DISEASES OF THE PLEURA & CHEST WALL
DrABDUL HAMEED AL QASEER
Pleurisy
Pleurisy is a term used to describe pain resulting from any disease involving the pleuraIt is common due pulmonary infection & infarction , also in malignancy , rare causes include rheumatoid arthritis & SLE .
The pain is sharp that aggravated by deep breath or coughing & pleural rub may be heard on the affected side .
Loss of a pleural rub & diminution of pain indicate either recovery or the development of a pleural effusion .
CXR should be done , but a normal x-ray does not exclude pleurisy .
Epidemic myalgia ( Bornholm disease ) is due to infection by Coxsackie B virus .it is common in young adults in the late summer& autumn , characterized by URTI followed by pleural pain &upper abdominal pain with tenderness. CXR is normal & the illness clear within a week .The management to treat the primary cause & the pain need good analgesics .
PLEURAL EFFUSION
Pleural effusion is the accumulation of serous fluid within the pleural space.Empyema is the accumulation of pus in the pleural space.
Hemothorax is the accumulation of blood in the space.
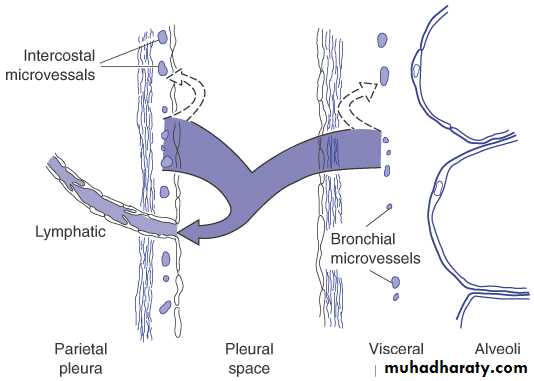
PLEURAL CIRCULATION
0.01ml / kg / hrs0.2ml / kg /hrs
Mechanisms of Pleural Fluid Accumulation
Hydrostatic pressureOncotic pressure
Pressure in the pleural cavity
Permeability in the microvasculatory circulation
Lymphatic drainage
Passage from abdomen
Causes of Pleural effusion
Other causesClinical assessment
Breathlessness is the only symptom related to the effusion itself , and the severity depend on the amount of fluid .Symptoms of pleurisy ( pleuritic chest pain) &/or pleural rub often precede the development of an effusion .
Feature of the primary cause may accompanied or masked the feature of effusion .
what are the physical finding ?
Decrease chest expansion .
Tracheal shift to other side ( large effusion) .
Stony dullness on percussion .
On auscultation , absent breath sound & vocal resonance .
Crackles above large effusion .
Investigation
CXR : 200 ml of fluid is required to be detectable on PA chest X-ray .Curved shadow at lung base .
Blunting the costophrenic angle.
The finding simulate an elevated hemidiaphragm
Fluid in the oblique fissure may produce a rounded opacity.
Ultrasonography is more accurate than CXR .
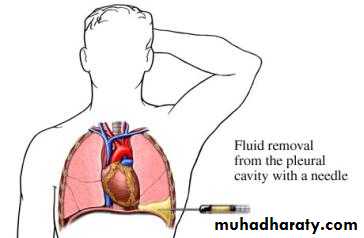
Pleural aspiration
At least 50 ml of fluid should be aspirated .The sample examined for protein, LDH , cytology , WBC & the differential counts , & bacterial including Z-N stain /auramine stain ,& culture for TB .
Other like glucose , cholesterol , amylase ….
In TB pleural effusion adenosine deaminase >40 iu/L or interferon – gamma > 140 pg /ml can be diagnostic .
Light`s Criteria Pleural fluid is an exudate if one or more of the following criteria are met:
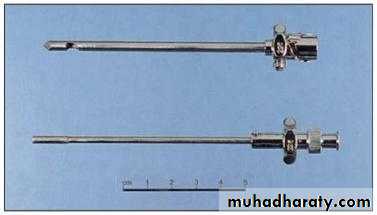
pleural biopsy
It is helpful for the diagnosis of malignant pleural effusion & TB effusion .Needle Biopsy of Pleura

Prospective randomised trial of ‘blind’ Abrams’ pleural biopsy vs CT guided cutting needle pleural biopsy in cytology negative undiagnosed pleural effusions. Maskell NA et al. Lancet 2003
• Abrams’sensitivity 47%, specificity 100%, negative predictive value 44%, positive predictive value 100%
• CT-guided biopsy sensitivity 87%, specificity 100%, negative predictive value 80%, positive predictive value 100%;
• difference in sensitivity between Abrams' and CT-guided 40%, 95% CI 10-69, p=0.02).
• CT guided pleural biopsy is more effective including MPM
• Prefere in cytology negative cases
CT guided cutting needle biyopsi
Thoracoscopy in the diagnosis of pleural effusion
(>90%) can diagnose malignancy including MPM(>95%) can diagnose TB
Rarely useful in diagnosing other bening diseases
Pleurodesis can be performed
Pleural abration or tetracycline

localized pleural effusion
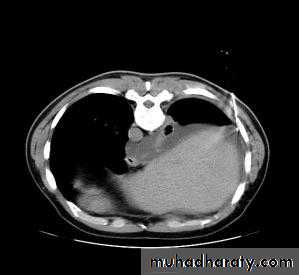
CT SCAN OF THE CHESTThoracentesis
If clinical and radiological diagnosis is not possibleDefinitive contrendication?
Relative contrendication
Bleeding diathesis
Anticoagulant therapySmall efusion
Mechanical ventilation
Single lung
Differential Cell Count
Neutrophil
Acute process
Mononucleated cells
Chronic process
Small lymphocyts
malignant, tuberculosis or post cabg pleural effusion
Eosinophil (>%10)
Air-blood
drugs
Asbest pleural effusion
Churg -Strauss syndrome
Frequently undefined
Separating Transudates and Exudates: Light’s criteria
Protein: pleural fluid/serum > 0.5LDH: pleural fluid/serum > 0.6
LDH: pleural fluid > 2/3 of upper normal for serum
occasionally misidentify transudate as exudate
Numerous other molecules/criteria been suggested
Light’s criteria are gold standard
Empyema
Empyema is a collection of pus in the pleural space.
The pus may be as thin as serous fluid or so thick that it is difficult to aspirate even through a wide – bore needle.
Empyema is always secondary to infection to neighboring structures ,usually the lung ,most commonly bacteria & TB .
Other causes are infected hemothorax , esophageal rupture or rupture of subphrenic abscess.
Clinical features of empyema
Pleural pain; breathlessness; cough and sputum usually because of underlying lung disease; copious purulent sputum if empyema ruptures into a bronchus (bronchopleural fistula)Clinical signs of pleural effusion
Aspiration of fluid
If fluid is thick & turbid pus , empyema is confirmed.Other features suggesting empyema :
- a fluid glucose < 3.3 mmol/L ( 60 mg/dl)
- LDH > 1000 U/L
- fluid PH < 7.0 ( H > 100 nmol/L
The distinction between TB & bacterial causes can be difficult & often requires pleural biopsy, & culture .
Treatment of empyema
Empiric antibiotic treatment ( e.g. I.V. co- amoxiclav or cefuroxime with metronidazole) can be started & when the microorganism is known the appropriated antibiotic should be given for 2-4 weeks .If the cause is TB , anti TB chemotherapy & pus in the pleural space aspirated through a wide –bore needle until it ceases to reacumulate .
Surgery may be needed in may occasions .
PNEUMOTHORAX
Pneumothorax is the presence of gas(air) in the pleural space .
Spontaneous pneumothorax is occur without trauma to the chest .
Primary spontaneous pneumothorax occur without underlying lung disease .
Secondary spontaneous pneumothorax occur due any lung disease most common in COPD .
Types of spontaneous pneumothorax
Tension pneumothoraxTension pneumothorax (TP)
Patient with TP presented with rapidly progressive dyspnea associated with a marked tachycardia , hypotension , cyanosis & tracheal shift away from the affected side .Physical examination: absent of breath sound , no chest expansion , & hyperresonant on percussion .
Tension pneumothorax must be treated as a medical emergency .
A large –bore needle should be inserted into the pleural space through the second anterior intercostal space .If large amounts of gas escape from the needle after interior , the diagnosis is confirmed.
The needle should be left in place until a thoracotomy tube can be inserted .
Simple aspiration of pneumothorax
Tension pneumothorax