1
Fifth stage
Gynecology
Lec-
Dr.Ahmed
/ /2016
Utero-vaginal prolapse
Objectives of this lecture
To know definition of uterovaginal prolapse
To know predisposing factors
To know symptoms of prolapse, To know differential diagnosis of genital prolapse.
In the majority of adult women, when standing, the uterus is anteverted, the fundus
directed forwards,and anteflexed, the body of the uterus bent forward on the cervix
Definition
Aprolapse is ahernia &is aprotrusion of pelvic organ or structures beyond its normal
anatomical bounderies.The pelvis is devided into three compartments,
Antrior :contain urethra&bladder
Middle :contain utrerine or vault descent&enterocele
Posterior :contain rectum
Structures involved in the prolapse
1. Acystocele occurs when the bladder descends through pubocervical fascia
2. Urethrocele occurs because of loss of support by the pubocervical fascia&posterior
pubourethral ligaments
3. Descend of uterus&cervix occur when the lateral cervical ligaments become weakened
4. Vault prolapse occurs following hysterectomy due to inadequate support by lateral
cervical ligaments
5. Rectocele represent increased hiatus between left&right portions of levator ani muscle
2
Prevalence
It is estimated that prolapse affect 12-30% of multiparous &2% of nulliparous women
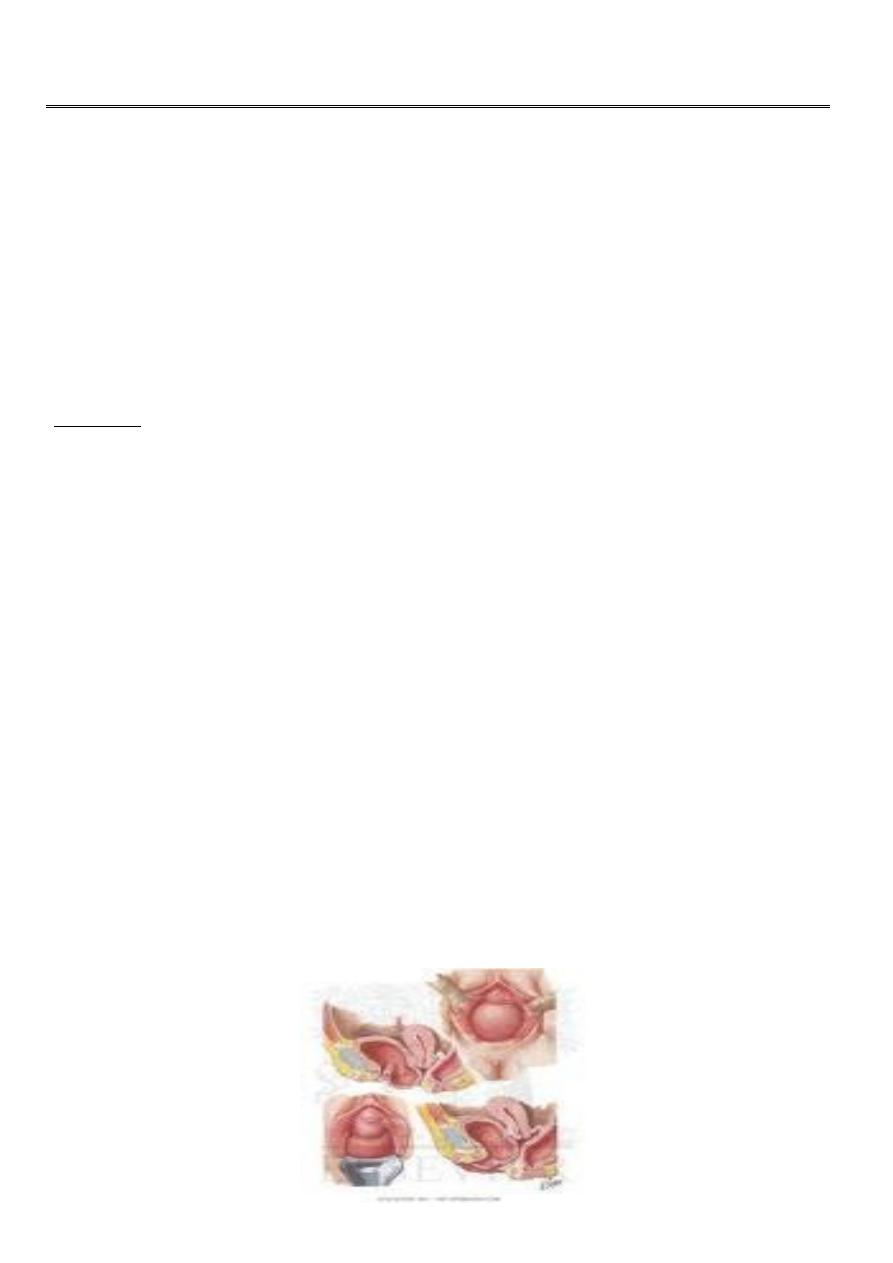
Grading
Three degrees of prolapse are described & the lowest or most dependant portion of the
prolapse is assessed whilst the patient is straining
i. 1st degree: descent within vagina
ii. 2nd degree: descent to the introitus
iii. 3rd degree: descent outside introitus which is termed procidentia & is usually
accompanied by cystourethrocele & rectocele
Aetiology
The connective tissue, levator ani & intact nerve supply are vital for the maintenance of
position of the pelvic structures&are influenced by pregnancy,child birth&aging.
Congenital weakness of the pelvic floor may occur with bladder extrophy.
Altered collagen metabolism
Congenital shortness of the vagina & deep uterovesical pouch.
Race :a decrease in prevalence of prolapse among black women may be due to better
connective tissue or lumber lordosis that encourage diversion of abdominal forces
towards abdominal wall rather than pelvic diaphragm
Acquired factors include:
1-Child-birth which lead to denervation&mechanical injury of the pelvic floor.
2-Rise in intra-abdominal pressure associated with chronic obstructive airway
disease,smoking,constipation&ascitis.
3-Lack of vitamin c &corticosteroid therapy.
4-Surgery as burch colposuspension
5-loss of supporting hormones as in menopause
3
Clinical presentation
Symptoms of prolapse depends on the type&site of prolapse.
Discomfort is usually caused by abnormal tension on nerves of the tissues that
stretched.
Feeling of ablump in the vagina which usually worse towards the end of the
day&relieved by lying down.
Cystocele may lead to dragging discomfort & urinary symptoms:
The commonest urinary symptom is stress incontinence if there is descent of
urethrovesical junction.
Voiding difficulty can occur if large cystocele is present&bladder neck is normal in
position so the woman has to reduce the mass digitally in order to pass urine with
incomplete emptying of bladder which may lead to overflow incontinence.
Alarge cystocele may lead to increased frequency due to persistant residual urine or
recurrent urinary tract infection because of stasis.
Urgency&frequency are found in association with cystocele which may developed as self
induced habit to keep the bladder empty.
Uterine descent cause low backache, protrusion of cervix & blood stained discharge.
Enterocele&vault prolapse may produce vague symptoms of discomfort,rarely
dehiscence of the vault with acute abdomen&small bowel may be seen at the vulva.
Rectocele gives rise to symptoms of backache, lump & incomplete bowel emptying.
Clinical examination
The patient is examined in lithotomy or left lateral position with sims speculum. Stress
incontinence is demonstrated when the bladder is full&the patient is asked to cough or
bear down. Anterior wall descent or uterine descent will be demonstrated by retracting the
posterior vaginal wall.
Enterocele &rectocele can be demonstrated by using the speculum to retract the anterior
vaginal wall.
If the cervix protrude outside the vagina,it may be ulcerated&hypertrophied.
Full pelvic examination should be performed to exclude pelvic mass that may cause the
prolapse.
4
Differential diagnosis
a) Anterior vaginal wall cyst
b) Urethral diverticulum
c) Large uterine polyp
d) Metastasis from uterine tumour
Investigations
Mid-stream urine specimen sent for culture&sensitivity prior to further investigations.
Stress incontinance should be evaluated ,if urinary frequency is present urinary diary is
completed with morning acid-fast bacilli.
Anterior vaginal wall can be imaged with perineal ultrasound.
Vaginal endosonography ,flouroscopy&MRI can be used.
PREVENTION
Shortening of the second stage of delivery&reducing traumatic labour,decrease use of
forceps may result in fewer women developing prolapse.
Women should avoid smoking ,constipation&heavy work.
The benefit of episiotomy &HRT at menopause have not been substantiated.
Treatment
Prior to specific treatment attempts should be made to correct obesity,chronic cough or
constipation .
If the prolapse is ulcerated aseven day course of local estrogen should be administrated.
1. Medical treatment
Before safe anesthesia&surgery ,prolapse was managed by avariety of pessaries of different
shapes&sizes.But nowadays the indications of pessary treatment are:
During&after pregnancy awaiting involution of tissues.
As therapeutic test to confirm benefit of surgery.
When the patient has not completed her child-bearing.
When she is medically unfit.

5
If the patient wish conservative treatment.
While awaiting surgery.
Pessaries are the most popular form of conservative treatment ,made of silicon –rubber or
inert plastic. They are inserted into vagina &need replacement at intervals of three months
to one year.
The most common pessary is ring-shaped of variable sizes.Shelf pessaries are also used in
women who cannot retain ring pessary.
Complications of pessaries
Vaginal ulceration
Infection
Incarceration leading to vaginal discharge&bleeding when pessary has been
forgotten ¬ changed.
2. Surgical treatment
The aim of surgical repair is to restore anatomy&function.There are vaginal&abdominal
operations designed to correct prolapse.Majority of operations are performed through the
vagina&the abdominal route is reserved for recurrence or more complex prolapse.
Cystourethrocele
1-Anterior repair or colporrhaphy is the commonest performed surgical procedure used
to correct cystocele or cystourethrocele &stress incontinence.An anterior vaginal wall
incision is made &the fascial defect allowing the bladder to herniate through is
identified&closed.With the bladder position restored any redundent vaginal epithelium
is exised&incision is closed.
2-Burch colposuspension
Can correct very effectively cystocele&stress incontinence, the lateral vaginal fornices are
approximated & sutured to ipsilateral iliopectineal ligaments
Rectocele
Posterior colporraphy or posterior repair is the commonest procedure
performed.Aposterior vaginal wall incision is made&the fascial defect allowing the rectum
to herniatethrough isidentified&closed.with the rectal position restored any redundant
vaginal epithelium is excised&the incision closed.

6
Enterocele
The surgical principles are similar to anterior&posterior repair but the peritoneal sac
containing small bowel is excised, the pouch of Douglas is closed by approximating the
peritoneum &uterosacral ligaments.
Uterine prolapse
If the woman does not wish to conserve her uterus for fertility then vaginal hysterectomy
with adequate support of the vault to the uterosacral ligaments.
If uterine conservation is required then the Manchester operation is performed,which
involves partial amputation of cervix&approximation of the cardinal ligaments.
Vault prolapse
Sacrocolpopexy is performed by attaching the vaginal vault to the sacrum using amesh&the
pouch of Douglas is closed.