1
Fifth stage
Ophthalmology
Lec-13
د.نزار
10/4/2017
The pupil
INTRODUCTION
Movements of the pupil are controlled by the parasympathetic and sympathetic nervous
systems.The pupils constrict (miosis) when the eye is illuminated (parasympathetic
activation, sympathetic relaxation) and dilate (mydriasis) in the dark (sympathetic
activation, parasympathetic relaxation). When the eyes accommodate the eyes converge
and the pupils constrict. The pupils are normally equal in size but some 20% of people may
have noticeably unequal pupils (anisocoria) with no associated disease. The key to
diagnosis of pupillary disorders is to:
• determine which pupil is abnormal;
• search for associated signs.
Disorders of the pupil may result from:
• ocular disease;
• disorders of the controlling neurological pathway;
• pharmacological action.
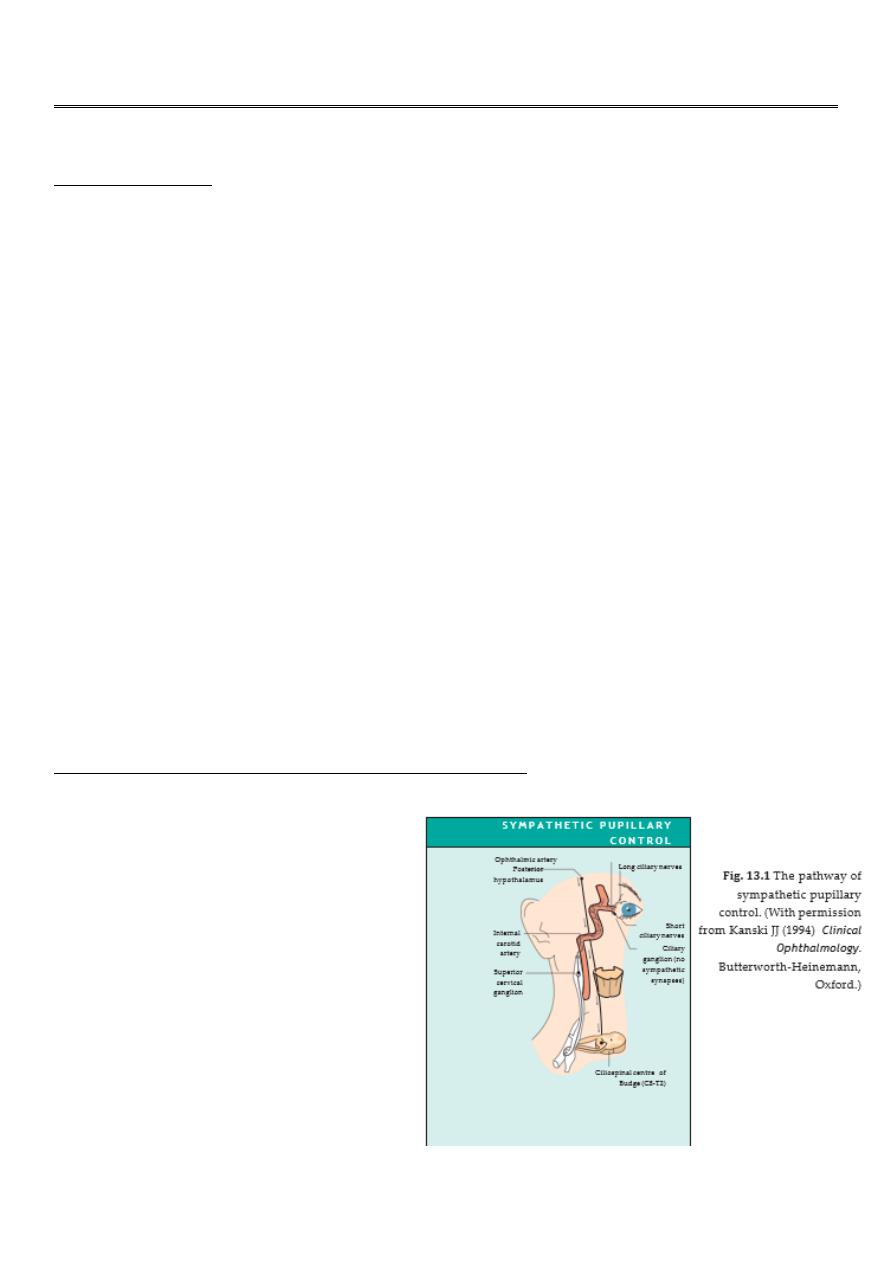
The parasympathetic fibres reach the eye through the third cranial nerve. The sympathetic
pathway is shown in Fig. 13.1.
OCULAR CAUSES OF PUPILLARY ABNORMALITY
• ocular inflammation where
posterior synechiae give the
pupil an irregular appearance
(see p. 91);
• the sequelae of intraocular
surgery;
• blunt trauma to the eye which
may rupture the sphincter
muscle causing irregularity, or
fixed dilation (traumatic
mydriasis).
2
NEUROLOGICAL CAUSES OF AN ABNORMAL PUPIL
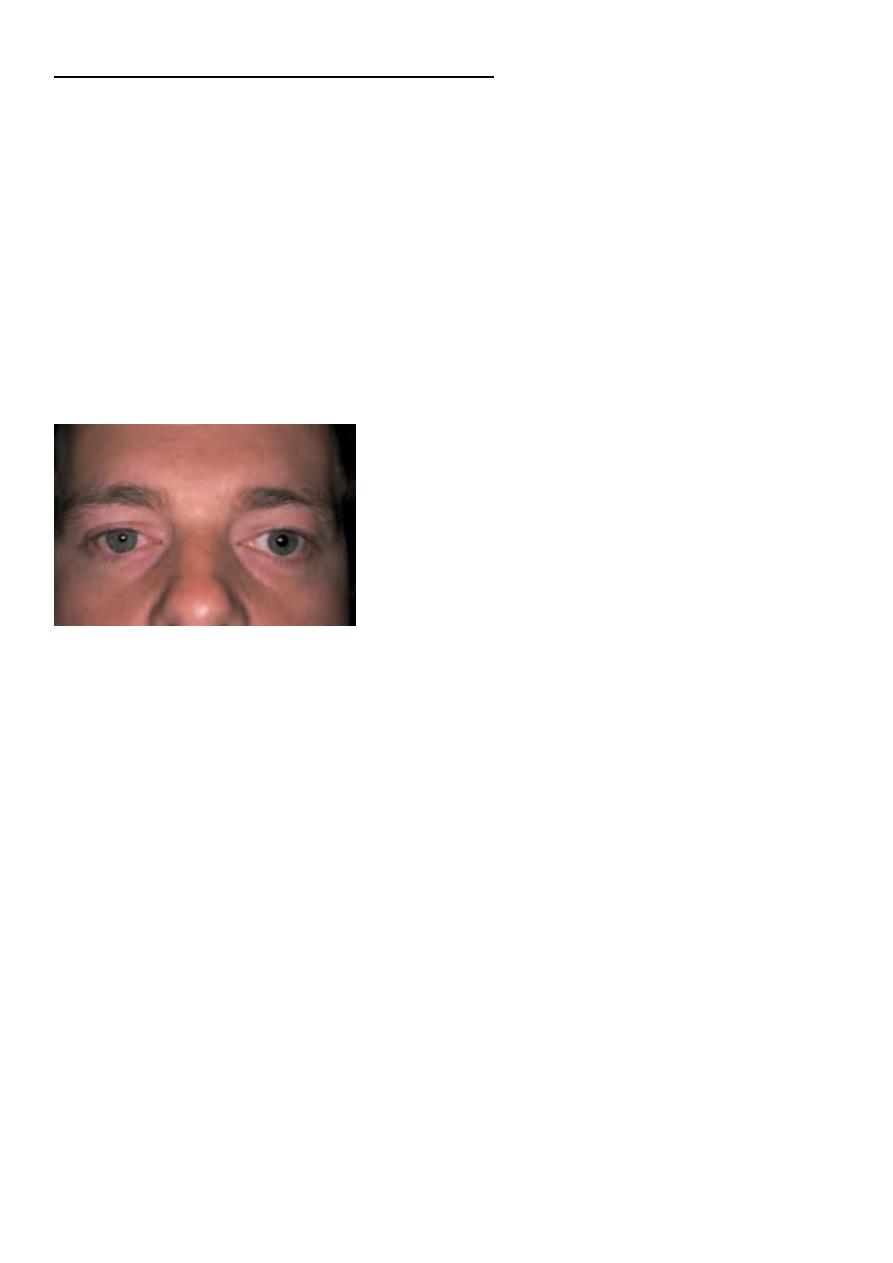
Horner’s syndrome (Fig. 13.2)
Interruption of the sympathetic pathway causes:
• A small pupil on the affected side. This is more noticeable in the dark when the
fellow, normal pupil, dilates more than the affected pupil.
• A slight ptosis on the affected side.
• Lack of sweating on the affected side if the sympathetic pathway is affected
proximal to the base of the skull.
• An apparent enophthalmos
Because of its extended course the sympathetic pathway may be affected by a multitude of
pathologies. Examples include:
• Syringomyelia,
• Disease of the lung apex catches the cervical sympathetic chain (e.g. neoplasia).
Involvement of the brachial plexus gives rise to pain and to T1 wasting of the small
muscles of the hand, in Pancoast’s syndrome.
• Neck injury, disease or surgery.
• Cavernous sinus disease.
• congenital. Here the iris colour may be altered when compared to the fellow eye
(heterochromia).
Fig. 13.2
A right ptosis and miosis in Horner’s syndrome.

3
LIGHT–NEAR DISSOCIATION (ARP-APR)
In these pupillary abnormalities the reaction of the pupils to light is much less than to the
near (accommodative) response. There is no condition in which the light reflex is intact but
the near reflex is defective. A light–near dissociation is seen in diabetes and multiple
sclerosis or may be caused by periaqueductal brainstem lesions (see below).
Relative afferent pupillary defect
A lesion of the optic nerve on one side blocks the afferent limb of the pupillary light reflex
(see p. 25). The pupils are equal and of normal size, but the pupillary response to light on
the affected side is reduced, while the near reflex is intact. This is an important test to
perform in a patient suspected of having an optic nerve lesion, such as optic neuritis. It
may
also, however, be seen in severe disease of the retina. It is not seen with opacities of the
cornea or lens.
Adie’s pupil
This is not an unusual cause of unequal pupil size (anisocoria). It affects young adults and
is seen more commonly in females than males (2 : 1). It is due to a ciliary ganglionitis
which denervates the iris and ciliary body. Parasympathetic fibres which reinnervate the
iris sphincter are those which were previously involved in accommodation. The affected
pupil:
• Is enlarged.
• Is poorly reactive to light. On the slit lamp examination the pupil movement in
response to light is seen as a worm-like (vermiform) contraction.
• Shows slow, sustained miosis on accommodation.
• Is supersensitive to dilute pilocarpine (0.1%).
The ability to accommodate is also impaired, the patient may complain of blurred vision
when looking from a distant object to a near one and vice versa. Systemically the disorder
is associated with loss of tendon reflexes; there are no other neurological signs.
Argyll Robertson pupil
Classically seen in neurosyphilis the pupils are bilaterally small and irregular. They do not
react to light but do to accommodation. The iris stroma has a typical feathery appearance
and loses its architectural detail.
4
Other causes of pupillary abnormality
In coma, both pupils may become miosed but remember that patients taking
pilocarpine for glaucoma or receiving morphine also show bilateral miosis.
Coma associated with a unilateral expanding supratentorial mass, e.g. a
haematoma, results in pressure on the third nerve and dilation of the pupil. Intrinsic
third nerve lesions also cause a dilated pupil (see p. 175). The pupil may also be
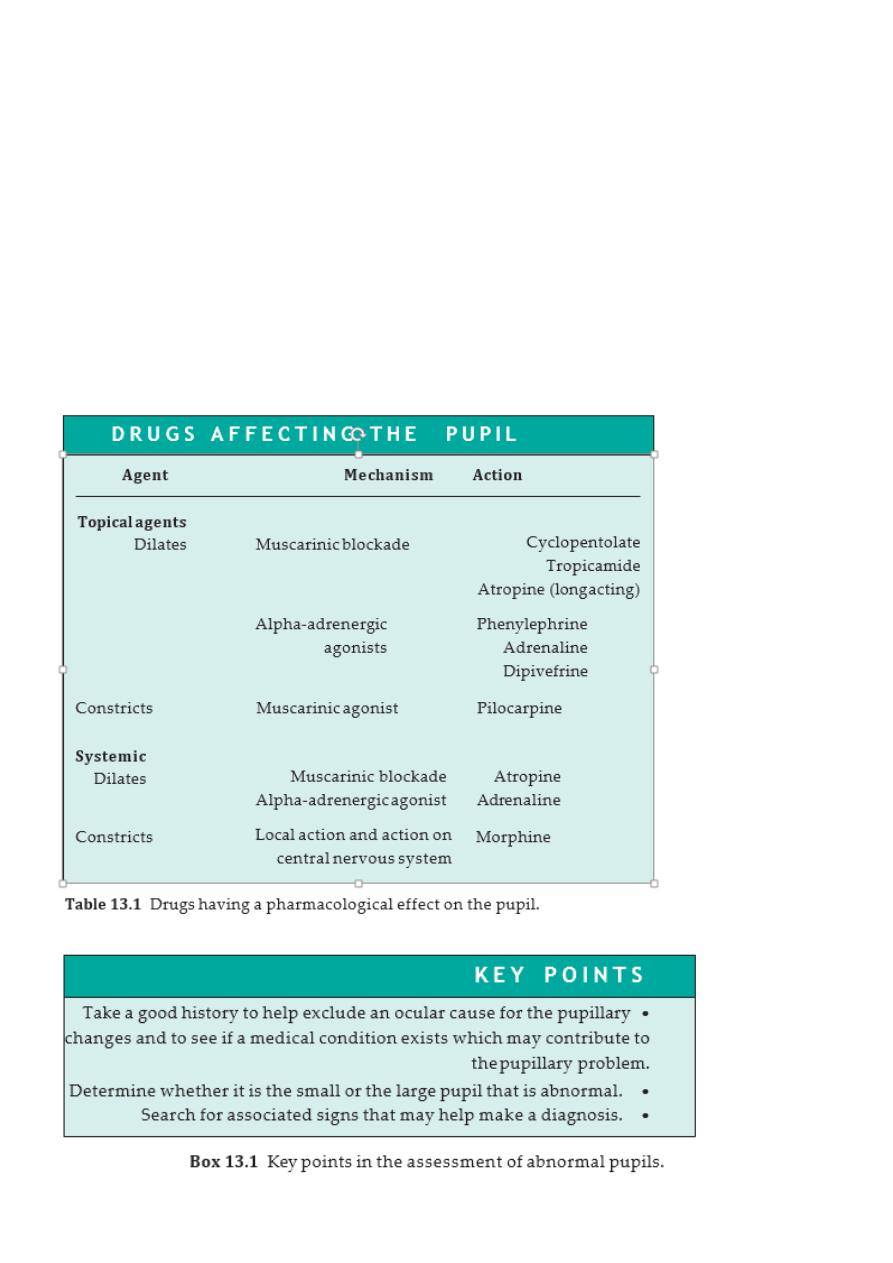
affected by drugs, both topical and systemic (Table 13.1).