1
L3
Pathology of Testes
Normal embryology and anatomy
ⱴ The normal adult testis is a paired organ that lies within the scrotum suspended by
the spermatic cord
ⱴ The average weight of each testis is 15 to 19 g,
ⱴ The right usually being 10% heavier than the left.
ⱴ The organ is covered by a capsule composed of three layers the outer serosa or
tunica vaginalis (covered by a flattened layer of mesothelial cells), the tunica
albuginea, and the inner tunica vasculosa.
ⱴ The posterior portion of the capsule, called the mediastinum, contains blood and
lymph vessels, nerves, and the mediastinal portion of the rete testis
ⱴ The parenchyma is divided into approximately 250 lobules,
ⱴ each lobule containing up to four seminiferous
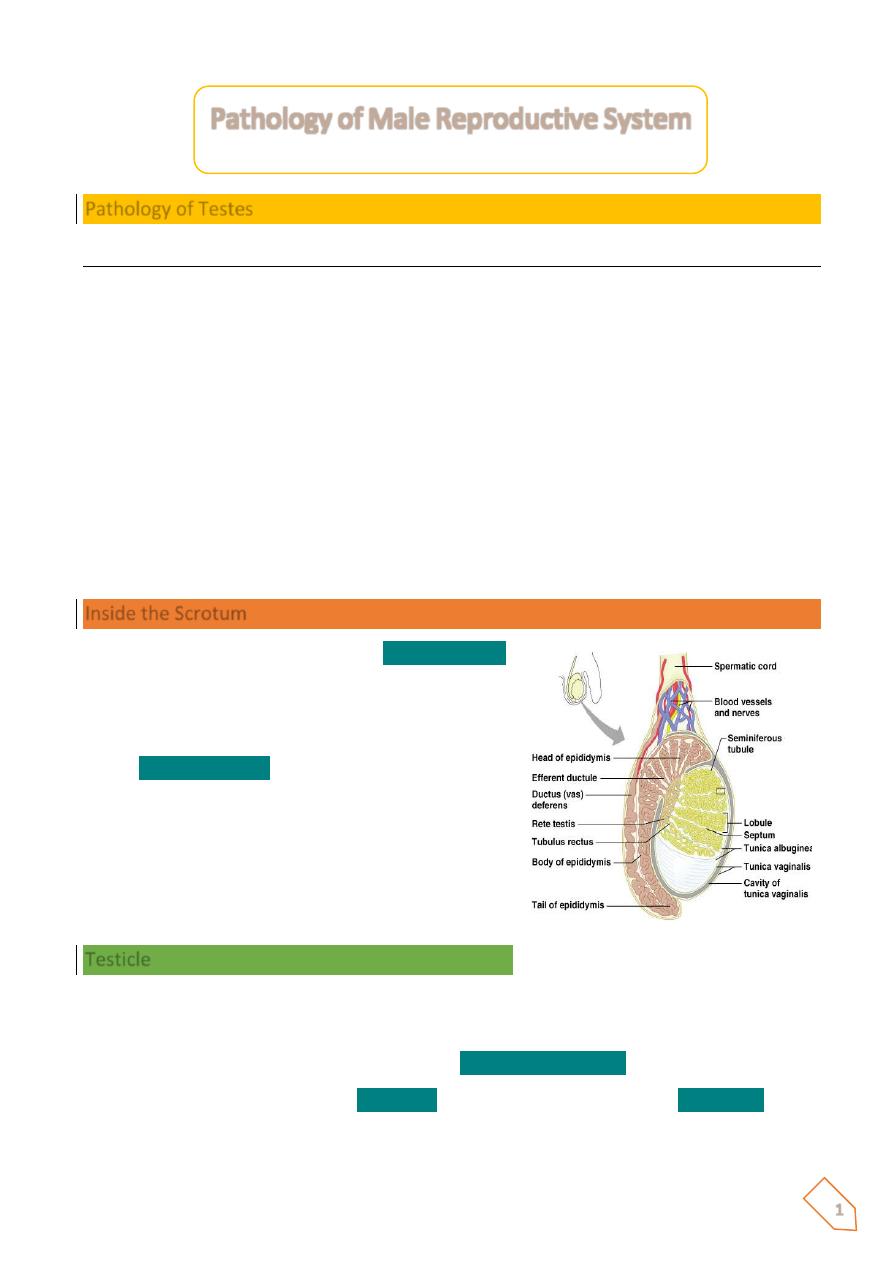
Inside the Scrotum
ⱴ Each testes is enclosed by the
tunica vaginalis
,
a continuation of the peritoneum that lines the
abdominopelvic cavity.
ⱴ A fibrous capsule covers each testis called the
tunica albuginea
.
Testicle
ⱴ The tunica albuginea gives rise to septa (partitions) that divide the testis into lobules
(about 250)
ⱴ Each lobule contains 3 or 4 highly coiled
seminiferous tubules
ⱴ These converge to become
rete testis
which transport sperm to the
epididymis
Pathology of Male Reproductive System
2
Cryptorchidism
ⱴ In one out of every ten males, the testis has not descended into the scrotum at the
time of birth but has remained in the inguinal region or abdomen
ⱴ Most of these "retained" or "retractile" testes descend into the scrotum during the
first year of life
ⱴ In only 1 in 100 individuals will a permanent retention of the testis outside the scrotum
occur a condition known as cryptorchidism
ⱴ The exact pathogenesis is unknown, but most evidence favors a role for testosterone
under the influence of the Hypothalamic-pituitary axis.
ⱴ Cryptorchidism is unilateral in 80% of the case
ⱴ Long-term consequences of cryptorchidism may include testicular malignancy and
infertility/subfertility.
Grossly
ⱴ Cryptorchid testes in adults are small and brown.
ⱴ The testicular tubules are atrophic, and their basement membrane is greatly
thickened
ⱴ In some instances, atypical germ cells are seen at the base ofthe tubules; these are
indicative of intratubular germ cell Neoplasm
ⱴ A cryptorchid testis is 30 to 50 times more likely to
ⱴ Develop a malignant neoplasm than is a normally placed organ.
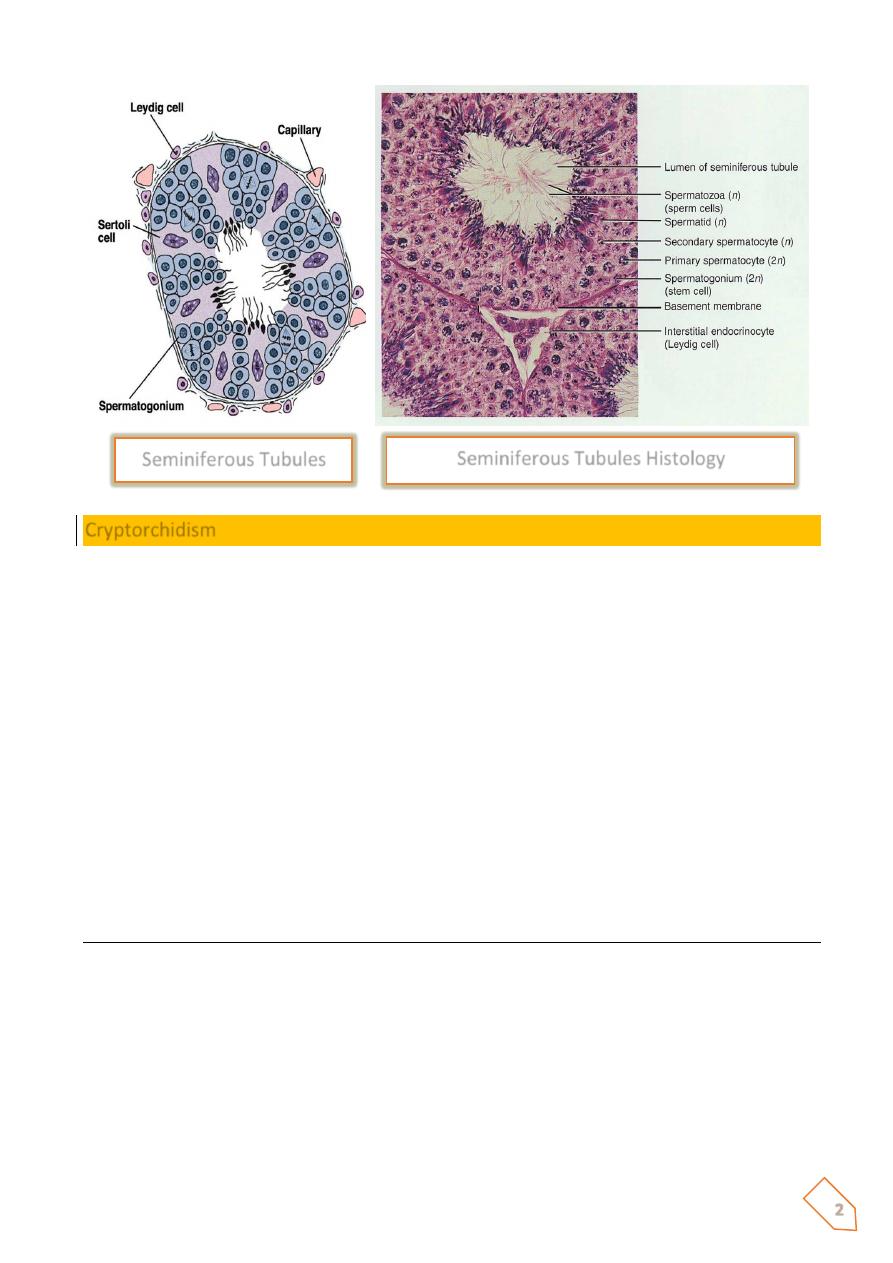
Seminiferous Tubules Histology
Seminiferous Tubules
3
Atrophy and infertility
Atrophy of the testis may result from a large variety of causes:
ⱴ The already mentioned
cryptorchidism
ⱴ The
orchitis of mumps
, especially when the infection occurs at or after puberty;
ⱴ
Liver cirrhosis
, because of increased circulating endogenous estrogens not
metabolized by the diseased liver
ⱴ Administration of
estrogens or gonadotropin-releasing
hormone
analog in the
treatment of prostatic carcinoma
ⱴ Radiation exposure;
ⱴ
Chemotherapy
In advanced testicular atrophy of any of these etiologies, the tubules are small, with thick
basement membranes and few or no germ cells.
The interstitial tissue shows varying degree of fibrosis, and there may be an increased number
of Leydig cells.
The causes of male infertility fall into one of three categories:
1. pretesticular,
2. testicular,
3. Post-testicular.
The pretesticular causes are extragonadal endocrine disorders usually originating in the
pituitary or adrenal gland.
The testicular causes are primary diseases of the testes, and little treatment is available now.
The post-testicular causes consist mainly of obstructions of the ducts leading away from the
testes.
The evaluation of the infertile male includes
1. Clinical history and examination
2. Semen analysis
3. Quantitation of leukocytes in semen,
4. Search for antisperm antibodies.
5. Testicular biopsy particularly useful in the individual with azoospermia and normal
endocrine findings
The material should be handled with extreme care Zenker's and Bouin's fixatives are used.
4
Biopsy specimens from infertile men with total lack of spermatozoa (azoospermia)
usually show one of the following conditions52:
1.
Germ cell aplasia
(Sertoli cell-only syndrome) (29%), In which the tubules are
populated by only Sertoli cells, thickening of the tubular basement membrane; germ
cells are completely absent.
2.
Spermatocytic arrest
(26%), characterized by a halt of the maturation sequence,
usually at the stage of the primary spermatocyte no spermatids or spermatozoa are
present despite the presence of abundant cells in division.
3.
Generalized fibrosis
(18%).
4.
Normal spermatogenesis
(27 %).
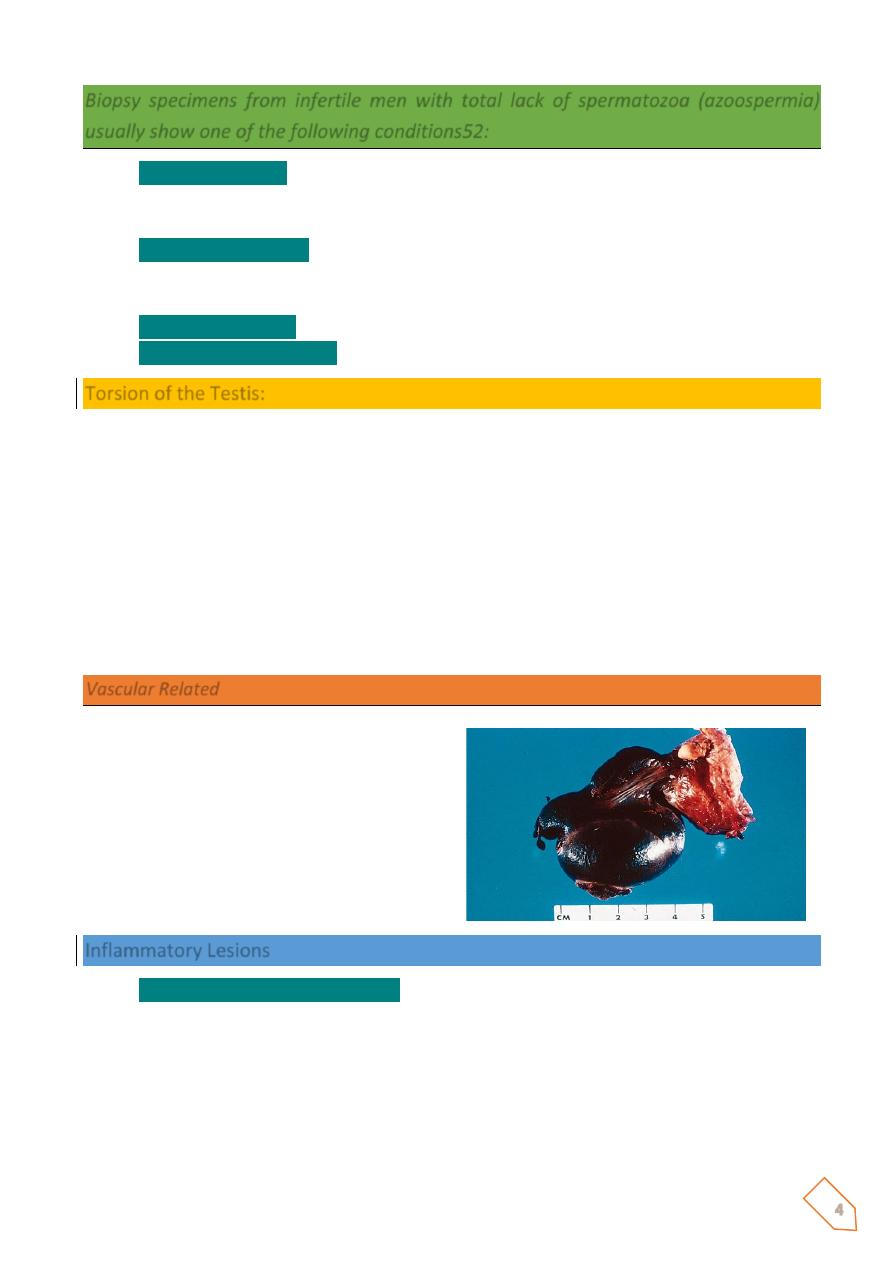
Torsion of the Testis:
(Rotation of the organ 360
ْ
around it longitudinal axis resulting in interruption of its blood
supply)
Sudden severe physical exercise or congenital anomalies that leads to increasing the mobility
of the testis and epididymis such high attachment of tunica vaginalis on the spermatic cord,
incomplete descened of the testis or absent of the scrotal ligments.
These above causes may lead to complete torsion with sudden onset of severe scrotal pain
followed by swelling and hemorrhagic infarction of the testicular germ cells within few hours.
Recurrent incomplete torsion of the spermatic cord results in small fibrotic testis.
Vascular Related
ⱴ Torsion
ⱴ Venous compression
ⱴ Hemorrhagic infarct
ⱴ Young men
ⱴ At night
ⱴ Very painful
ⱴ Can be reduced
Inflammatory Lesions
ⱴ
Inflammatory lesions of the testis
are more common in the epididymis than in the testis
proper. Some of the more important inflammatory diseases of the testis are associated
with venereal disease.
ⱴ Other causes of testicular inflammation include nonspecific epididymitis and orchitis,
mumps, and tuberculosis.

5
ⱴ
Nonspecific epididymitis and orchitis
usually begin as a primary urinary tract infection
with secondary ascending infection of the testis through the vas deferens or lymphatics
of the spermatic cord.
The involved testis is typically swollen and tender and contains a predominantly
neutrophilic inflammatory infiltrate.
ⱴ
Orchitis complicates mumps infection
in roughly 20% of infected adult males but rarely
occurs in children. The affected testis is edematous and congested and contains a
predominantly lymphoplasmacytic inflammatory infiltrate. Severe cases may be
associated with considerable loss of seminiferous epithelium with resultant tubular
atrophy, fibrosis, and sterility.
Disorders of the testicular tunica:-
ⱴ
Hydrocele
: - is the most common cause of the scrotal swelling and it refers to collection
of serous fluid in the scrotal sac (tunica vaginalis). It is either congenital or acquired
due to inflammatory disorders of the epididymis and the testis. Uncomplicated
hydrocele usually presented with unilateral scrotal swelling.
ⱴ
Hematocele
:- refers to hemorrhage into a hydrocele
Hydrocele
ⱴ Fluid filled scrotal cyst.
ⱴ Benign
ⱴ Often with inguinal hernia
ⱴ Transilluminates
ⱴ Fluid will recollect if aspirated.
ⱴ Can be large
Epididmitis
6
Spermatocele:
A cystic enlargement of the efferent ducts or ducts of rete testis. Clinically it is
indistinguishable from the hydrocele but the presence of sperm in the fluid of the
spermatocele differentiates this cystic enlargement from a hydrocele.
Varicocele:
Dilation of the testicular vein which is usually a symptomatic. Most varicoceles are detected
during the physical examination of infertile men, it usually accompanied by testicular atrophy
resulting in infertility.
Surgical treatment with ligation of the internal spermatic vein may need but the subsequent
fertility is inversely related with the duration and the severity of injury to the testicular germ
cells prior to the treatment.
Mubark A. Wilkins
Notes