Fifth stage
Dermatology
Lec. 10
.د
منار
16/3/2017
Systemic Lupus Erythematosus
Autoimmune disease affects multisystem
1.5 million cases of lupus
Prevalence of 17 to 48 per 100,000 population
African Americans > Whites
Chronic follows a relapsing and remitting course.
More than 90% of cases of SLE occur in women, frequently starting at childbearing age
Women > Men - 9:1 ratio
Can occur in childhood or later in life
Onset usually between ages of 15 and 45 years,
Clinaical Manifestations
A person has SLE if 4 or more of the 11 criteria are present, serially or simultaneously,
during any interval of observation. (Specificity 95%, sensitivity 75%).
It is important to remember that a patient may have SLE and not have 4 criteria.
Criteria
1. Butterfly rash
2. Discoid lupus
3. Photosensitivity
4. Oral ulcers
5. Arthritis
6. Serositis
7. Neurologic: seizure, psychosis
8. Hematologic cytopenias such as leukopenia, lymphopenia, anemia, or
thrombocytopenia)
9. Renal: acute or chronic renal failure, acute nephritic disease)
10. Immunologic: anti-DNA, anti-phospholipid
11. Anti-nuclear antibody (ANA)
Types of cutaneous lupus
About 80% of patients with SLE have skin involvement (cutaneous LE) and it is the first sign
of SLE
Acute
Subacute
Chronic (discoid)
Lupus profundus
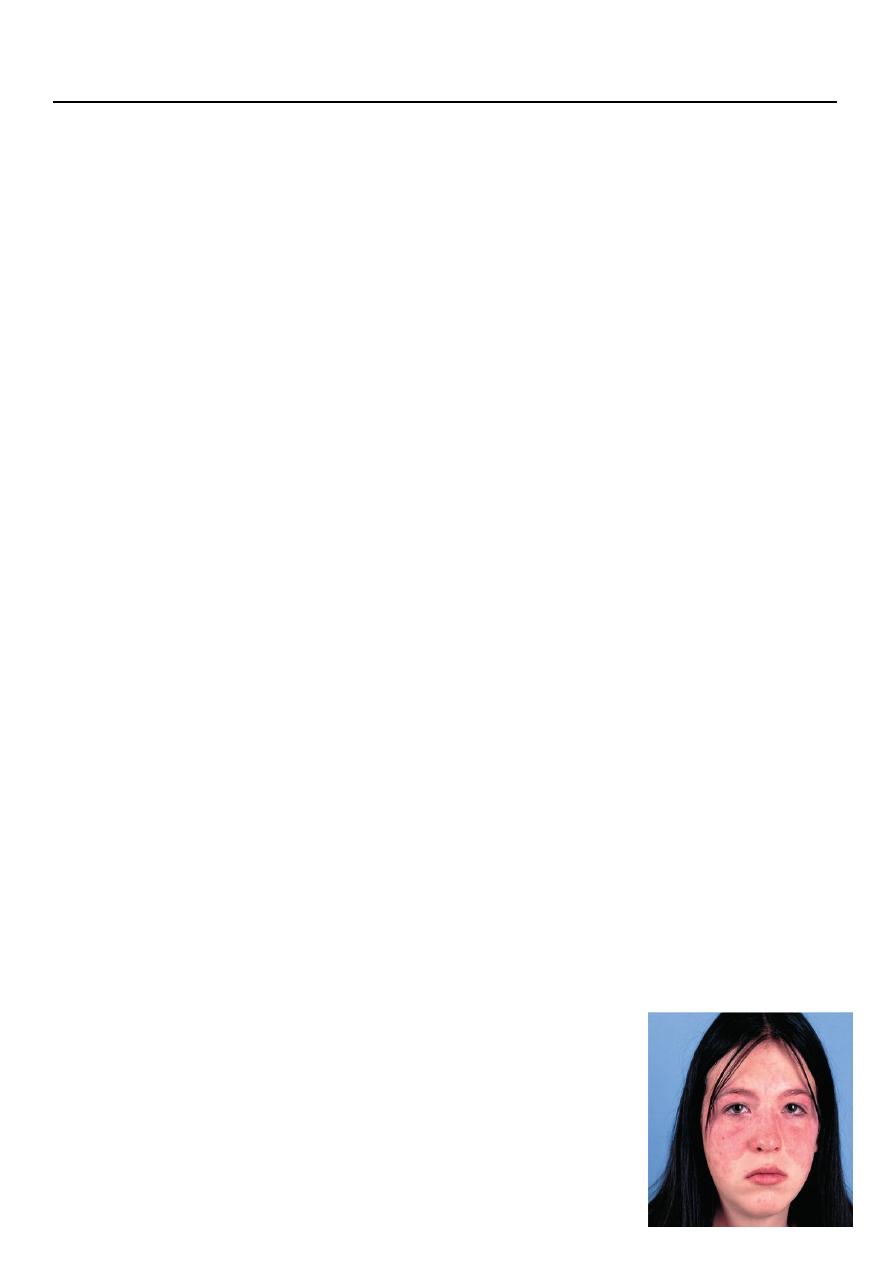
Malar Rash
Most common type is the acute rash
Central face malar rash, flat or raised erythematous butterfly lesion involving both
cheeks and nasal bridge resolves without scarring.
It is photosensitive
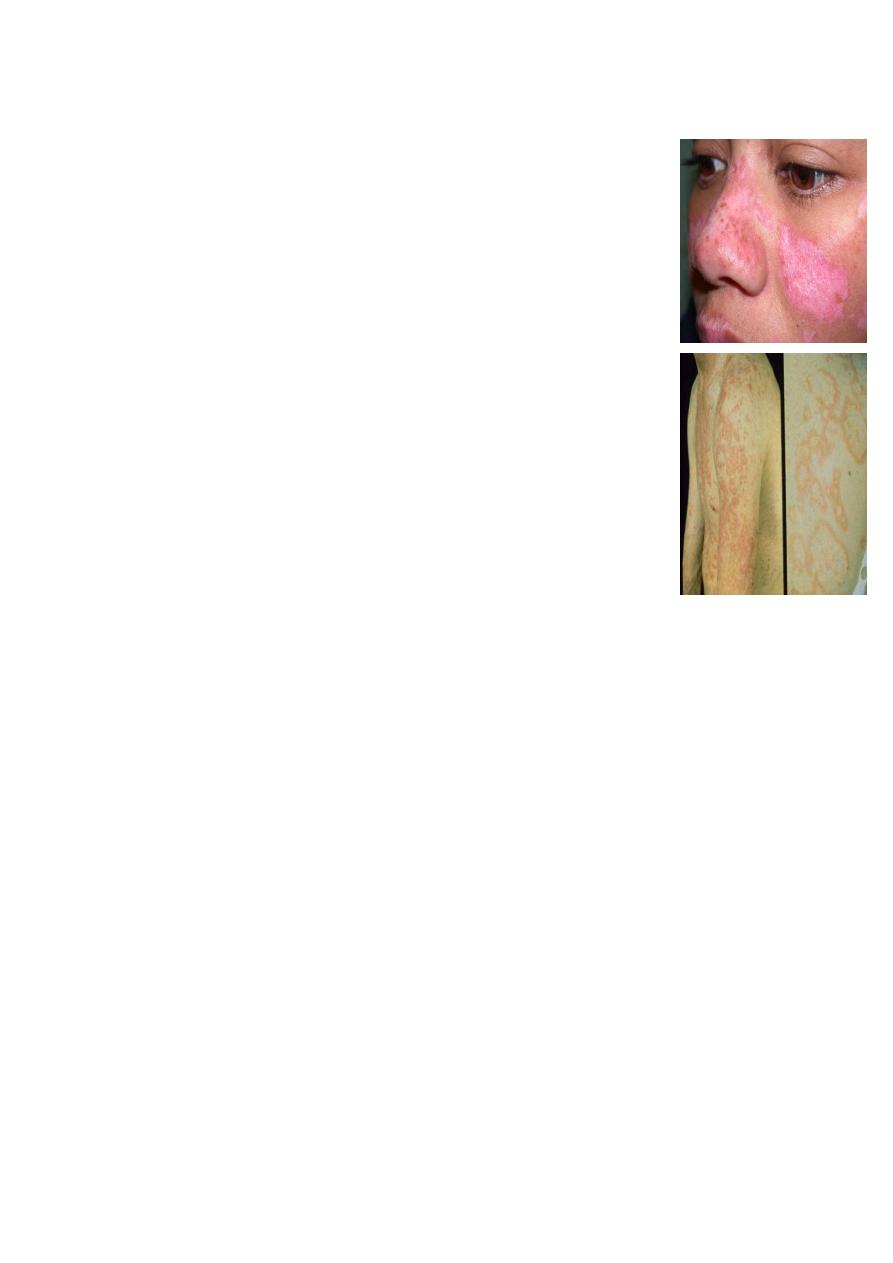
Discoid Lupus Erythematosus (DLE)
Plugged hair follicles and adherent scale.
Atrophy or thinning of the top layer of skin.
Hardness of the skin.
Telangiectasias.
Erythema.
Scarring & permanent hair loss can develop
Subacute cutaneous lupus erythematosus (SCLE)
Typically manifests in 1 of 2 forms:
o Annular/polycyclic
o Psoriasiform/papulosquamos
Lesions typically occur in a photosensitive distribution. Many
patients notice that sun exposure results in an exacerbation of
their disease, and some report worsening each spring and
summer.
Investigations
Blood disorders
o Leukopenia (< 4 × 10 3cells/µL on >1 occasion)
o Lymphopenia (< 1500 cells/µL on >1 occasion)
o Thrombocytopenia (< 100 × 10 3 cells/µL in the absence of offending medications)
o Hemolytic anemia
Renal involvement
o Based on presence of proteinuria (>0.5 g/day or 3+ positive on dipstick testing)
o Cellular casts (including red blood cells [RBCs], hemoglobin, granular, tubular, or
mixed) or based on the opinion of a rheumatologist or nephrologist
Antinuclear antibodies (ANAs) indirect immunoflourescent - Higher titers generally
more specific (>1:160); must be in the absence of medications associated with drug-
induced lupus
Immunologic phenomena
o Anti dsDNA
o Aanti-Smith (Sm) antibodies
o Antiphospholipid antibodies (anticardiolipin immunoglobulin G [IgG] or
immunoglobulin M [IgM] or lupus anticoagulant)
Anti (Ro, La antibodies)
(immuno-blot)
LBT lupus band test (direct immuno-fluorescence )
Biopsy

Treatment
Topical steroids (potent ones or intralesional injections in case of discoid lupus)
Sunscreens are mandatory in all cases
Antimalarial agents: Hydroxychloroquin 200 mg twice daily.
Systemic steroids, only for systemic involvement.
Immunosuppressives