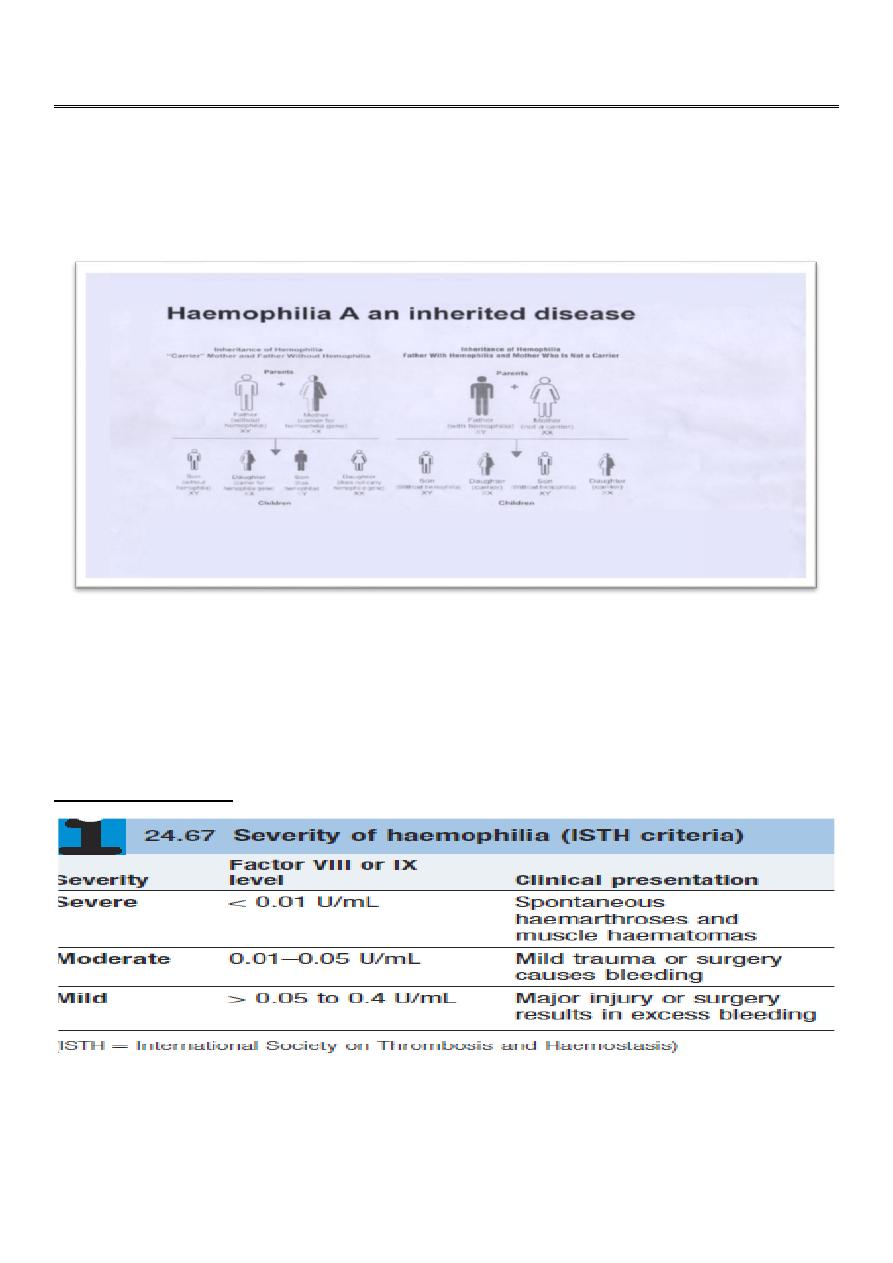
Haemophilia A ( ROYAL DISEASE )
Only men are affected .
Heamophillia A is the classic example of an X-linked recessive trait.
Hemophilia A also called the "ROYAL DISEASE".
Epidemiology: more than 400.000persons affected ,, About 1 in 10.000 people is born
with heamphilia A .
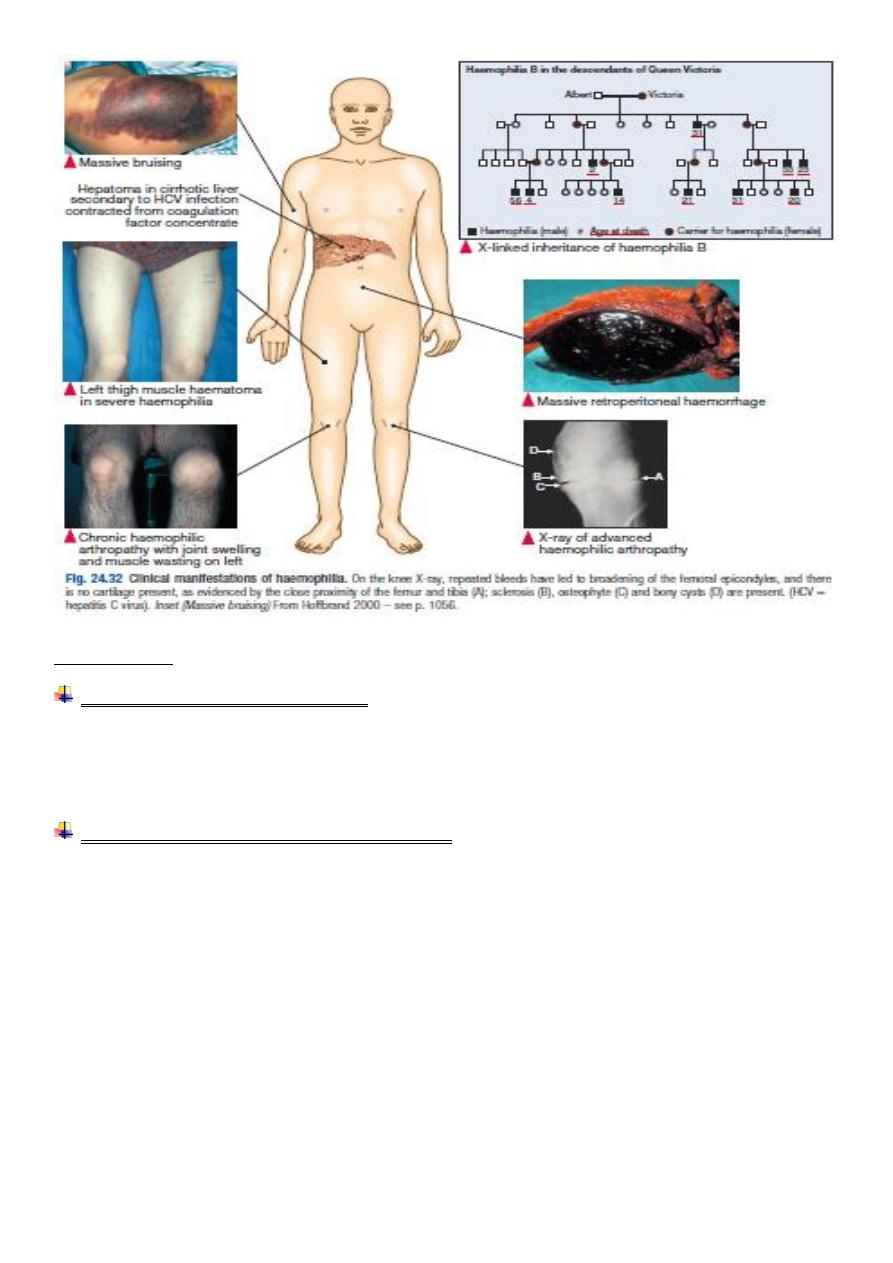
Clinical features
A prolonged aPTT : a normal aPTT does not exclude mild hemophilia A because the aPTT
may not be sufficiently sensitive to detect slightly reduced levels of FVIII-C in the
approximate 20-30% range
Normal PT .
2
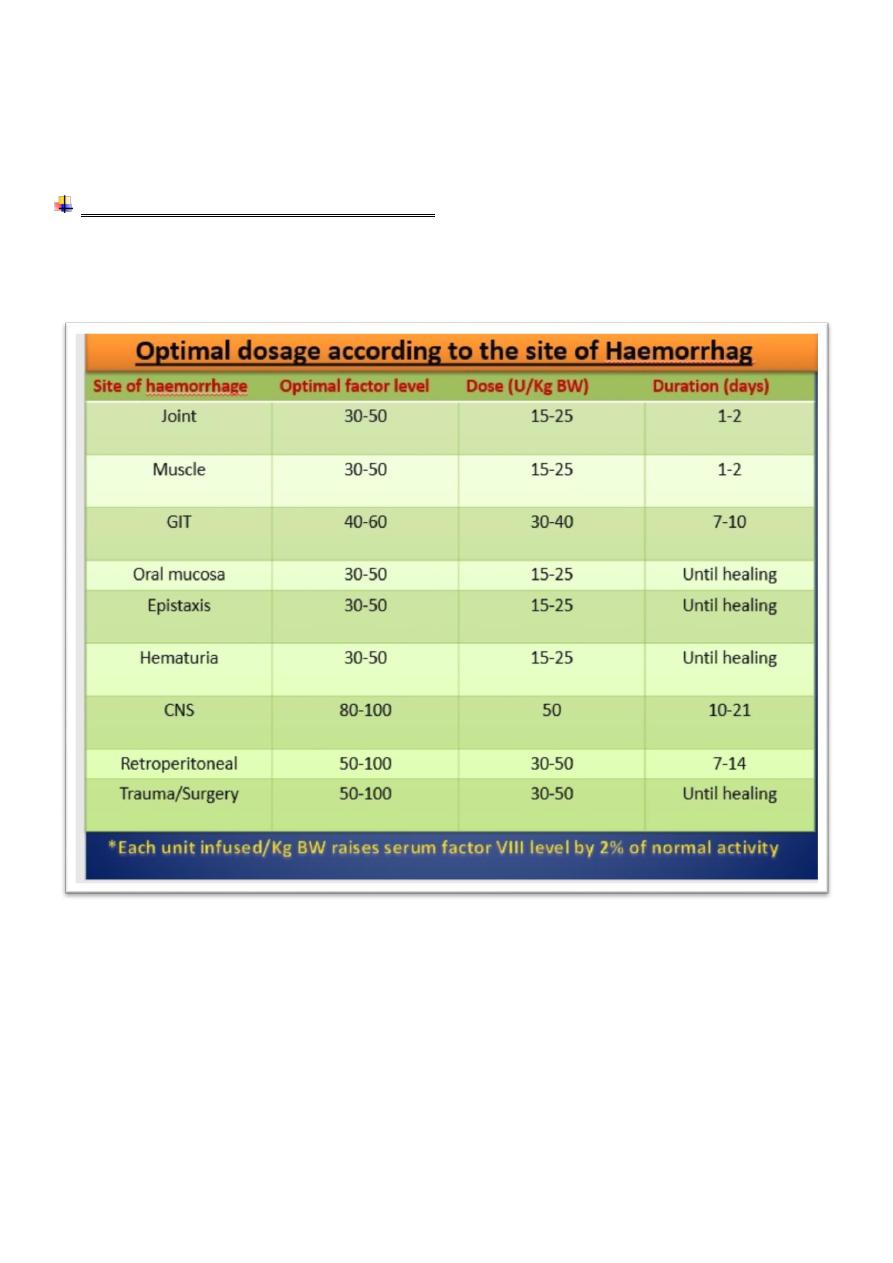
Treatment
Two main Treatment Modalities:
On –demand.
Prophylaxis.
Replacement of missing coagulation factor:
Clotting factor replacements
Clotting factor concentrates (CFCs)
Plasma-derived .
Recombinant.
FVIIa .
Cryoprecipitate in developing countries .
Other pharmacologic agents
Desmopressin (DDAVP) .
Anti-fibrinolytic agent .
Tranexamic acid .
8-aminocaproic acid (EACA) .
3
Supportive measures
Rest.
Ice.
Compression.
Elevation.
Complication of clotting factor therapy :
Infection ; HIV, HBV, HCV.
Anti factor VIII inhibitor in 20 % , treated by infusion of activated factor VIIa OR
factor VIII inhibitor bypass activity (FEIBA).
Haemophilia B ( Christmas disease )
Due to deficiency of factor IX .
X-linked .
Clinical manifestation indistinguishable from haemophilia A .
Treatment ; factor IX concentrate , indication and dosing same as to haemophilia A.
Complication of therapy similar to haemophilia A regarding transmission of infection
BUT the incidence of inhibitor is < 1%.
4
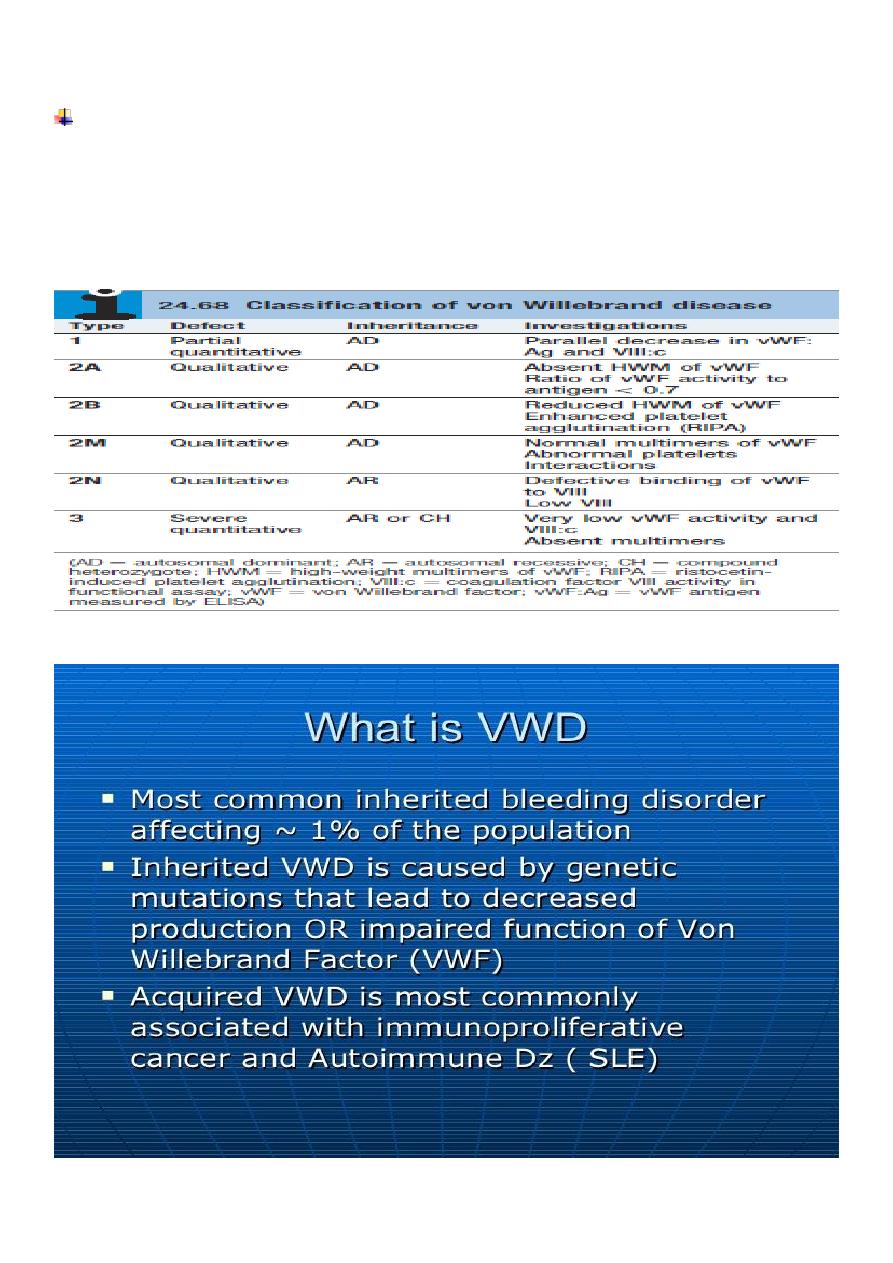
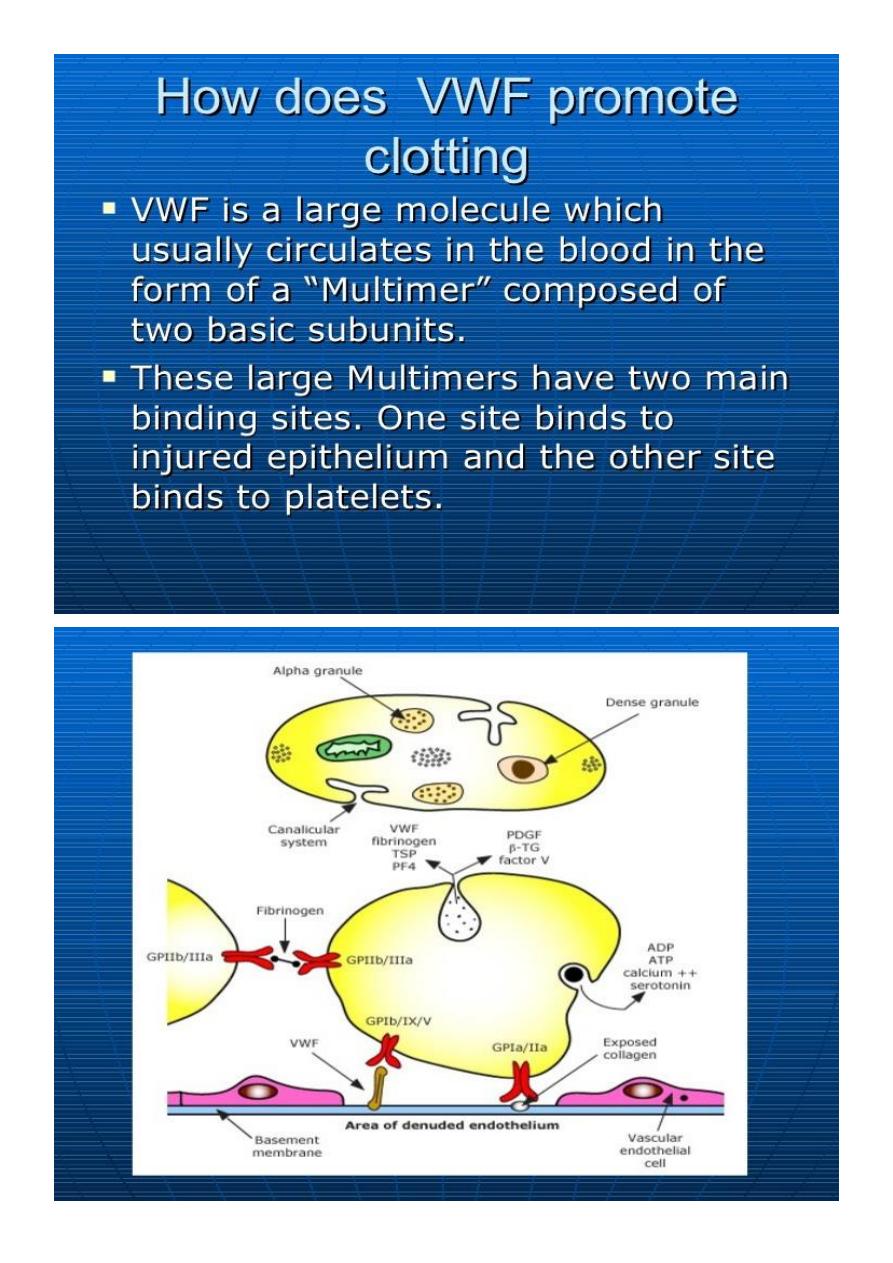
Von Willebrand disease
von Willebrand factor
Synthesis in endothelium and megakaryocytes
Forms large multimer
Carrier of factor VIII
Anchors platelets to subendothelium
Bridge between platelets
5
6
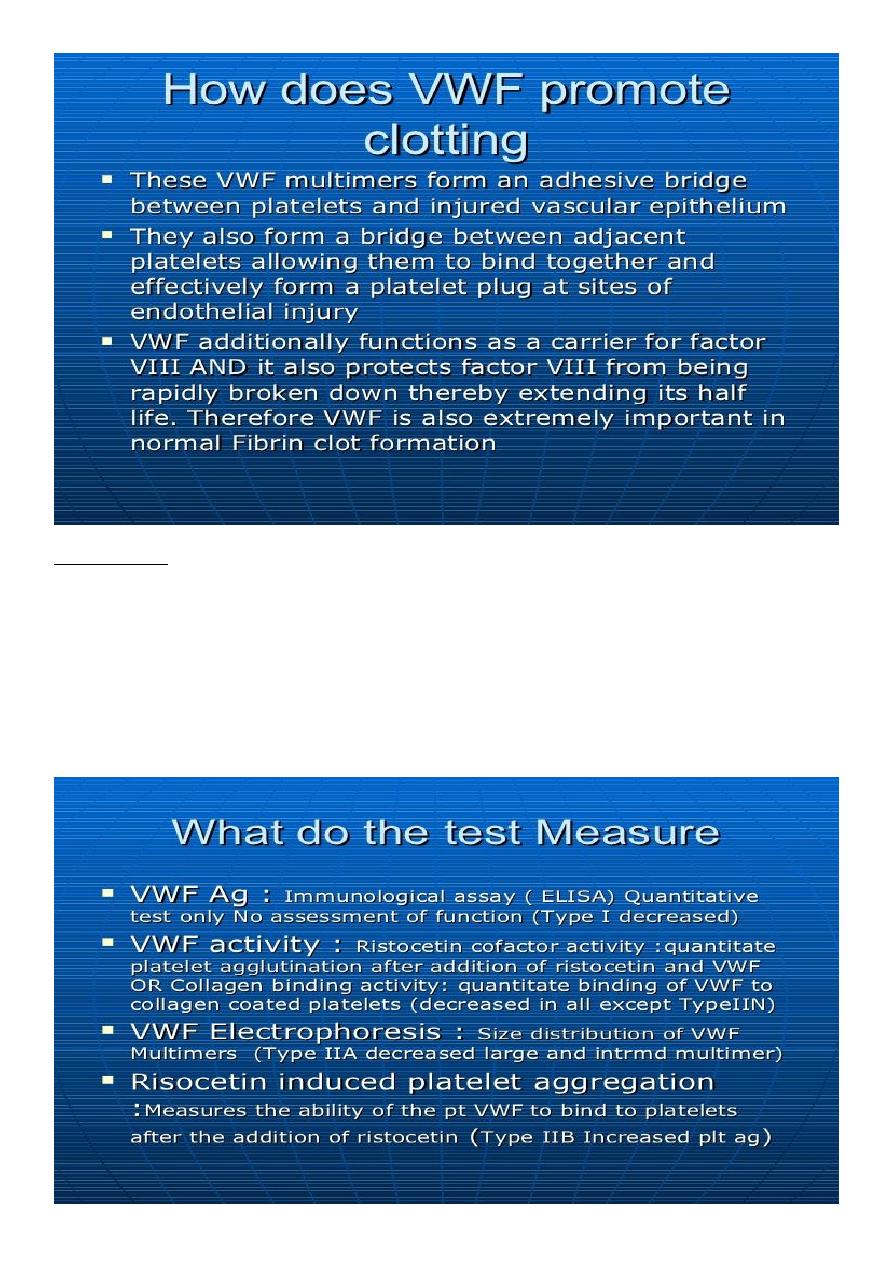
Lab Studies:
Screening tests typically include :
prothrombin time (PT).
activated partial thromboplastin time (aPTT),
FVIII level.
ristocetin cofactor (RCoF) activity.
vWF antigen (vWF:Ag).
7
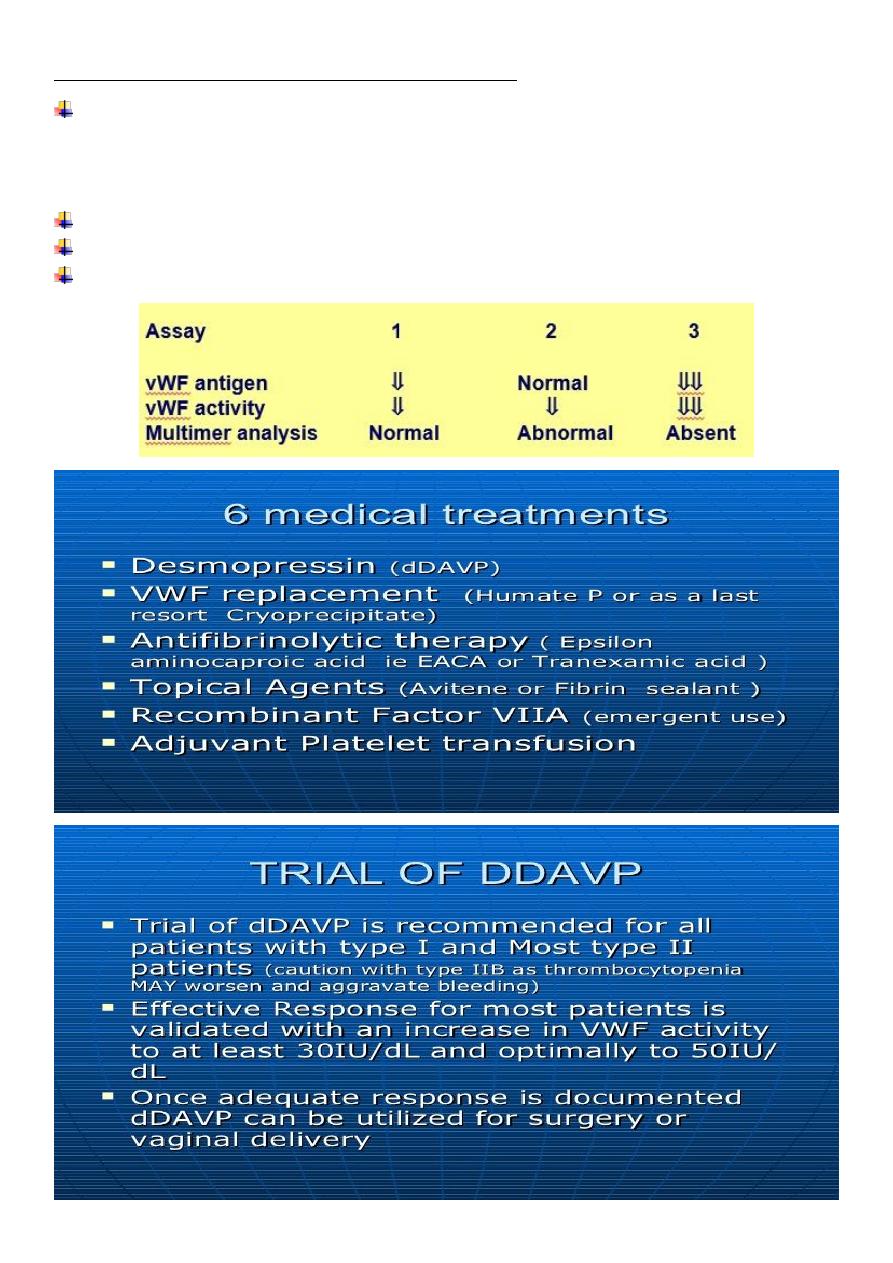
Laboratory evaluation of von Willebrand disease:
Classification
Type 1
Partial quantitative deficiency.
Type 2
Qualitative deficiency.
Type 3
Total quantitative deficiency.
Bleeding time ↑.
aPTT ↑.
vWD type :-
8
9
10
11
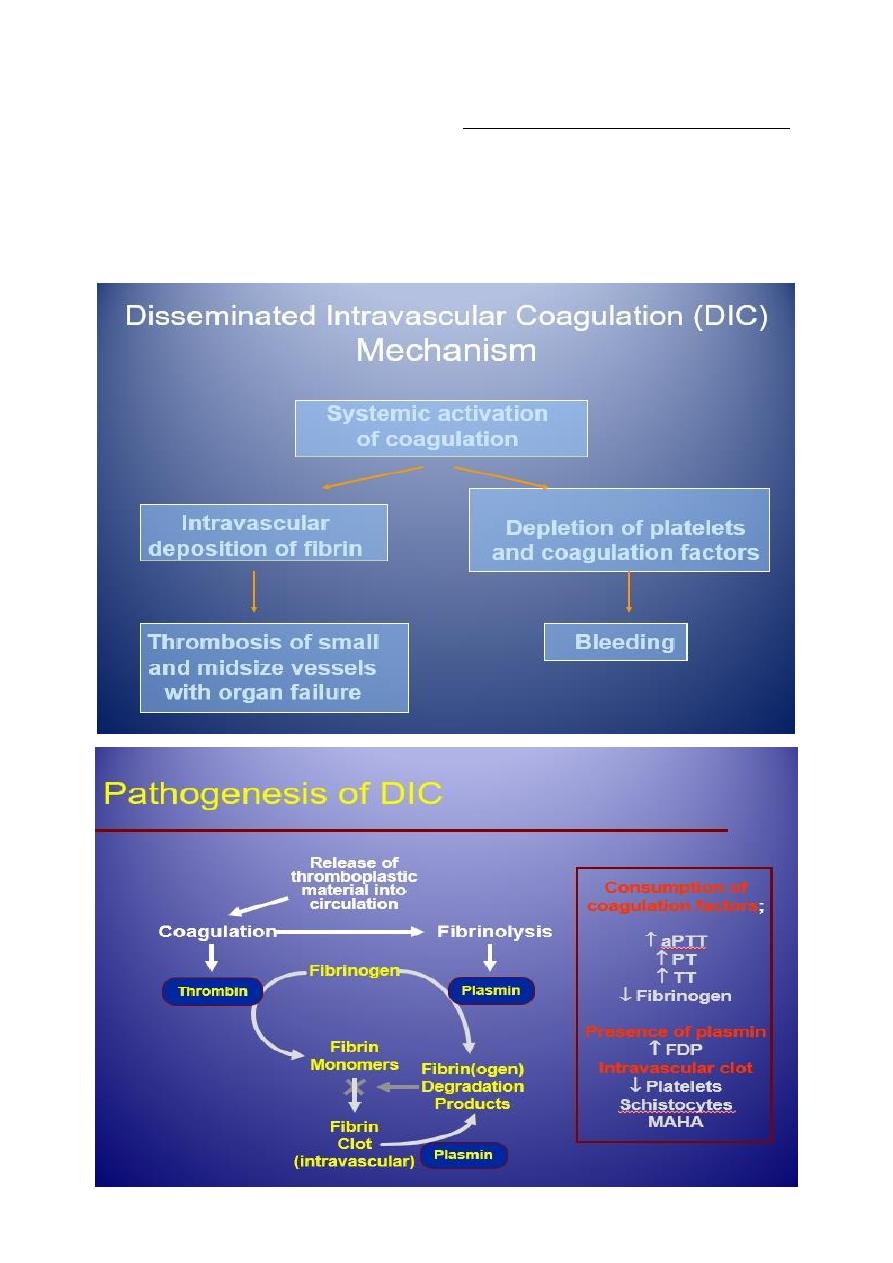
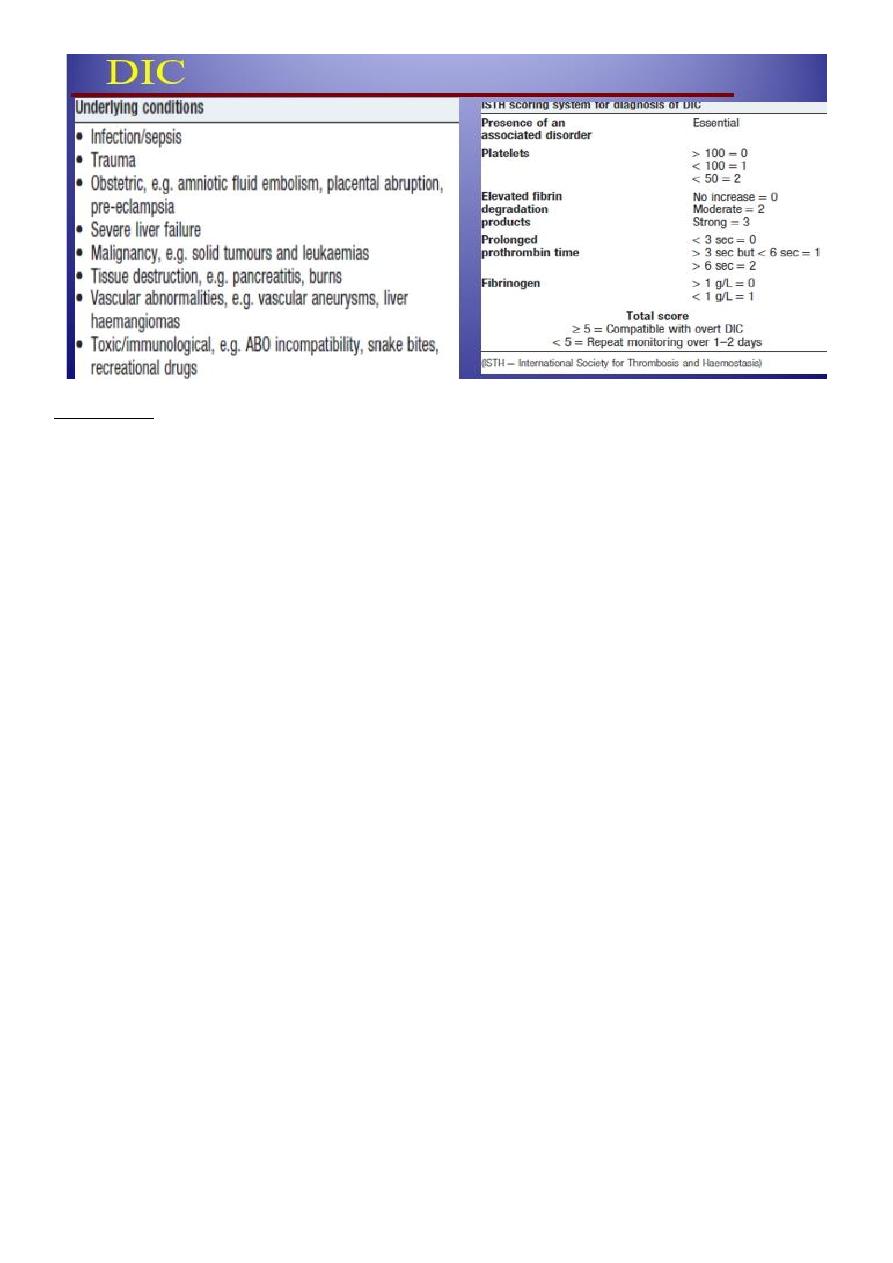
Disseminated intravascular coagulation (DIC)
DIC is a clinicopathologic syndrome in which widespread intravascular coagulation is
induced by procoagulant that are introduce or produce in circulation and overcome the
natural anticoagulant mechanisms.
DIC may cause tissue ischemia from occlusive microthrombi as well as bleeding from
both consumption of platelet and coagulation factor and anticoagulation effect of
product of secondary fibrinolysis.
12
Treatment
Treatment of underlying disorder.
Platelet transfusion (6-10 U plat ) ideally rise to more than 50000-100000.
Fresh frozen plasma;1-2 unit For coagulation factor depletion.
Hypofibrinogenaemia ; 8-10 U cryoprecipitate.
Anticoagulation with heparin; unless there is a clear contraindication.
Coagulation inhibitor concentrate (ATIII).
Patients with DIC should not be treated with antifibrinolytic therapy, e.g.tranexamic
acid.
Thrombotic thrombocytopenic purpura ( TTP )
thrombosis is accompanied by paradoxical thrombocytopenia,
TTP is characterised by a pentad of findings, although few patients have all five
components:
Thrombocytopenia.
microangiopathic haemolytic anaemia (MAHA).
neurological sequelae.
fever.
renal impairment.
It is an acute autoimmune disorder mediated by antibodies against ADAMTS-13 (a
disintegrin and metalloproteinase with a thrombospondin type-1 motif).
It is a rare disorder (1 in 750 000 per annum), which may occur alone or in association
with drugs (ticlopidine, ciclosporin), HIV, shiga toxins and malignancy.
It should be treated by emergency plasma exchange. Corticosteroids, aspirin and
rituximab also have a role in management.
Untreated mortality rates are 90% in the first 10 days, and even with appropriate
therapy, the mortality rate is 20–30% at 6 months.

13
THROMBOTIC DISORDERS
Virchow’s Triad
Pathogenesis of a Thrombus:
Endothelial injury
Abnormal blood flow
Hypercoagulability
• Genetic.
• Acquired.
Signs & Symptoms
DVT:
50% with no clinical signs
Edematous extremity
Plethoric,Warm,Painful extremity
PE:
o Cough, SOB, Hemoptysis.
o Tachycardia.
Thrombophilia
Physiologic Inhibitors of coagulation
Antithrombin
Activated Protein C + protein S
Inactivates Va and VIIIa (via proteolysis)
Thrombomodulin
Binds to thrombin
activate Protein C
Hereditary Thrombophilias
Protein C pathway
Factor V Leiden
Protein C deficiency
Protein S deficiency
14
Prothrombin G20210A mutation
Antithrombin deficiency
Hyperhomocystinemia
C677T MTHFR mutation
Hereditary Thrombophilias
None of them is strongly associated with arterial thrombosis.
All are associated with a slightly increased incidence of adverse outcome of
pregnancy,including recurrent early fetal loss, but there are no data to indicate that any
specific intervention changes that outcome.
Apart from in antithrombin deficiency and homozygous factor V Leiden, most carriers of
these genes will never have an episode of VTE; if they do, it will be associated with the
presence of an additional temporary risk factor.
There is little evidence that detection of these abnormalities predicts recurrence of VTE.
None of these conditions per se requires treatment with anticoagulants.
Antiphospholipid Antibody Syndrome
Autoimmune Acquired Prothrombotic Disorder.
Very High Risk for recurrent thromboembolic disease ;
• both venous and arterial.
Indefinite duration anticoagulation recommended +/- immunosuppression.
Strict Diagnostic Criteria.
Clinical criteria (≥1 must be present):
1. Vascular thrombosis:
- ≥ 1clinical episode of, objectively confirmed, arterial, venous, or small vessel
thrombosis.
2. Pregnancy morbidity:
- ≥ 1 unexplained fetal death @ ≥ 10 weeks EGA.
- ≥ 1 premature birth (≤ 34th week of gestation) due to eclampsia, severe pre-
eclampsia, or placental insufficiency.
- ≥ 3 unexplained consecutive spontaneous abortions @ <10 weeks EGA.
Laboratory criteria (≥1 must be present):
Lupus anticoagulant {LA} (+) ≥ 2 occasions, at least 12 weeks apart, according to ISTH
guidelines:
o prolonged aPTT, lack of correction with 1:1 mix, and correction with .
Anticardiolipine antibody(ACLA) and/or anti-β2 glycoprotein-I antibody:
o medium or high IgG and/or IgM isotype titer ≥ 2 occasions, at least 12 weeks apart.
o Standardized ELISA assays.