
1
Female genital tract:-
L1
Vulva:-
I. Inflammatory condition ( vulvitis )
There are 2 types of vulval infections which are:-
1- Non-specific infections:
by non-specific microbes which induced severe itching.
2- Specific infections:
which are related to sexually transmitted diseases.
The two most important of these infectious agents are:
a- HPV
infection producing condylomata acuminate and vulvar intraepithelial
neoplasia.
b- HSV
causing vesicular eruption.
Bartholin cysts:
It's a common disorder occur in vulva due to obstruction of the
excretory ducts of the glands.
II. Condylomas:
Which are anogenital warts, it's divided into 2 types:
1- Condylomata lata:
caused by secondary syphilis and rarely seen today.
2- Condylomata acuminata:
which is more common caused by HPV type (6 and 11)
appears as papillary and elevated lesion, singly but more often in multiple sites.
Microscopically
appear in epidermal layer as perinuclear cytoplasmic vacuolization
and nuclear angular pleomorphism.

2
III-Carcinoma of vulva and vulvar intraepithelial neoplasia.
90% of carcinoma of vulva is SCC, the remainder are adenocarcinoma, melanoma or
BCC.
It occurs usually in young age women 40-60 years old.
There are 2 biological forms of vulvar carcinoma, the
1
st
type
occur in young age
group and associated with HPV infection especially type 16 and 18 and preceded by
vaginal , cervical carcinoma , carcinoma in situ or condylomata acuminata.
The vulvar intraepithelial neoplasia VIN usually graded according to its layer into
grade I, II and III or called carcinomain situ, this condition remain many years or
decades then develop invasive carcinoma by genetic, environmental factor as
cigarette smoking or HPV infection.
2
nd
type
occur in older age group, it's seen not associated with HPV infection.
Morphology:
Gossly:
VIN and early vulvar carcinoma appear as areas of leukoplakia, then
transformed into exophytic or ulcerative endophytic tumors.
Microscopically:
HPV+ve neoplasms tend to be multifocal and poorly differentiated
SCC, while HPV-ve lesions which are usually unifocal and well diffentiated keratinizing
SCC, direct spread with deep invasion and regional LN involvement occur.
Vagina:
Inflammatory conditions ( Vaginitis )
It's a common disorder producing vaginal discharge (leukorrhea), it's caused by
bacteria, fungi and parasites.
The most common examples of fungi is
Candida albicans (monilia)
produced white discharge, this organism present in about
5% of normal adults but appearance of symptomatic infection occur in lowering of
immunity as in diabetic patients or sexually transmission of new aggressive strain.
T. vaginalis
is example of parasitic infection produce watery, copious, grey-green
discharge.
Tumors:-
Vaginal intraepithelial neoplasia and SCC.
3
These are uncommon lesions that usually occur in women over the age of 60, usually
is preexisting or concurrent carcinoma of the cervix or vulva is present, however
presence of HPV infection as a caucative agent is not well known but concurrence of
this neoplasia with cervix and vulva suggest a common probably viral infection.
Other rare neoplasm of vagina is sarcoma botryoides (embryonal rhabdomyosarcoma
) occur usually in infants and children under the age of 5 years, it appear as soft
polypoid masses.
Cervix:-
Cervicitis
Inflammation of cervix are common disorder and associated with mucopurulent
vaginal discharge.
The infectious cervicitis is caused by variable specific and non specific microorganisms
many of these microorganisms are transmitted sexually, the most important
pathogen are C. trachomatis, herpetic infection and HPV.
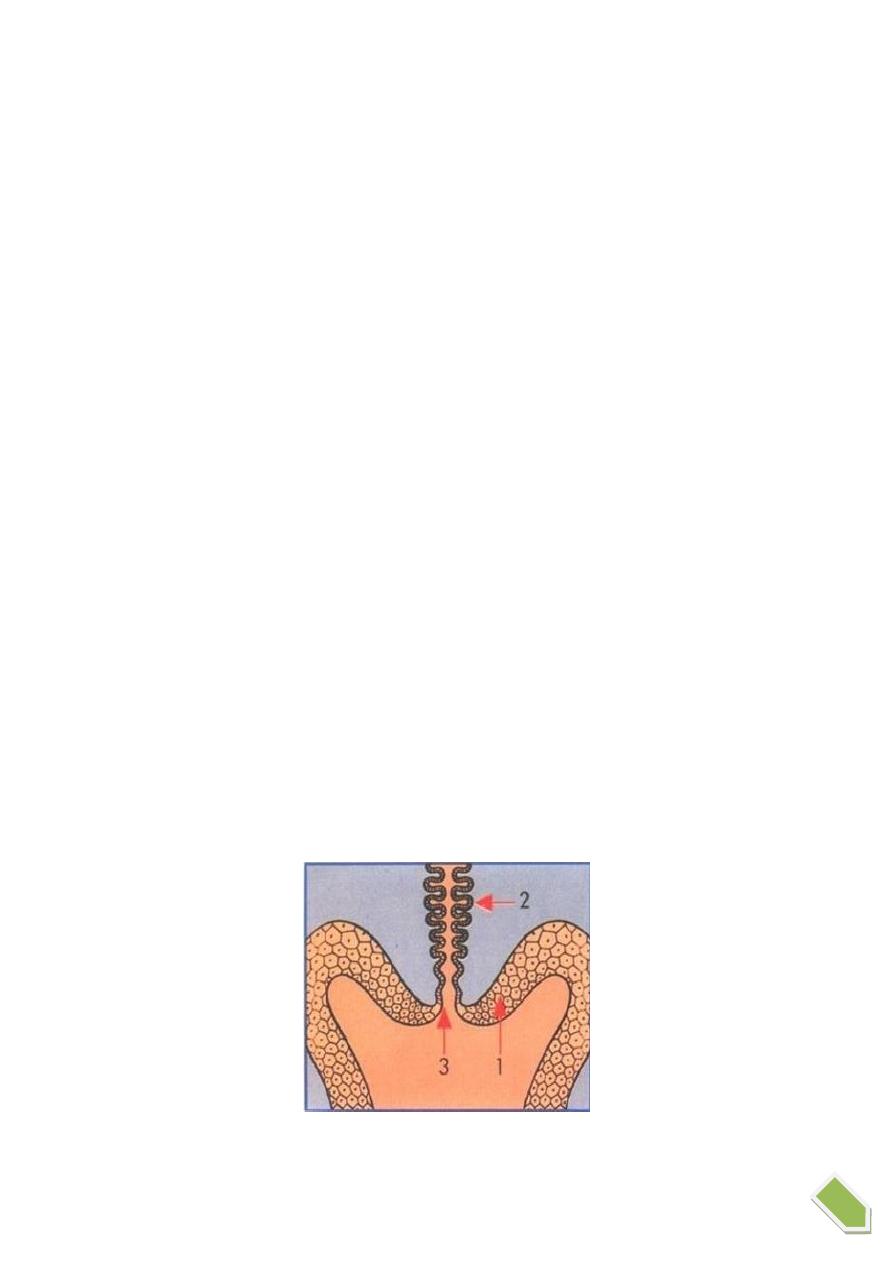
We must differetaite true inflammatory cervicitis from so called "erosions", during
development the columnar mucus secreting epithelium of the endocervix meets the
squamous epithelial of ectocervix at the external os, in young women there's down-
growth of the columnar epithelium below the ectocervical os-ectropian so
squamocolumnar junction lie below exocervix, this exposed mucus-secreting
columnar epithelium may appear reddened and moist and is mistakenly called
cervical "erosion" but in elderly there's regrowth of the squamous epithelium up to
the original external os. The area replaced by the squamous epithelium is known as
the "transformation zone"
4
Tumors:-
Endocervical polyp:
It appear as soft glistening polypoid mass protrude from endocervix and it's
inflammatory in origin.
Microscopically:
the lining epithelium of polyp and lining of glands consist of mucous
secreting columnar epithelium, the stroma is oedematous and infiltrated by scattered
mononuclear cells.
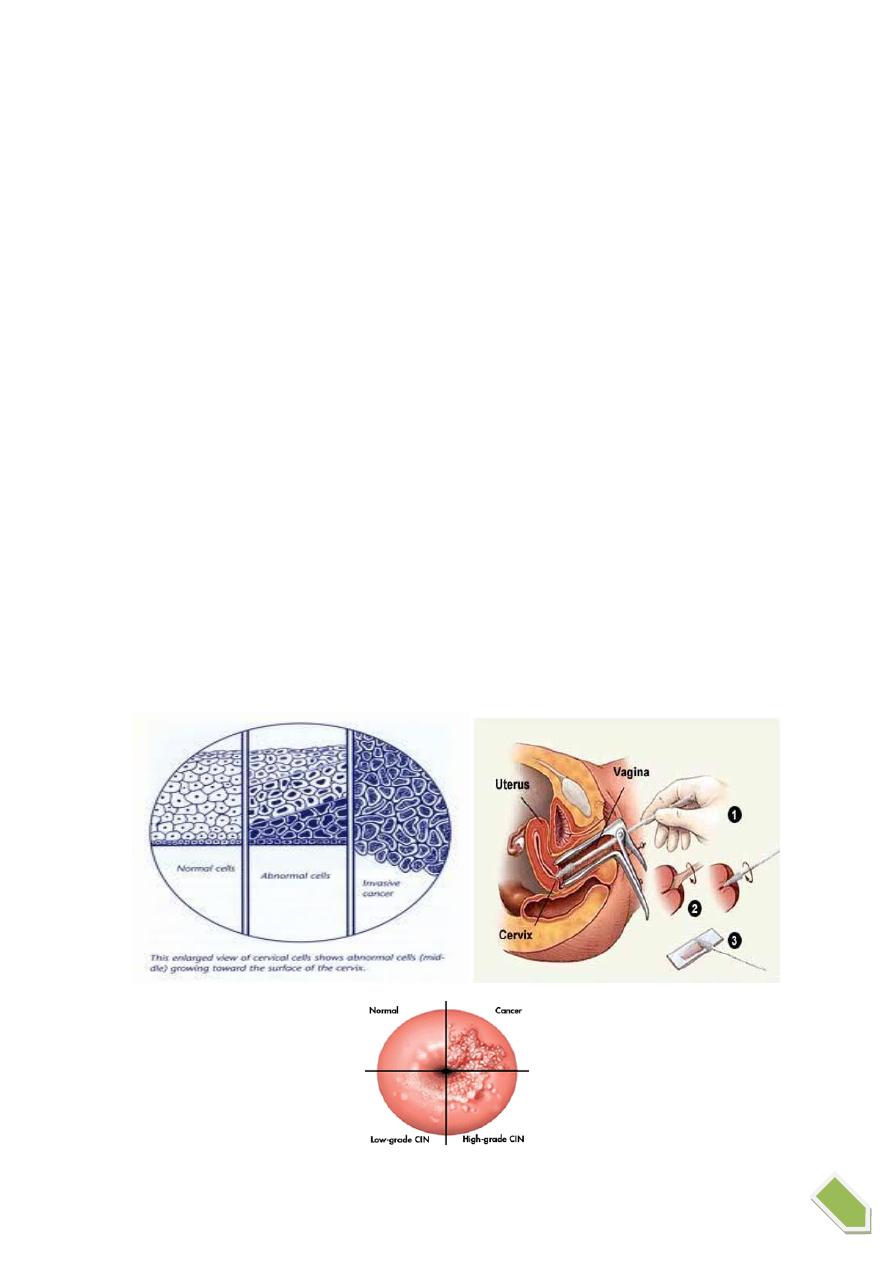
Cervical intraepithelial neoplasia (CIN) and squamous cell carcinoma.
Wide spread of papanicolaou (cytological) screening or pap smear has dramatically
lowered the incidence of invasive tumor, because most or all of invasive cervical
squamous cell carcinomas arise from precursor epithelial changes (CIN) but not all
cases of CIN progress to invasive cancer, it may be regress, that's the precancerous
epithelial changes (CIN) may precede the development of cancer by many years, so
cellular atypia of squamous lining epithelium it's divided into 3 grades:
CIN grade I: Mild dysplasia.
CIN grade II: Moderate dysplasia.
CIN grade III: Severe dysplasia and carcinoma in situ and this according to level of
dysplatic changes.

5
Pathogenesis:-
The prominent risk factors for the development of CIN and invasive carcinoma are:
1- Early age at first intercourse.
2- Multiple sexual partners.
3- A male partner with multiple previous sexual partners.
4- Higher incidence in lower socioeconomic groups.
HPV infection can be detected in higher percentage of precancerous lesions and
invasive neoplasms, especially type 16 and 18 in these lesions viral DNA integrate into
the cellular genome and endcode proteins that block or inactivate tumor suppressor
genes P53 and Rb in target epithelial cells and this causing uncontrolled proliferations
of cells.
However not all women infect by this virus develop SCC but this need another
carcinogens as lowering immunity or cigarette smoking.
Invasive carcinoma of the cervix:-
SCC is most common type of invasive carcinoma of cervix which is form 80-95% of all
cases, other rare form are adenocarcinoma and other types, this is usually arise from
CIN by many years may be reached 10-15 years other cases especially in high grade
CIN may be shorter interval to develop invasive carcinoma.
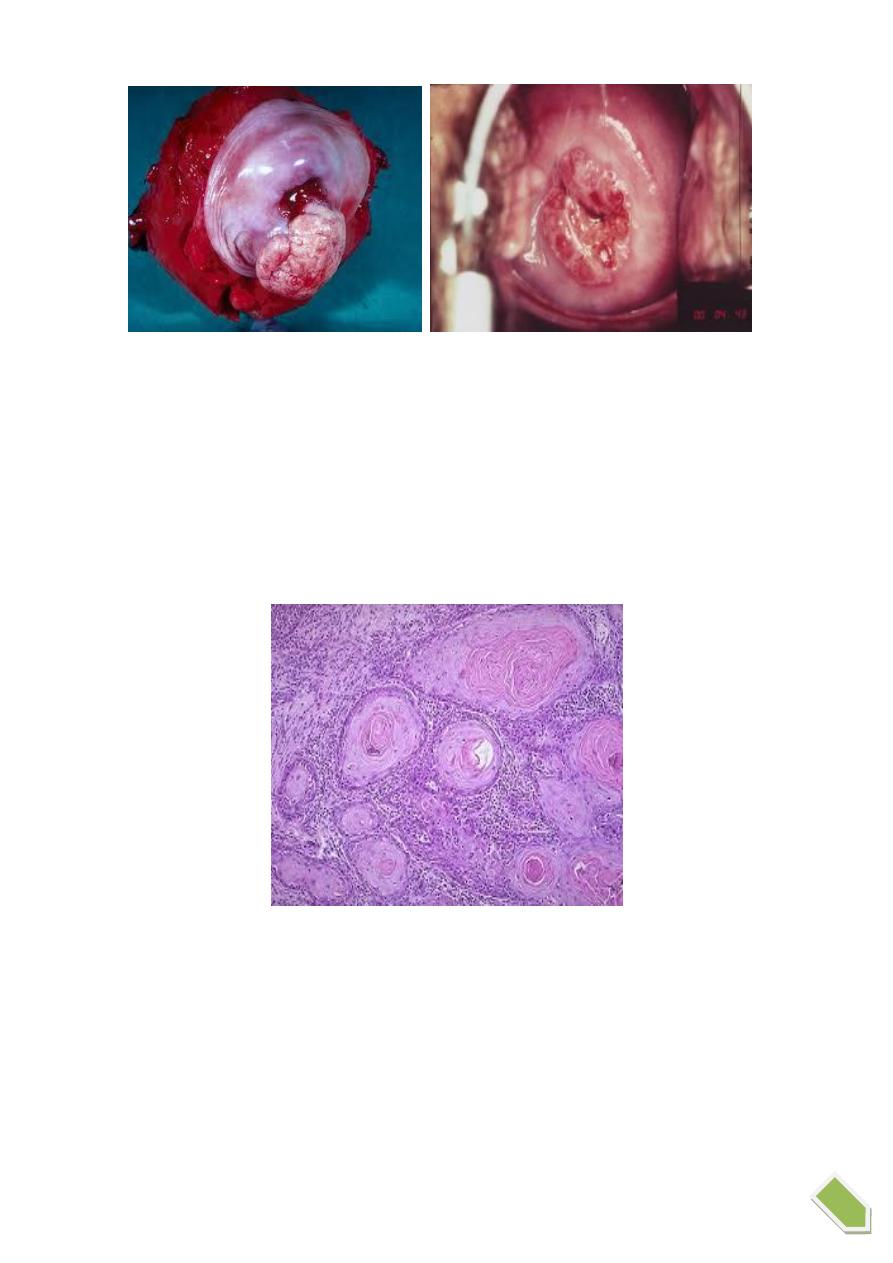
Morphology:-
Grossly:
invasive carcinoma takes one of three forms it's either:
1- Fungating
tumor that may develop to cauliflower-like mass.
2- Ulcerative
form characterized by sloughing of the central surface of the tumor.
3- Infiltrative
which tend to grow downward to stroma. These tumors usually spread
locally downward and upward to uterus, broad ligament, rectum, base of bladder and
even the ureters. Then with progress can spread by LN or hematogenous distant
metastasis.
6
Histology:
SCC is graded according to differentiation of tumor cells into 3 grades:
Grade I: in well differentiated keratinizing type.
Grade II: in moderately differentiated type.
Grade III: in poorly differentiated type.
While staging system according to its dissemination.