1
PROSTATE
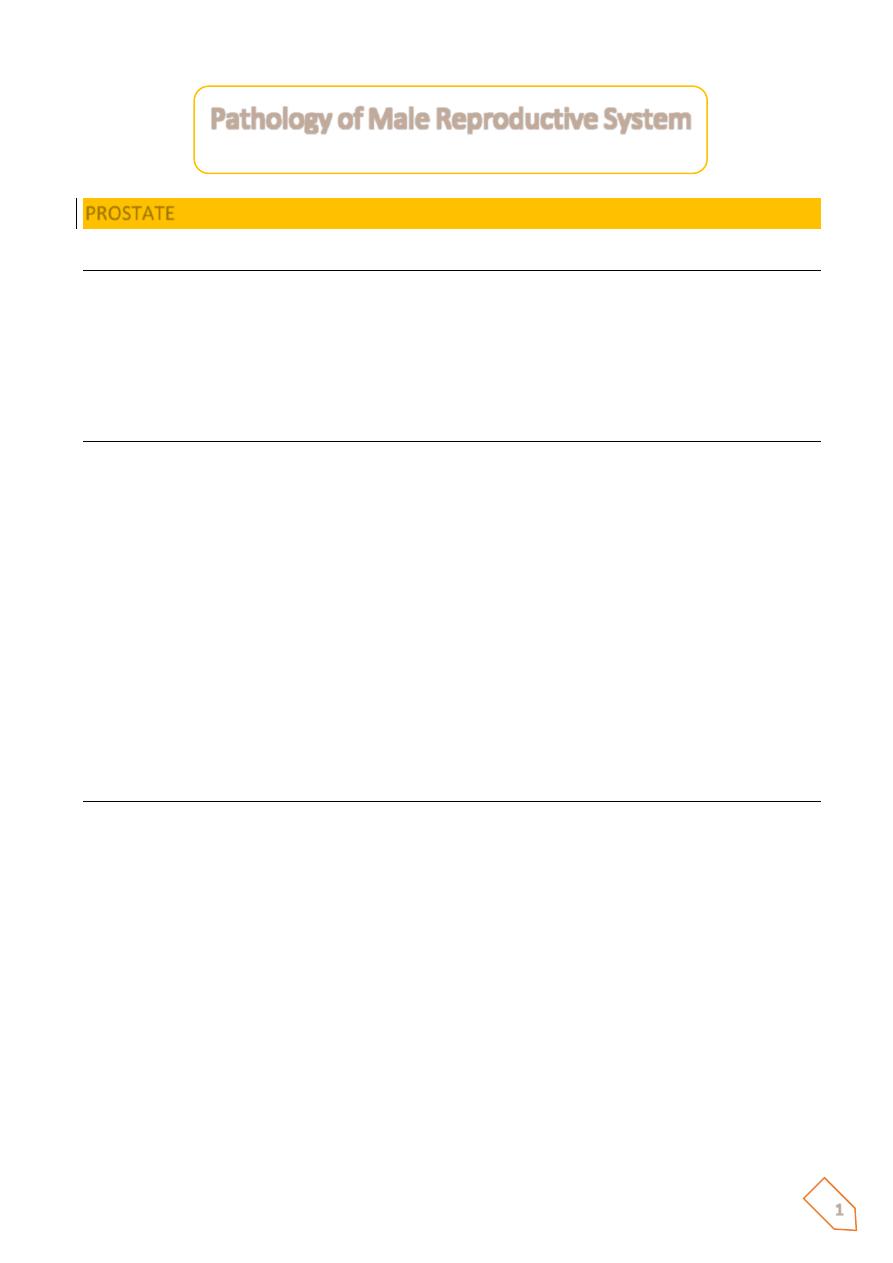
Prostatitis:
Inflammation of the prostate may be acute or chronic, manifested by dysuria, urinary
frequency, and lower back pain. The diagnosis is depended on clinical feature, microscopic
exam and culture of urine specimen that is obtained before and after prostatic massage.
Acute prostatitis:
most commonly associated with LUTI such urethrocysitis caused by E. coli and other G-ve
organisms. These organisms may reach the prostate by either direct extension or by vascular
channels from more distant sites.
• Microscopically characterized by acute neutrophilic infiltration with stromal
congestion and edema in severe infection there is destruction of the glandular
epithelium with microabscesss formation.
• Grossly: visible abscesses uncommon but they may develop in extensive tissue
destruction as in patient with DM.
Chronic prostatitis:
Chronic bacterial prostatitis follows recurrent episodes of acute prostatitis. Chronic a bacterial
prostatitis: there is an increase number of leukocytes in prostatic secretion but negative
finding on bacteriological culture. It caused by the nonbacterial agents such as Chlamydia
trachomatis.
• Microscopically: in addition to the acute inflammatory changes there is lymphoid
infiltration with more glandular tissue destruction and fibroblast proliferation.
• Chronic granulomatous prostatitis: associated with systemic inflammatory processes
such disseminates Tb, fungal infection, sarcoidosis, Wegener granulomatosis.
Pathology of Male Reproductive System
2
Prostatitis
ⱴ Acute bacterial
o Ascending
o E. coli
ⱴ Chronic bacterial
o Low back pain
o Dysuria
o Suprapubic pain
ⱴ ‘Abacterial’
o Chlamydia
Benign prostatic hyperplasia (BPH):-
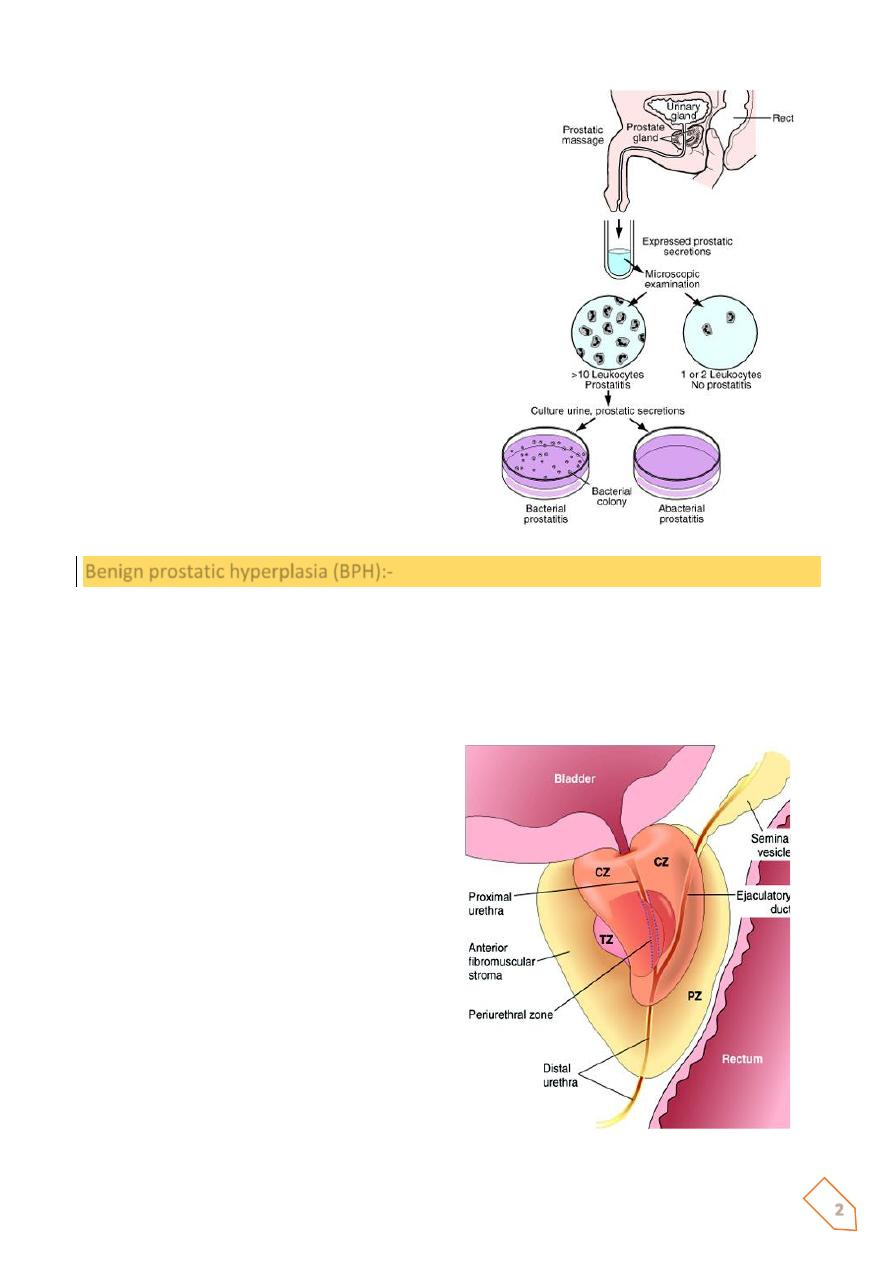
Prostatic parenchyma consists of glandular and stromal elements and it’s divided into specific
regions which are the peripheral, central, transitional, periurethral zones.
Most hyperplastic lesions arise in the inner transitional and central zones while most
carcinomas (70-80%) arise in the peripheral zones.
Nodular
hyperplasia
of
the
prostate
characterized by proliferation of both
epithelial and stromal elements with
enlargement of the gland and urinary
obstruction may occur.
The patient manifested by hesitancy
(difficulty in starting the stream of urine) with
intermittent interruption of urine stream
while voiding and sometimes-complete
urinary obstruction may occur with bladder
distension
and
hydronephrosis.
BPH
developed in significant number of men by
the age 40 and the frequency rises
progressively with age reaching 90% by the
eighth decade.
3
Benign Prostatic Hyperplasia
ⱴ Very common
ⱴ Androgen mediated growth (DHT).
ⱴ Central zone proliferates
o Stroma &
o Glands
ⱴ Minimal if any increased cancer risk
ⱴ Nodular growth pattern
ⱴ Some chronic inflammation
ⱴ Glands always have a double layer of epithelium
o Columnar &
o Reserve layer
4
The cause of the BPH remains incompletely understood but they found that androgens and
estrogens play a synergistic role in its development
Because the androgen play an important role in the pathogenesis of this disease; an intact
testis is necessary for the development of nodular hyperplasia and that’s why nodular
hyperplasia dose not occur in castrated males.
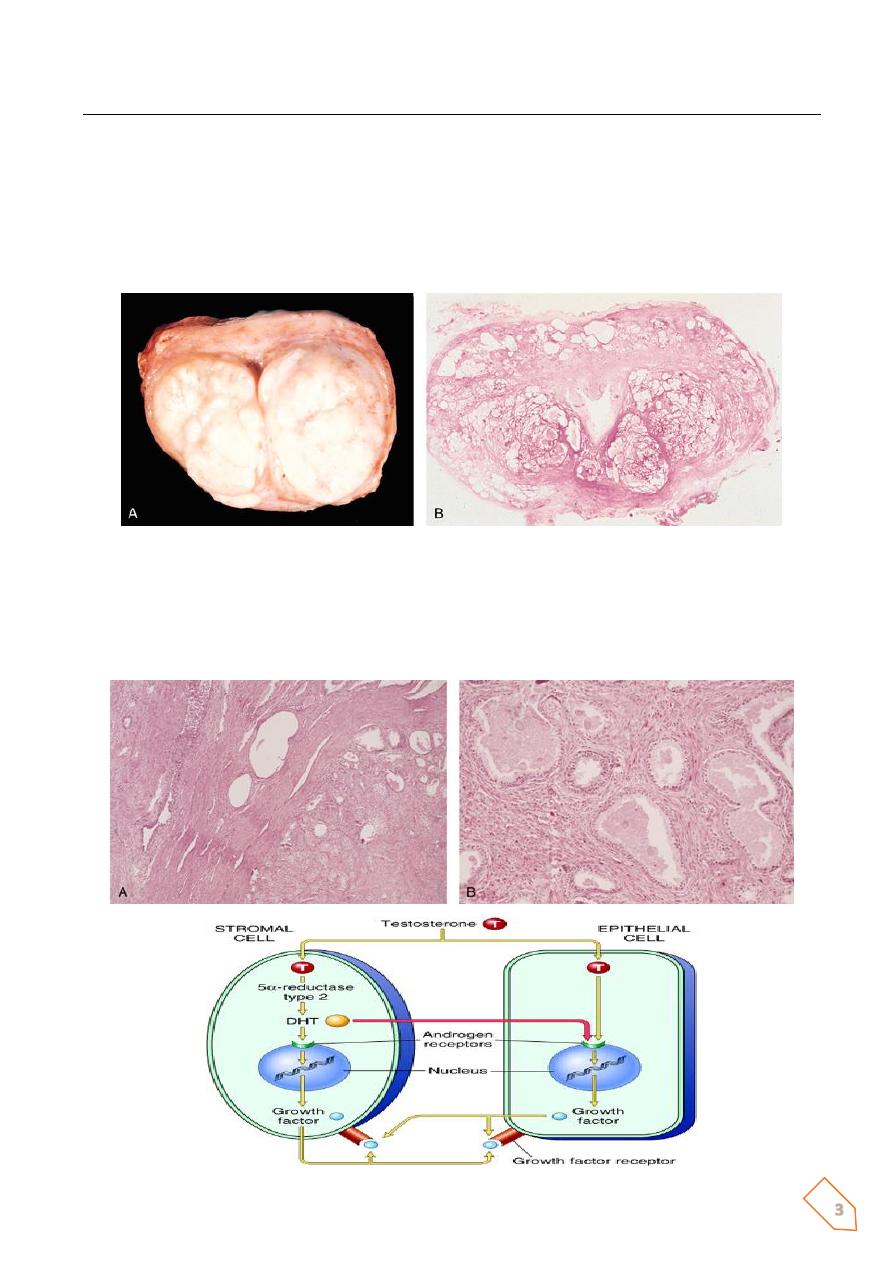
Dihydrotestosterone (DHT) is an androgen derived from the testosterone through the action
5α-reductase but its metabolite 3α-androstanediol appear to be a major hormonal stimulus
for proliferation of both epithelial and stromal elements in patient with BPH, and that’s why
5α-reductase inhibitors used in treatment of symptomatic cases.
Paradoxically
ⱴ BPH is manifested in old age men when the level of the testosterone is either stable or
declined.
ⱴ They also found that; the administration of testosterone dose not exacerbated the
preexisting nodular hyperplasia.
ⱴ From these observations they suggest that there is an other factor that playing a role
in the pathogenesis of the disease rather than androgens and they found that the age
related increases in the estrogen levels may increase the expression of DHT receptors
on the prostatic parenchymal cells and so enhancing the effect of the DHT.
Pathology
ⱴ Nodular hyperplasia arises most commonly in the inner (central and transitional)
region.
ⱴ The affected prostate is enlarged and the developing nodules compress the centrally
located urethral lumen and the normal peripheral prostatic tissue which converted to
an attenuated rim of tissue beneath the prostatic capsule.
ⱴ The cut surface contains multiple well circumscribed nodules which bulge from the cut
surface. The nodules may have a solid appearance or may contain cystic spaces due to
focal hemorrhage and infarction.
Microscopically
ⱴ The hyperplastic nodules composed of varying proportions of proliferating glandular
elements and fibromuscular stroma.
ⱴ The hyperplastic glands are lined by tall columnar epithelium based on flattened basal
cells; papillary projections in some glands due to crowding of the proliferating
epithelium.
ⱴ The glandular lumen often contains inspissated, protienaceous secretory material
termed corpora amylacea.
ⱴ The glands are surrounded by proliferating stromal elements (stroma is always present
between the hyperplastic glands in contrast to carcinoma).