THE BREAST
Normal anatomy:-
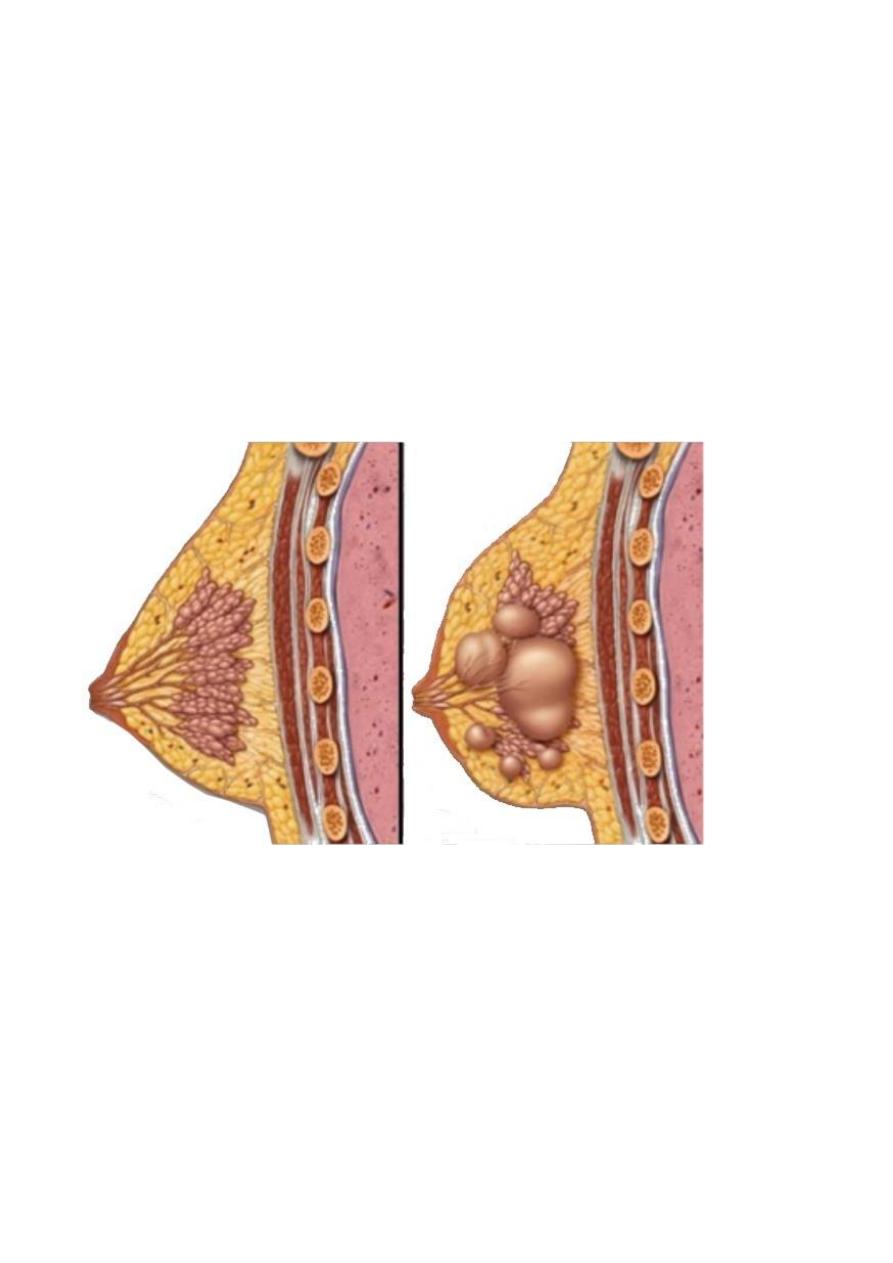
The breast is a modified sweat gland, the morphofunctional unit of the organ is a
single gland which's a complex branching structure that's composed of 2 major parts
terminal duct lobular unit (TDLU) is formed by lobules and terminal ductules and
represent the secretory portion of gland, it connect to subsegmental duct which's lead
to segmental duct and this to a collecting duct which empties into the nipple.
Diseases of breast:-
Benign breast diseases
the vast majority of the lesions that occur in the breast are benign lesions, but much
concern is given to malignant lesions because the breast cancer is the most common
malignancy in the world, so that the most common benign breast lesion are;
I-developmental abnormalities:
Ectopic breast tissue (mammary heterotopia) is the most congenital anomaly of the
breast, the most frequent sites of ectopic breast tissue is seen along the milk line, so
can be seen in chest wall, vulva and axilla, but most common location is the axilla,
they usually have nipple, areola and separate duct system from that of the normal
breast, this ectopic tissue is responds in the same way as the normal breast tissue to
physiological influences, so the absence of duct system may cause symptom of
obstruction during lactation and may be mistaken clinically for carcinoma.
II-Inflammation:
-

1- Acute mastitis:-
caused by bacteria which's gain access through fissures of nipple in
female during lactation .ex. staphylococcus infections caused breast abscess while
streptococcus caused pain, swelling and breast tenderness.
2- Chronic mastitis:-
a- Granulomatous mastitis:-
Characterized by presence of non-caseating granuloma
confined to breast lobules, it had no microorganisms so it's immunologically mediated.
b- Tuberculosis:-
is a rare secondary to blood stream dissemination or local extension,
microscopically composed of typical caseating granuloma of TB.
III. Mammary ductectasia:-
The condition occur in female during reproductive life caused by inspissation of breast
secretion in main excretory duct, this dilation lead to a reactive changes in the
surrounding breast tissue which's infiltrated by inflammatory cells especially
lymphocytes, plasma cells and even granuloma, the importance of this condition is
causing of skin and nipple retraction similar to seen in carcinoma.
IV. Galactocele:-
This is occurring in lactating female due to cystic dilation of obstructive ducts when
ruptured and caused inflammatory reaction in surrounding stroma.
V. Fat necrosis:
-
Which's occur due to trauma (accidental or surgical) the importance of this condition
in causing breast mass and nipple retraction.
VI. lipomas.
Are common benign fatty tumors that can appear almost anywhere in the body,
including the breast they are usually not tender.
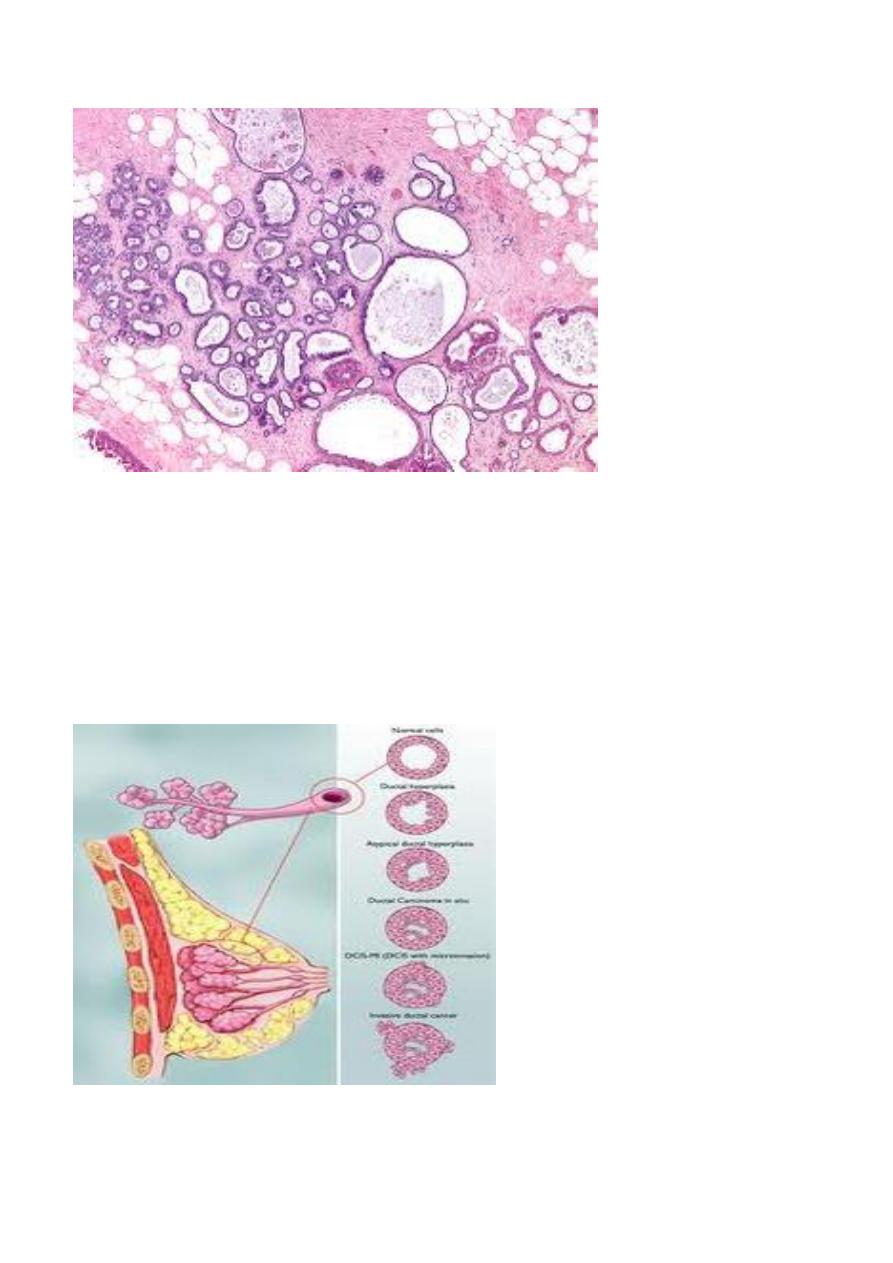
VII. Fibrocystic disease of breast:
-
It is a group of changes occur in breast consist of stromal fibrosis with stromal and
epithelial hyperplasia inducing micro or macrocysts, there are banal of epithelial
hyperplasia the more serious is atypical hyperplasia which's produce palpable lumps
and more risky to develop carcinoma, so fibrocystic disease is divided into:-
A- Non proliferative lesion:-
This lesion include cysts and/or fibrosis without epithelial cell hyperplasia, it is more
common occur in female breast during reproductive life, the disorder is usually
multifocal and often bilateral, the breast is consist of ill defined mass and only
nodularity.
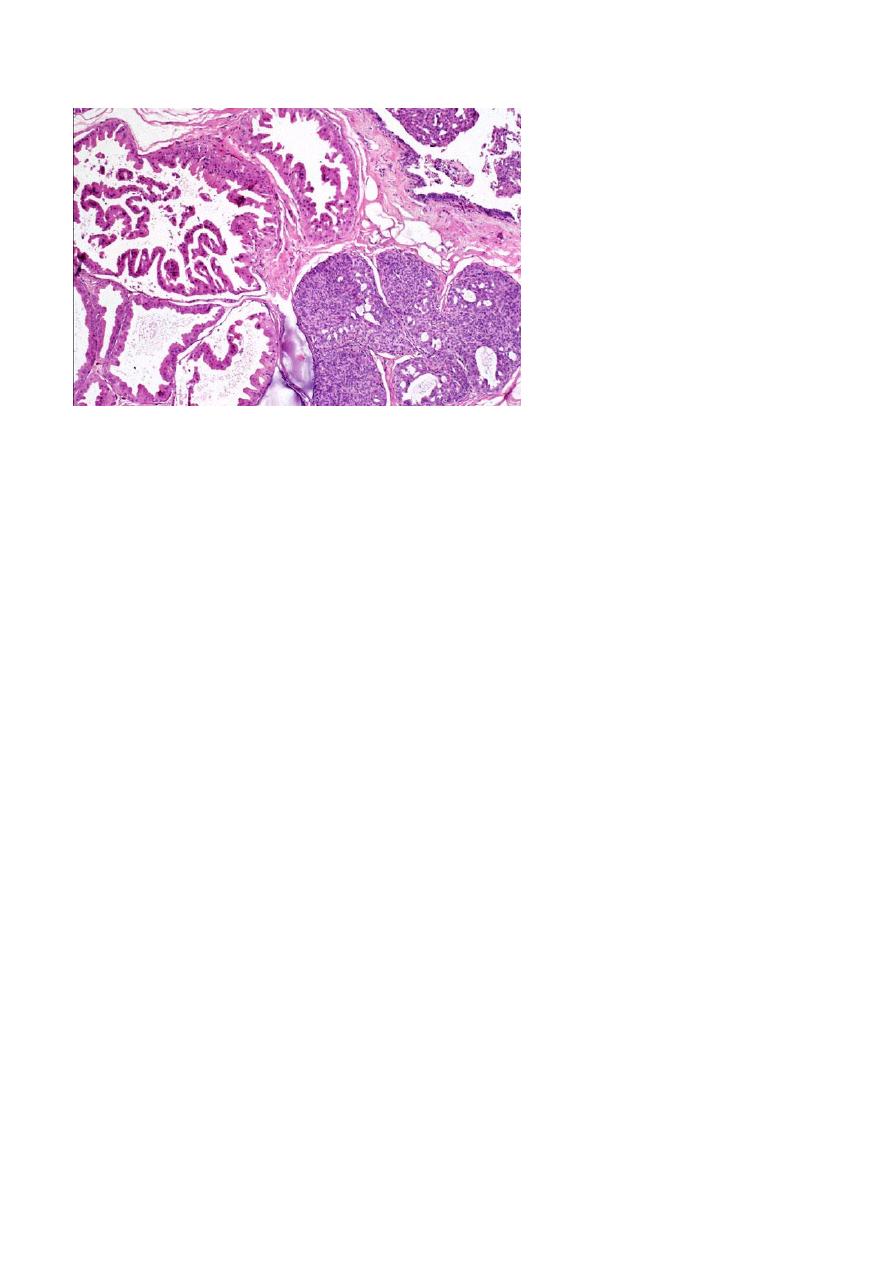
B- Proliferative lesion:-
It is consist of proliferated epithelial cells lined ducts, ductules, or lobules and this
proliferation is either mild hyperplasia which's carry little risk of carcinoma, moderate
and severe hyperplasia, if the hyperplastic epithelial cells multilayered, disordered and
vary in nuclear cell size and shape with nuclear hyperchromasia this approach to
carcinoma in situe, but this is usually preserved myoepithelial cell layer.
Relationship of Fibrocystic disease to breast cancer.
1. Minimal or no increased risk of breast cancer in fibrosis, cystic changes (micro of
macro cystic ) and mild hyperplasia.
2. Slightly increased the risk (1.5 to 2 times) in moderate to florid hyperplasia and
ductal papillomatosis .
3. Significantly increased risk (5 times) in atypical hyperplasia.
4. proliferative lesions may be multifocal and the risk of carcinoma extends to both
breasts.
5. A family history of breast cancer increases the risk in all categories.
VIII. Tumors of breast:
-
Fibroadenoma:-
It is a common benign tumor occur in female breast in young age group, the peak
incidence usually in ages 20-35 years, the estrogen is play important role in it's
development, the tumor usually well capsulated, freely movable hard mass.
Grossly :
appear as hard, firm mass white in colour.
Histologically:
consist of loose fibroblastic stroma with duct like epithelium lined
spaces of various forms and sizes.
Malignant transformation in fibroadenoma found in 0.1% of the cases.
Phyllodes tumor:-
They are much less common than fibroadenoma and are arising from intralobular
stroma, most of these tumor usually benign but some become malignant which there
are increased in stroma cellularity with anaplasia, high mitotic activity and rapid
increase in size.
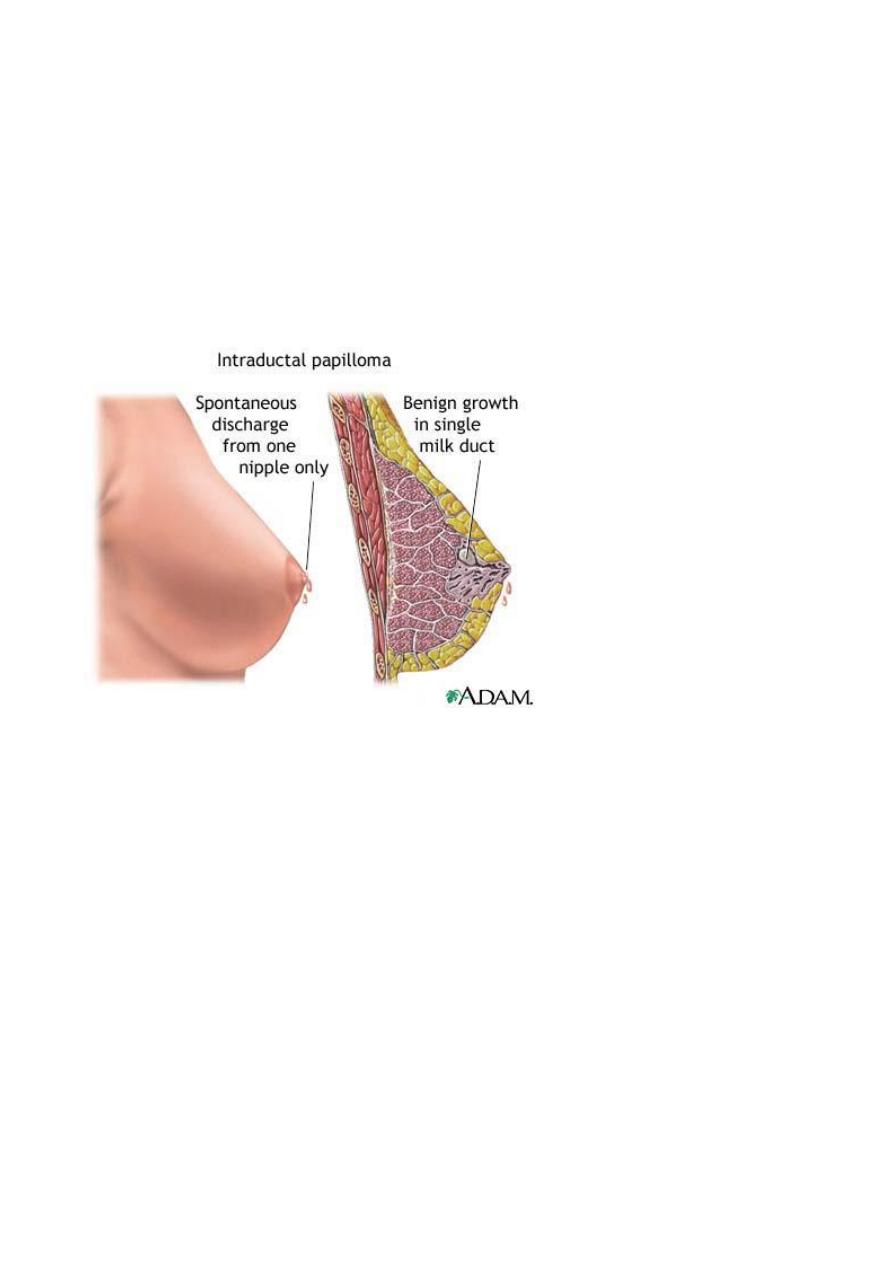
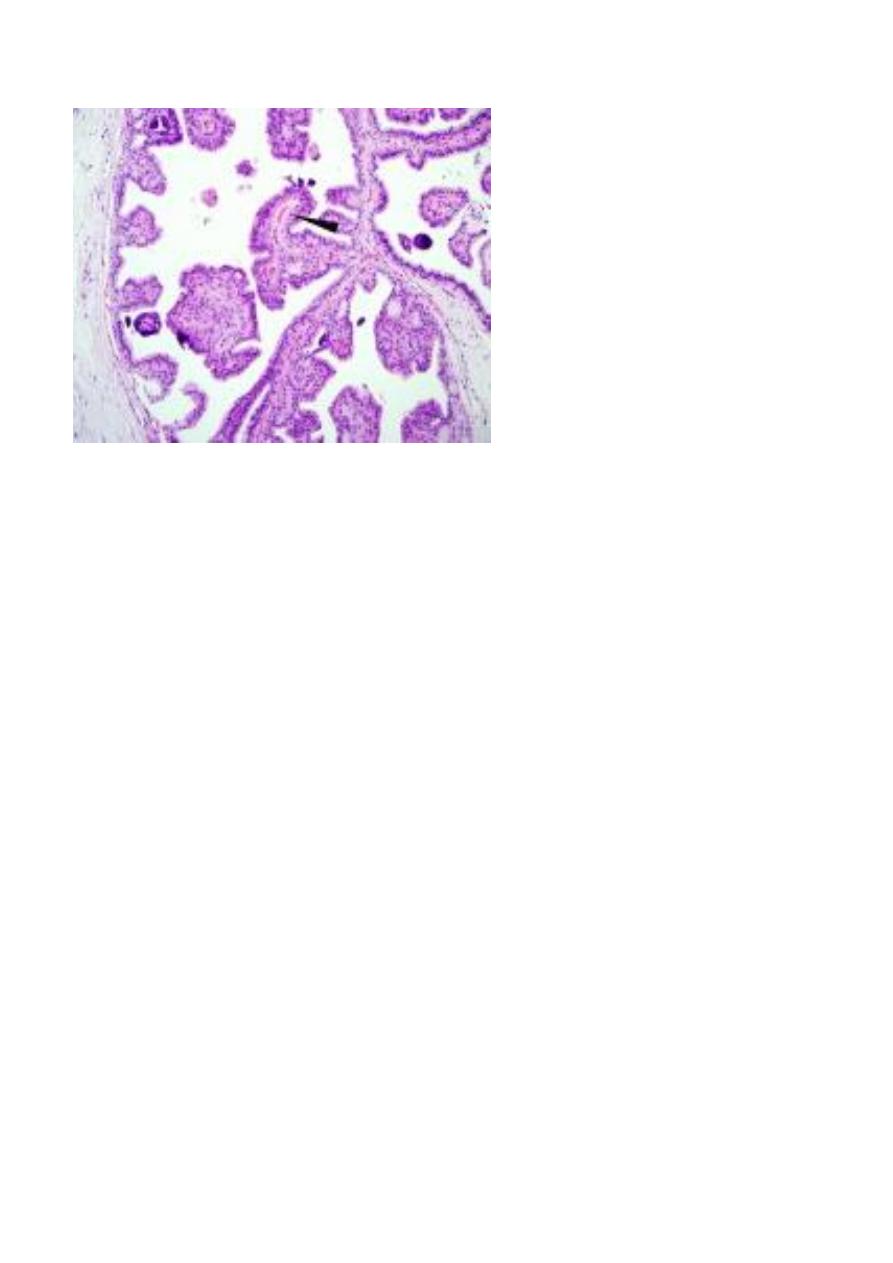
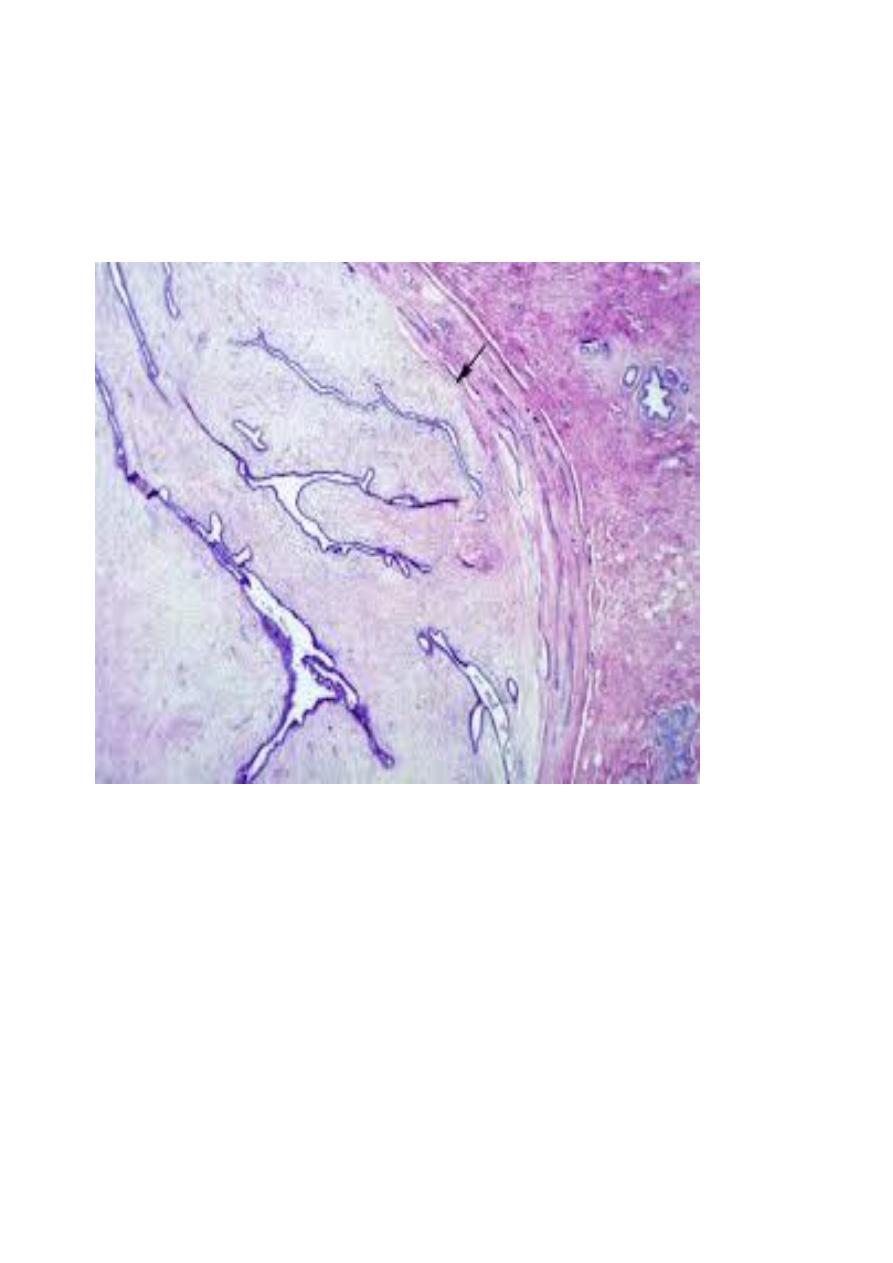
Intraductal papilloma:-
It's a benign papillary growth within a duct, most lesion are solitary occur in common
ducts the presentation are usually characteristic by:-
1- Serous or bloody nipple discharge.
2- Presence of small subareolar tumor.
3- Rarely nipple retraction.
Microscopically:
seen as multiple papillae having fibrovascular core and lined by
cuboidal to columnar epithelial cells usually double layer epithelial and myoepithelial
cells.