Pediatric Surgery

Infantile Hypertrophic Pyloric Stenosis(IHPS)
Objectives At the end of this subject you should be able to:1. Define IHPS.2. List the cardinal features and signs of IHPS.3. Determine the investigations and treatment of IHP.
☆ Acquired condition☆Hypertrophy of circular muscles of the pylorus☆ Incidence 1-4 in every 1000 live birth☆ Boys are affected four times more than girls☆ Aetiology is multifactorial☆ Age of presentation is 2-8 weeks of life☆ Rare after 3 month of age
IHPSC/F: 1. Vomiting- Non bilious.- Projectile.- Postprandial.2. Dehydration3. Weight LossO/E:→ visible peristalsis→ olive mass





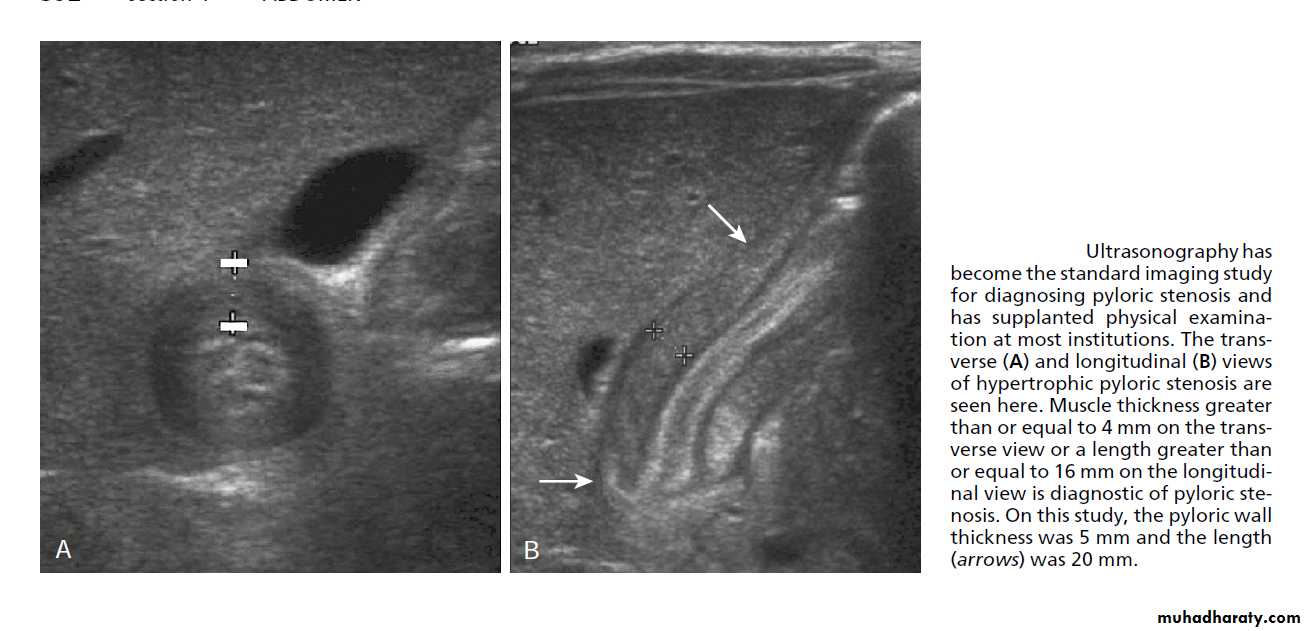
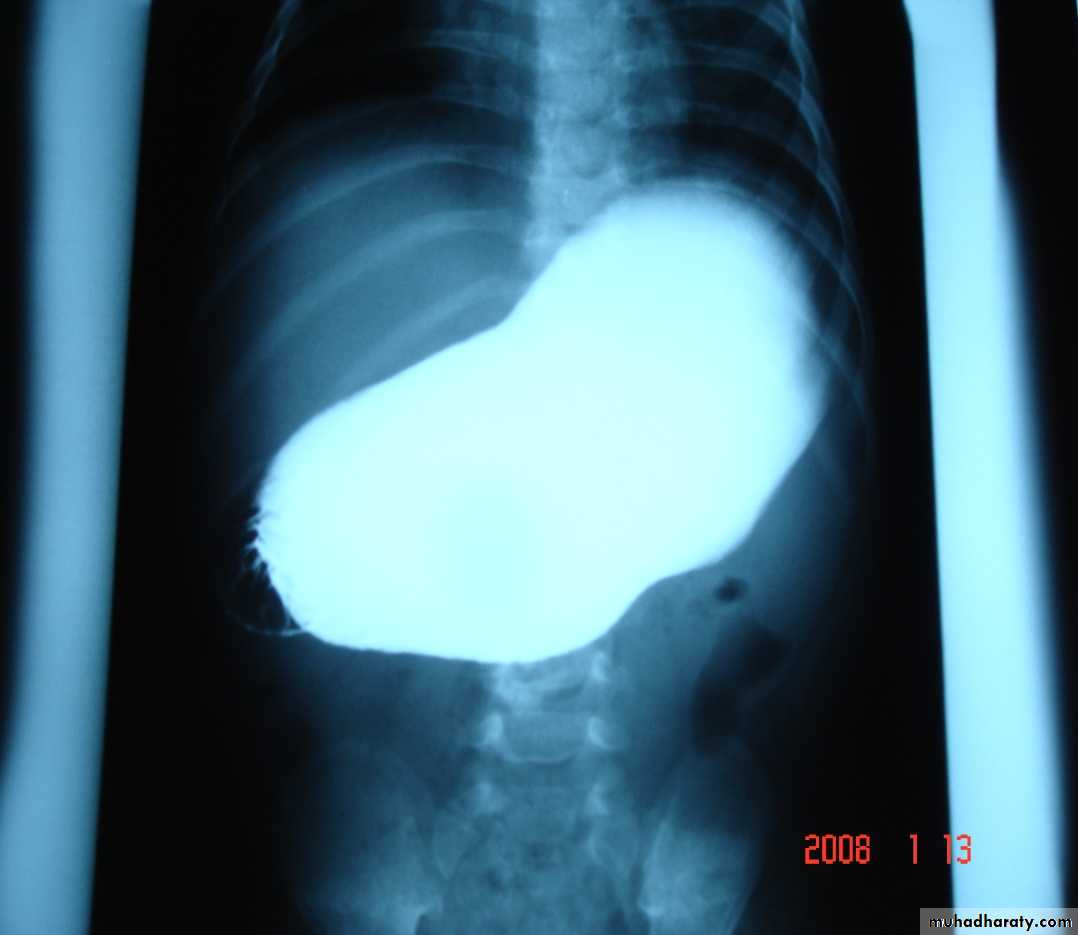
Diagnosis
Clinical US Contrast Olive mass studyFeed test

Treatment★Stop oral feeding with /without NGT★ Correction of hydration state with fluid and electrolytes replacement★ Monitoring of glucose★ 120-150 ml/kg of 0.45% saline + 5% dextrose + 20 meq of K+ per one liter of fluid.★ Surgery is not an emergency
Pyloromyotomy

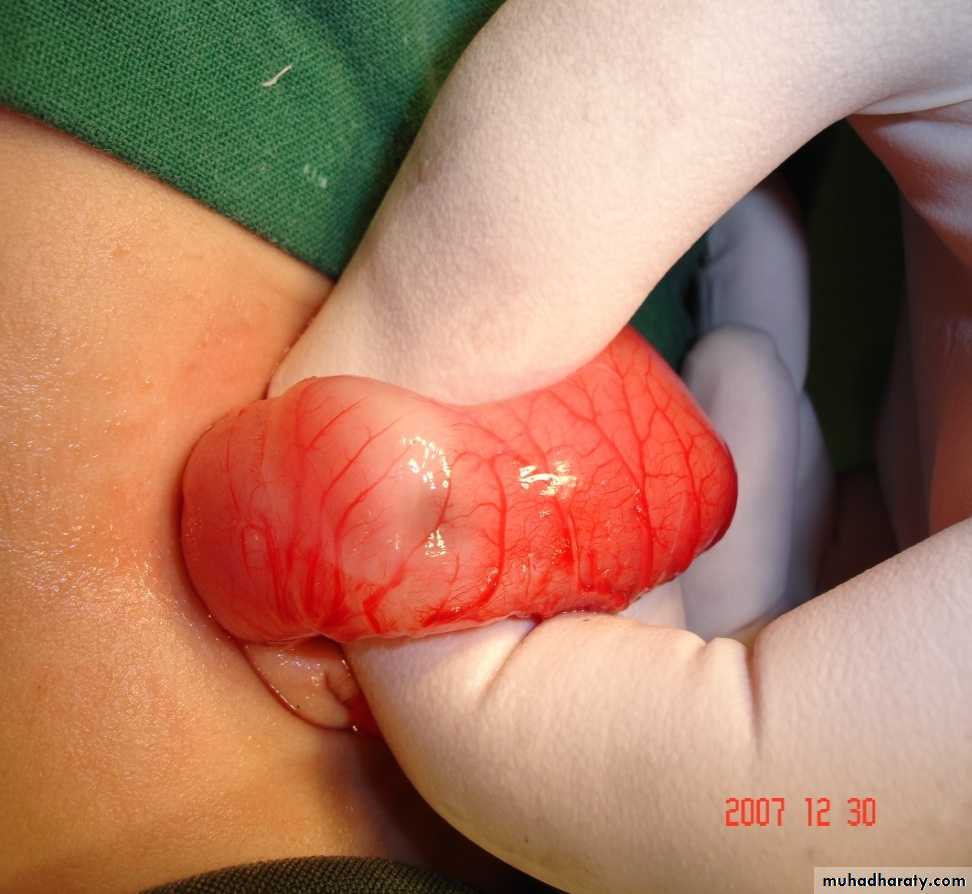
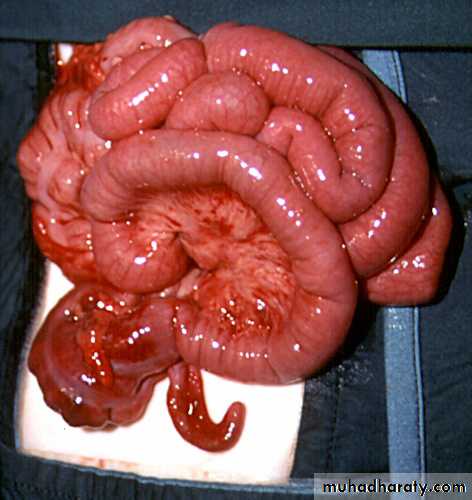
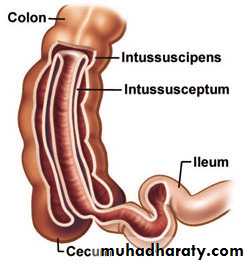
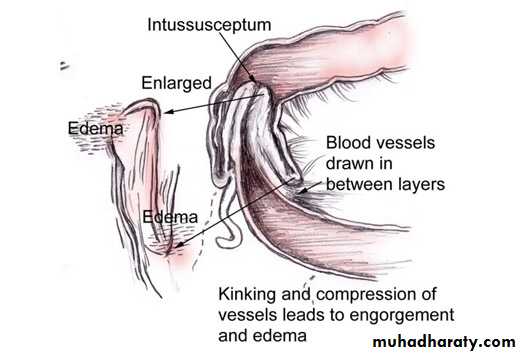
Intussusception
Objectives At the end of this subject you should be able to:1. Define Intussusception.2. Classify the Intussusception.3. List the symptoms and signs of Intussusception.4. Name the investigations used to confirm the diagnosis.5. Itemize the modalities of treatment.
Definition:Types Anatomically Etiology
10% of cases there is a pathological leading point and it occurs more in children more than 2 years of age and in cases with recurrent intussusception.More during attacks of upper respiratory tract infection and gastroenteritis.Age 5-10 monthMore in boys
C/F: 1. Abdominal cramps 2. Vomiting 3. Bowel motion O/E: dehydration abdominal distension palpable abdominal mass



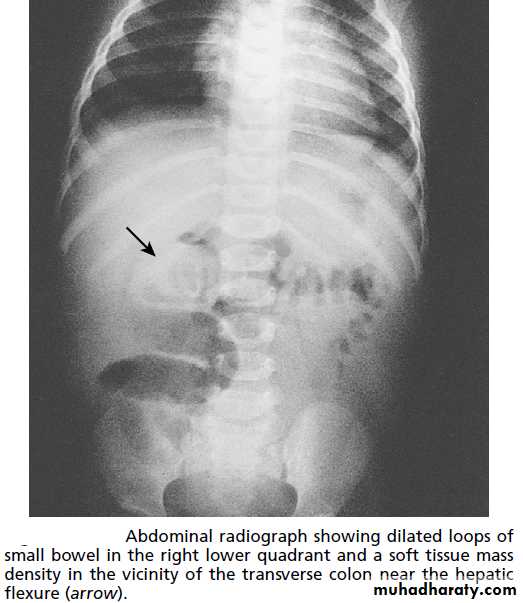
P/R:Dx.1. Plain radiograph


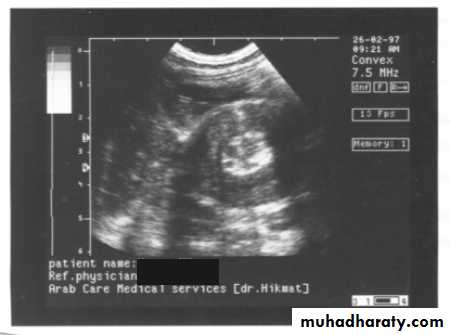
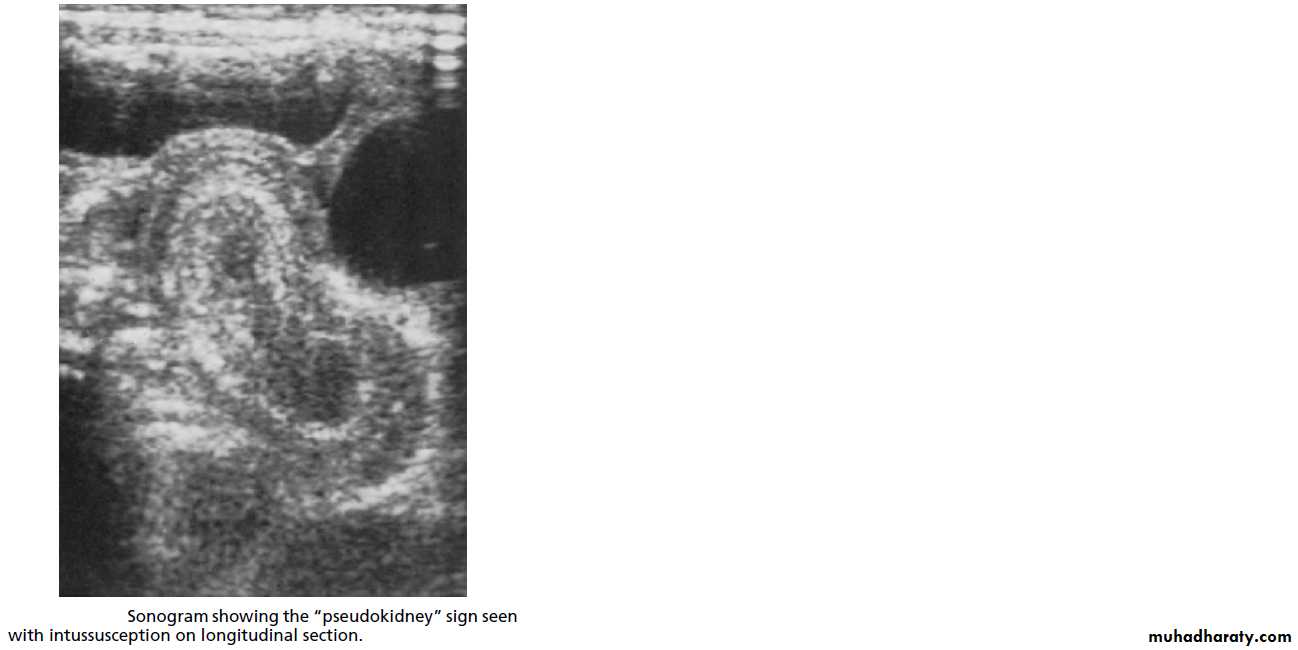
2. US
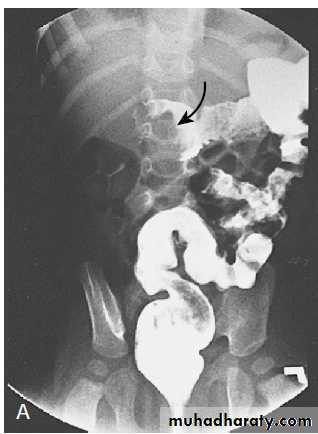
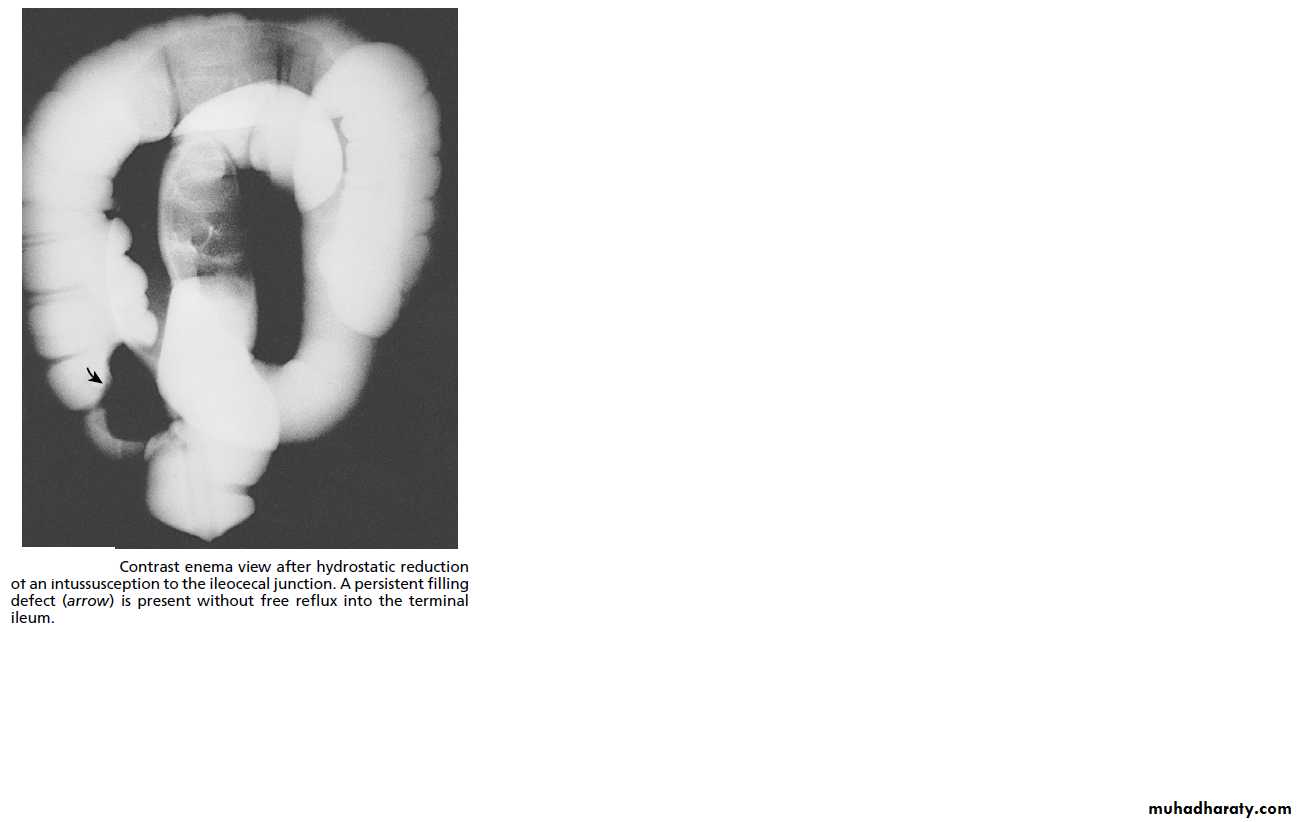
3. Contrast enema


SurgicalIndicationManual reduction Resection with end-end anastomosisAppendicectomy (incidental)


Acute abdominal pain In Children
History and examinationTime and patience.The child is frightened and the parents are worried. Difficult to accurately describe or localise abdominal pain.
Inspect the abdomen thoroughly and reassess after a period of time.The genitalia, chest and neck must also be examined.Rectal examination is not routinely done.
Active observation ?Admit the childReassess after few hoursClear fluid and simple analgesiaReduce the need for investigations and removal of innocent appendix.
Acute non-specific abdominal pain➣ Similar to acute appendicitis differences??➣ Poorly localized➣ not aggravated by movement ➣ gardening (rarely)➣ self limiting symptoms (48 hr)
Acute appendicitisClassical features :Abdominal pain, nausea, anorexia, vomiting, localised tenderness, loose stool (pelvic).Dysuria ?? False?! Sterile pyuria ?Temp. & pulse rate: normal or slightly elevated initially390C and above perforated appendix, abscess formation Not acute appendicitis Examination of chest (Rt. lower lobe pneumonia), tonsils,……etc
Poorly communicated symptomsEasily confused with UTI, GEAbdominal signs are modified with AB (throat or ear infection)Why they develop peritonitis more common?????1. Late presentation and difficult diagnosis.2. More incidence of faecoliths (obstructing type)3. Poorly developed greater omentum.
Rx:1. Resuscitation with i.v fluid, AB, analgesia.2. Surgery which is either open or laparoscopically.Rx of App. Mass & abscess ……………