Lecture (1) ENT Dr. Haitham Alnori
30 /3/ 2017Inner Ear
Otosclerosis
Deafness (SNHL)
Sudden hearing loss
Ototoxic drugs
Presbyacusis
Acoustic trauma
Vertigo
BPPV
Menier's disease
Vestibular neuronitis
Tinnitus
Vestibular schwannoma( acoustic neuroma)
Deafness (Hearing Loss)
I. ConductiveA. Congenital: congenital meatal atresia.
B. Acquired
1. External ear: impacted wax, foreign bodies and squamous cell carcinoma.
2. Middle ear:
a. Trauma: TM perforation & ossicular disconnection.
b. Inflammatory: chronic supp. otitis media, secretory otitis media.
d. Tumours: glomus jugulari.
3. Otic capsule: otosclerosis.
II. Sensorineural Hearing Loss. It has two types:
Sensory (cochlear) hearing loss= cochlear lesion.
Neural (retrocochlear) hearing loss= auditory nerve lesion, spiral ganglion and its connections.
A. Congenital:
a. Intrauterine infections: rubella, syphilis & toxoplasmosis.
b. Toxins: hypoxia and kernicterus.
B. Acquired:
Traumatic: head injury and blast injury.
Infective; Labyrinthitis, measles (bilateral deafness), mumps(unilateral deafness) syphilis, meningitis
Meniere's disease.
Ototoxic drugs.
Degenerative: pressbyacusis.
Neoplastic: acoustic neuroma.
Sudden Hearing Loss
Sudden hearing loss may be conductive or sensori-neural.Sudden conductive hearing loss may be due to :
Impacted wax.
Traumatic perforation.
Ossicular chain disruption.
Sudden SNHL
Idiopathic: in 2/3 of cases no cause could be found.
Vascular: spasm, thrombosis or hemorrhage of the internal auditory artery.
Viral infection: mumps, measles, rubella or Herpes zoster.
Trauma: Head injury, blast injury, ear surgery as stapedectomy.
Raised intracranial pressure as it occur in straining , coughing and bending down position , these may lead to rupture of round window .
Tumors: Acoustic neuroma (10 % of acoustic neuroma presents as sudden SNHL, that's why MRI is indicated in sudden SNHL).
Clinical Picture of sudden SNHL
Hearing loss: occurs over minutes, hours or days.Tinnitus: good prognostic sign, means that hair cells still functioning.
Vertigo: common in those with vascular aetiology , carries bad prognosis.
Examination
TM is usually normal. Tuning fork test: Rinne test is positive and Weber test is lateralized to the better hearing ear.PTA: Hearing loss in high frequency, sometimes total hearing loss.
Treatment of sudden SNHL
Bed rest is important. Steroids are given in high doses: prednisolone 1-2 mg/kg daily for 5 days. Vasodilators: Betahistine 16 mg tid± breathing 5% CO2 in air (carbogen) to improve the cochlear circulation.
Low molecular weight dextran: to lessen sludging of blood in the small vessels of the cochlea.
Prognosis
In 1/3 of patients there is quick recovery. If there is no recovery within 3 weeks it is unlikely to occur. One third experience partial recovery and a third have none. A severe loss, high frequency loss, absence of tinnitus and the presence of vertigo are unfavorable prognostic features.Drug Ototoxicity
Damage to the cochlear and/or vestibular part of the inner ear by certain drugs:
Aminoglycosides: gentamycin, amikacin, neomycin.
Loop diuretics: frusemide and ethacrynic acid.
Salicylates: transient deafness and tinnitus.
Quinine.
Antiepileptics: phenytoin.
B-blockers.
Cytotoxics: cisplatin.
If two potentially cytotoxic drugs are given at the same time, such as aminoglycosides and diuretics, their toxic effects may be synergistic. The danger are especially great if excretion is impaired as in renal failure.
Clinical Picture
Tinnitus is often the first symptom followed by SNHL at high frequency. Vertigo is less common.Management
Keep the plasma level in a safe range and avoid or discontinue ototoxic drugs whenever there are signs of otoxicity.Presbyacusis (senile Hearing Loss)
Symmetrical Bilateral SNHL which usually occurs after the age of 65 years with no underlying cause. The degenerative changes occur as a result of aging process, vascular insufficiency or noise exposure.
Clinical Picture
Deafness is characteristically progressive, bilateral SNHL with marked loss of speech discrimination due to inability to hear the higher frequencies(consonant sounds).Thus, speech is difficult to be understood
especially if fast, too loud or in a noisy background.
PTA: Bilateral symmetrical SNHL.
Treatment
Lip reading and auditory training.
It is important to speak slowly, distinctly and not to shout with these patients.
Hearing aids: If the hearing loss is greater than 40dB.
Deafness and Noise
Deafness that results from excessive sound stimulation. It is of two types:Acoustic trauma: SNHL due to brief exposure to very loud noise e.g. gunfire and explosions.
Noise-induced hearing loss: SNHL caused by prolonged exposure to loud noise in certain occupations. A noise level in excess of 85 dB for 8 hours/ day is hazardous. Tinnitus is usually a feature.
PTA: The earliest changes of acoustic trauma is SNHL at 4kHz which may be transient(temporary threshold shift). If the condition is repeated, SNHL will affect all frequencies.
Treatment
preventive: by using protective ear plugs and screening personnel in noisyoccupations by routine audiometry.
Therapeutic:
Avoidance of further trauma.
Hearing aids and auditory training.
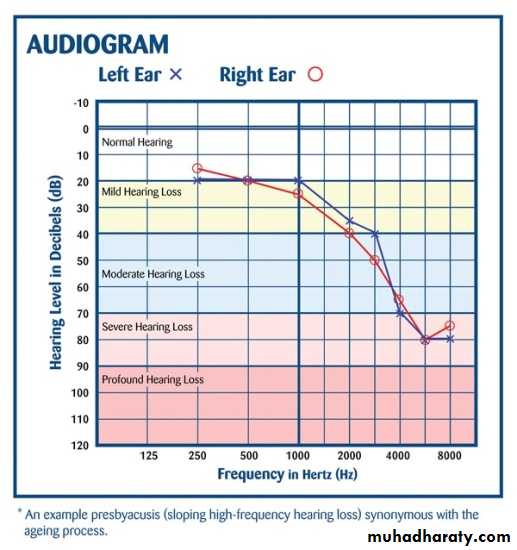
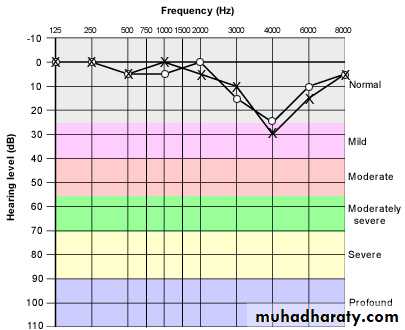
Acoustic Trauma Presbyacusis
Non-Organic Hearing LossIt means deafness without organic cause:
Psychogenic(hysterical): the patient is unaware that he is simulating deafness. The onset is usually due to some severe psychological trauma.
Malingering: the subject is quite aware that his hearing is normal. He pretend deafness to avoid situation of responsibility.
Diagnosis
There is gross discrepancy between history and examination, and between repeated tuning fork tests.Fracture base of skull
Direct or indirect trauma to the petrous bone may cause fracture ( longitudinal or transverse). The longitudinal is more common and is parallel to the long axis of the petrous bone. There may be hemorrhage in the cochlea, vestibule or internal auditory meatus. Microscopic fracture may occur in the otic capsule in case of severe head injury, causing permanent hearing loss.Clinical Features
Severe sensorineural hearing loss, may be permanent.Tinnitus and vertigo may disappear later.
Facial nerve palsy is seen more often in transverse fracture(50%).
Tympanic membrane may be intact with hemotympanum.
Management
Management is not easy because the patient is sometimes severely injured. Negative findings in X-ray does not exclude the diagnosis and CT is preferred.
DO NOT syringe the ear.
DO NOT put instruments inside.
NO caloric test.
Facial nerve palsy: delayed onset, conservative treatment while immediate onset may require surgery in the form of decompression or re-anastomosis.