
INFECRTION CAUSED BY HELMINTHS
1, Nematodes
2. Trematodes
3. Cestodes
INTESTINAL HUMAN NEMATODES
ANCYLOSTOMIASIS (( HOOK WORM ))
It is cased by Ancylostoma duodenale or Necator americanus.
The adult hookworm is 1 cm length and lives in the duodenum and upper jejunum. eggs
are passed in the faeces and in the moist soil, the larvae develop into the filariform larvae
which is the infective stage which penetrate the human skin and carried to the lungs
where they ascend to the bronchi are swallowed and mature in the small intestine within
4 – 7 weeks.
PATHOLOGY:
The larvae may cause allergic inflammation at the site of entry in the skin.
Heavy infection may cause pulmonary eosinophilia.
The worms attach to the small bowel mucosa and withdraw blood (( 0.15 ml/worm/day
for A. duodenale )).
The degree of anaemia is variable and it deepened on :
1. worm load
2. nutritional status
3. iron store.
CLINICAL FEATURES:
dermatitis usually on the feet (( ground itch ))
paroxysmal cough with blood stained sputum associated with patchy
pulmonary consolidation. (( pulmonary phase )).
Vomiting and epigastric pain may occur.
Iron deficiency anemia, protein losing enteropathy and hypoproteinemia.
Cardiac failure may result from chronic iron deficiency.
INVESTIGATIONS:
1. eosinophilia
2. the characteristic ovum can be recognized in the stool.
3. faecal occult blood test will be positive.
MANAGEMANT
mebendazole 100 mg/12 hr. for 3 days or single dose albendazole 400mg.
oral iron for treatment of anemia.
ASCARIS LUMBERICOIDES (( ROUND WORM ))
Pale yellow nematode 20 – 35 cm length. Human are infected by eating food
contaminated with ova. Ova will hatch in the duodenum to larvae which migrate
through the lungs, ascend the bronchial tree, from which they may be swallowed and
mature in the small intestine.
CLINICAL FEATURES:
variable symptoms from vague abdominal pain to malnutrition
obstructive complications: intestinal complications mainly in the terminal
ileum or bile duct obstruction.
INVESTIGATIONS;
Diagnosis by demonstration the ova in the faeces

Adult warm may be expelled orally or rectally
Ba. Meal may demonstrate the adult warm.
Eosinophilia
Treatment;
Mebendazole 100 mg/12 hr. for 3 days OR
Albendazole 400 mg single dose OR
Piperazin 4 gm as single dose
For obstructive complications: i.v fluid, nasogastric suction and
piprazine.
PREVENTION:
Community chemotherapy regimen
OR
Treating school age group.
ENTEROBIUS VERMICULARIS
(( Thread worm )) (( Pin worm ))
It is common world wide, mainly children, after
swallowing of the ova, development take place in
the small intestine but the adult worms are found
chiefly in the colon.
CLINICAL FEATURES:
The gravid female worm lays ova around the
anus causing intense itching especially at night,
the ova carried to the mouth by the fingers ((
auto Re- infection ))
Adult worm may be seen moving on the buttocks
or in the stool.
INVESTIGATIONS:
Adhesive cellophane tap to
the perianal skin in the
morning to detect the ova.

Perianal swab moistened with
saline
TREATMENT
Single dose mebendazole 100 mg OR
Albendazole 400mg OR
Piperazine 4 gm
Treatment may be repeated after 2
weeks.
All the family members should be
treated.
Clothes, bed liven, nail cutting.
TREMATODES (( FLUKES ))
Leaf – shaped
SCHISTOSOMIASIS
There are 3 species of the genus
Schistosoma causing the disease in
human:
S. haematobium, S. mansoni & S.
japonicum.
The ovum is passed in the urine or faeces
of the infected individual and gains an
access to fresh where the ciliated
miracidium iside it will be liberated into
the water where it enter the intermediate
host (( fresh water snail )) in which it
multiply and large number of (( fork –
tailed cercaria )) are liberated to the water
where they can penetrate the skin or the
mucous membrane of the mouth of the
human.
They transform into
SCHISTOSOMUTAE and pass through
the lungs and by the blood stream to the
liver and so to the portal vein where they
mature. Within 4 – 6 weeks, adult worms
migrate to the venules draining the pelvic
viscera where the females deposit ova.
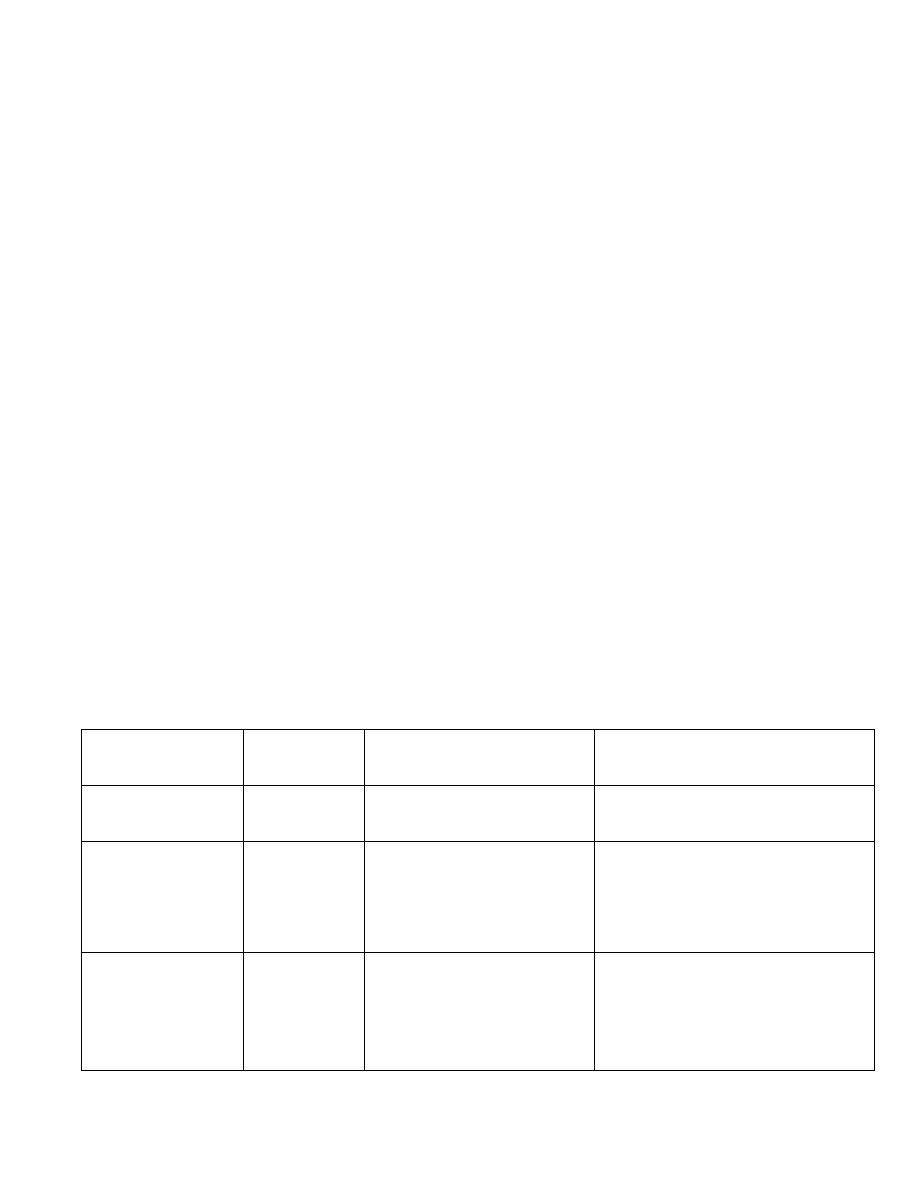
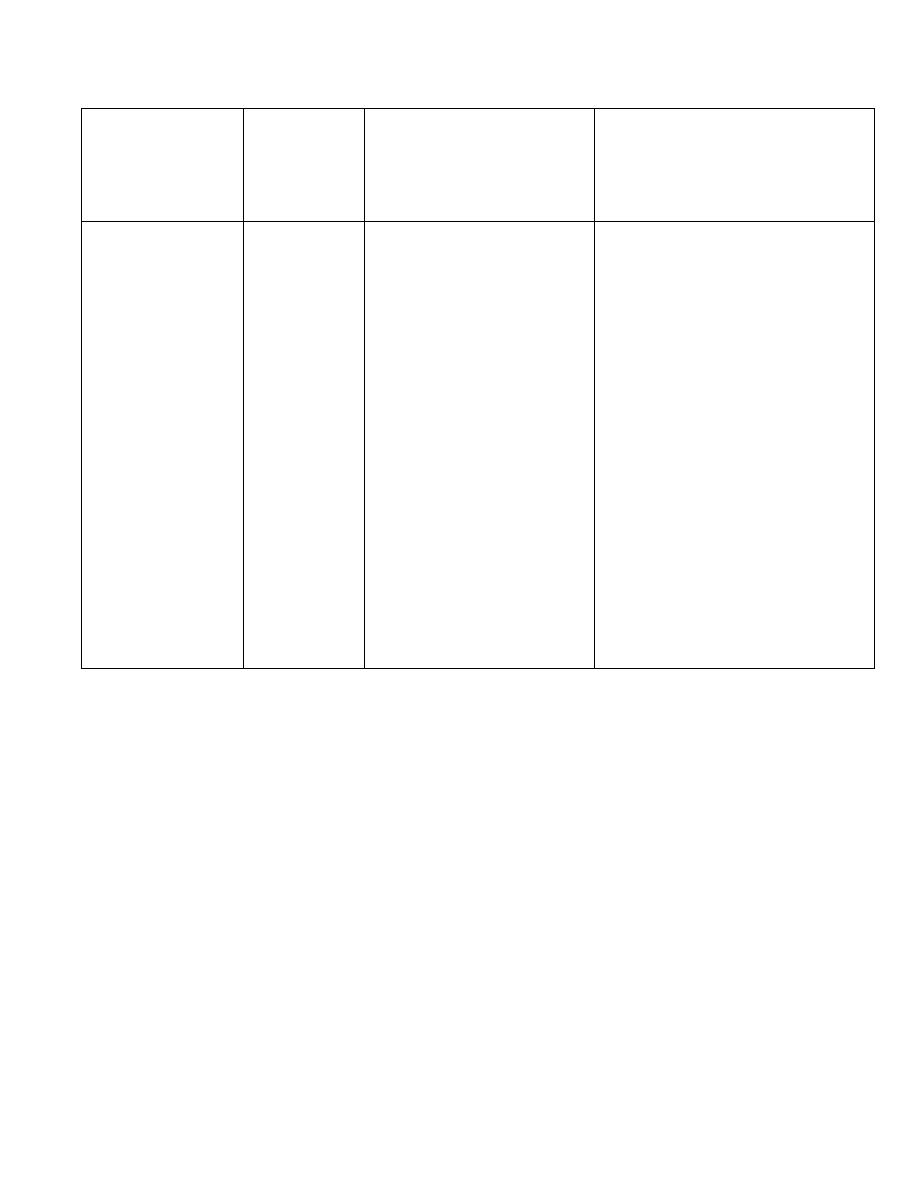
PATHOGENESIS
stage
time
S. haematobium
S. mansoni
S. japanicum
Cercarial
penetration
days
Papular dermatitis at
site of penetration
As for S. haematobium
Larval
migration &
maturation
weeks
Pneumonitis,
myositis, hepatitis,
fever, eosinophilia &
seroconversion
As for S. haematobium
Early egg
deposition
months
Cystitis,
haematuria
ectopic
granuloma in
Colitis
Hepatitis
Portal hypertension
Ectopic granuloma
the skin,
CNS,…
Immune
complex GN
GN
Late egg
deposition
years
Fibrosis &
calcification
of ureters and
bladder
Bacterial
infection
Calculi
Hydronephros
is
Carcinoma
Pulmonary
granuloma &
pulmonary
hypertension
Colonic
polyposis &
stricture
Periportal
fibrosis
Portal
hypertension
Pulmonary
granuloma &
pulmonary
hypertension
CLINICAL FEATURES
Itching lasting 1 – 2 days at the site of
cercarial penetration.
After symptom free – period of 3 – 5
weeks, acute Schistosomiasis ((
Katayama syndrome )) such as
urticaria, fever, muscle aches,
abdominal pain, headache, cough,

sweating, hepatosplenomegaly,
lymphadenopathy and pneumonia
may be present and there is
eosinophelia
Katayama syndrome seen in severe
S.mansoni and S. japanicum but rare
in S. haematobium.
Acute Schistosomiasis subside after 1
– 2 weeks.
Chronic Schistosomiasis due to egg
deposition depend upon the intensity
of the infection and the species.
S. haematobium
Painless terminal haematuria
Frequency due to bladder
calcification
Frequent UTI
Bladder or ureteric stone formation
Hydronephrosis
Renal impairment & renal failure
with contracted calcified bladder
Loin pain radiated to the groin

Haemospermia
Intestinal symptoms may follow
bowel wall involemant
Strong association with squamous
cell carcinoma of the bladder.
S. mansoni
Variable symptoms from malaise,
abdominal pain, frequent blood –
stained diarrhea & rectal polyps
Portal hypertension may cause
massive splenomegaly
Fatal haematemesis from
esophageal varices or progressive
ascites.
Liver function is initially
preserved because the pathology is
fibrotic rather than cirrhotic.
S. mansoni infection predispose to
the carriage of salmonella.
S. japanicum
The adult worm infect human, dogs,
rats, cats, pigs & sheeps.

The pathology is similar to that of S.
mansoni but but it produces more eggs
and extensive & wide spread lesions
The clinical features resemble severe
infection with S. mansoni with added
neurological features.
Small as well as the large bowel may be
affected.
INVESTIGATIONS:
Demonistration of eggs or serological
evidence of the infection.
S. haematobium → terminal spined
egg.
S. mansoni → lateral spined egg.
S. japanicum → lateral rudimentary
spined egg.
Ultrasonagraphy may shows bladder
wall thickening and calicification
with or without hydronephrosis.
Cystoscopy may shows sandy
patches, bleeding mucosa & later
distortion.

Sigmoidoscopy may shows
inflammation and bleeding with
biopsy for ova in S. mansoni and S.
japanicum.
Eosinophelia.
Serology via ELISA as a screening
test.
TREATMANT:
Praziquantel 40 mg/kg once is the
drug of choice for all forms of
Schistosomiasis produce 80% cure
& 90% reduction in egg counts in
the remaining.
S/E nausea and abdominal pain
Oxamniquine is useful and safe in
chronic hepatic forms of S. mansoni
Surgery may be required for
residual lesions.
Plastic surgery for uretric stricture
and fibrotic lesions
Removal of rectal papilloma by
diathermy.

PREVENTION:
1.the life cycle is terminated if the
ova in urine or faeces are not
allowed to contaminate fresh
water containing the snail host.
2.mass treatment of the
population.
3.attack on the intermediate host
(( the snail ))
CESTODES (( TAPEWORMS ))
they inhibit intestinal tract
they have no alimentary
system and absorb nutrient
through there surface.
The anterior surface ((
scolex )) has suckers for
attachment to the host. From
the scolex, a series of
progressively developing
segments are arises.
Larvae are librated from
ingested ova.

Human acquired the
infection by eating
undercooked beef infected
with cysticercus bovis (( the
larval stage of Taenia
Saginata – beef tapeworm-
)).
Undercooked pork
containing larval stage of T.
Solium (( pork tapeworm))
Undercooked fresh water
fish containg larva of
Diphillobothrium latum ((
fish tapeworm ))
Usually only one adult
tapeworm is present in the
gut but up to ten have been
detected.
TAENIA SAGINATA
Adult worm may be several
meters length and produce little or
no intestinal upset in human
being.

Ova may be found in the stool
which is indistinguishable fro T.
solium ova.
Praziquantel is the drug of choice
Niclosamide is an alternative.
Prevention depend on efficient
meat inspection and through
good cooking of beef
TAENIA SOLIUM
It is not as large as T.
saginata.
The adult worm is found only
in human following the eating
of undercooked pork
containing cysticerci
CYSTICERCOSIS:
It is acquired by ingestion
of tapeworm ova from
contaminated fingers or by
eating contaminated food.
The larvae are librated from
eggs in the stomach and

then penetrate the intestinal
mucosa and carried to
many parts of the body
where they developed and
form CYSTISERCI ( 0.5 –
1 cm cysts that contain the
head of a young worm ).
They do not grow or
migrate & located in
subcutaneous tissues,
skeletal muscles and brain.
CLINICAL FEATURES:
Cysts can be palpated under
the skin or mucosa, they
may cause few or no
symptoms and will die &
become calcified.
Heavy brain infection may
cause features of
encephalitis
Cerebral signs do not occur
until the larvae die, 5 – 20
years later in form of

epilepsy or personality
disorders.
Abnormal gait or signs of
internal hydrocephalus.
INVESTIGATIONS
1.calcified cyst can be
recognized
radiologicaly
2.brain CT or MRI are
more sensitive
3.epileptic fit starting in
adult life in endemic
area suggest the
diagnosis
4.antibody detection by
IFAT
TREATMANT
intestinal infection ; Niclosamide
followed by mild laxative
for cerebral cystisercosis,
praziquantel improve prognosis
albendazole for parenchymal
neurocystisercosis

prednisolone given 1 day before
praziquantel or allbendazole
antiepileptic drugs should be given
surgery for hydrocephalus
ECHINOCOCCUS GRANULOSUS
TAENIA ECHINOCOCCUS
HYDATID DISEASE
dogs are the definitive host
the larval stage ( hydatid cyst ) normally occurs
in sheep, cattle, camels and other animals.
By handling the dog or drinking contaminated
water, human may ingest the eggs & the embryo
will liberated in the small intestine and then to
the blood stream and then to the liver.
The resultant cyst will grow very slowly & it
may be calcified or rupture giving rise to
multiple cysts.
CLINICAL FEATURES
It typically acquired during childhood
Usually symptomless.
It may cause pressure symptoms

In 75% of patients with hydatid disease, the
right lobe of the liver is involved and contain
a single cyst.
In the others single or multiple cysts may be
found in the lungs, liver, bone, brain or
elsewhere.
INVESTIGATIONS:
Clinical
Radiological
Ultrasound finding
Complement fixation
ELISA
TREATMANT:
1.hydatid cyst should be excised wherever
possible.
2.albendazole 400mg/12hr for 3 months used for
inoperable or multiple cysts and to reduce the
infectivity of the cyst preoperatively.
3.praziquantel 20 mg/ kg/12hr. for 14 days kill
protoscolices perioperativly.
GOOD LUCK

GOOD BYE