
1
As with other organs, lymph nodes, and more globally, the immune system, can be the
site of infectious, immune and neoplastic disease, the latter either primary or
metastatic
The clinical manifestations of diseases of the lymph nodes are:
o
Local enlargement, tender on nontender, +/_
o
Compression of adjacent structures +/_
o
Release of cytokines producing "systemic" symptoms of fever, weight loss and
night sweats
Infectious organisms can stimulate the same acute, chronic or granulomatous
reactions in the draining lymph nodes as they characteristically stimulate at other sites
Several types of immune stimuli can cause "reactive" enlargement of the entire lymph
node, or selective expansion of cortical, paracortical or medullary regions
Metastatic tumors spread to the lymph nodes primarily via lymphatic drainage from
adjacent solid organs
Primary neoplasms of the lymph nodes are all malignant
They are divided into malignant non-Hodgkin's lymphomas (NHL), and Hodgkin
lymphoma
NHL's are more common, and can be simply divided into indolent, or slow growing
types, and aggressive types
Malignant lymphomas represent clonal malignancies in which mutational events have
caused the majority of progeny cells to freeze at a single stage of normal lymphocyte
differentiation
o Lymphomas frozen at a stage associated with high replication --> aggressive
lymphomas;
o Lymphomas frozen at stages associated with recirculation or final function -->
indolent lymphomas
The diagnosis of malignant lymphomas is based on the microscopic recognition of the
dominant cytologic cell type, supplemented by immunologic and molecular
techniques
The treatment and prognosis of lymphomas are based on
o The dominant cell type (and it's inherent biologic behavior),
o The extent of spread (Stage)
o The underlying health of the patient
All of the previous statements are complicated by the fact that indolent lymphomas
can further mutate and transform to aggressive types
Pathology of Lymph Nodes

2
Hodgkin lymphoma is a less common nodal disease whose diagnosis is based on the
detection of a characteristic cell, the Reed Sternberg cell, in the appropriate histologic
setting
There are several (five) histologic subtypes, but prognosis is based primarily on extent
of disease
Hodgkin lymphoma is a more curable disease than non-Hodgkin lymphomas
Now watch me confuse this relatively straightforward information with the details.
Biopsy
Selection of the lymph node to be biopsied is of great importance. Inguinal nodes are to be
avoided whenever possible because of the high frequency of chronic inflammatory and
fibrotic changes present in them.
Axillary or cervical nodes are more likely to be informative in cases of generalized
lymphadenopathy. Whenever possible, the largest lymph node in the region should be
biopsied. Small superficial nodes may show only nonspecific hyperplasia, whereas a deeper
node of the same group may show diagnostic features.
Bacteriologic examination
If there is a possibility that the node contains an infectious process, an adequate sample of
the biopsied lymph node must be sent directly for bacteriologic study or at least be placed
in a sterile Petri dish in the refrigerator
Needle biopsy
Core needle biopsy is adequate for the diagnosis of metastatic carcinoma but is rarely used
for the evaluation of primary lymphoid disorders.
DNA ploidy studies
Examination of DNA ploidy by flow cytometry of cell suspensions from fluids or material
from fine needle aspiration or from tissue sections has shown a good correlation with the
microscopic grades of malignant lymphoma.
Lymphocytes evolve from pluripotent stem cells --> two major functional cell types:
o B lymphocytes, comprising the humoral immune --> production of antibodies
o T lymphocytes, comprising the cellular immune system, -->
Direct killing of foreign or intracellularly infected cells, cytotoxic T cells
Lymph node evaluation
Overview of the lymphoid immune system
3
Fine control of the immune response through the secretion of
cytokines, helper and suppressor T cells.
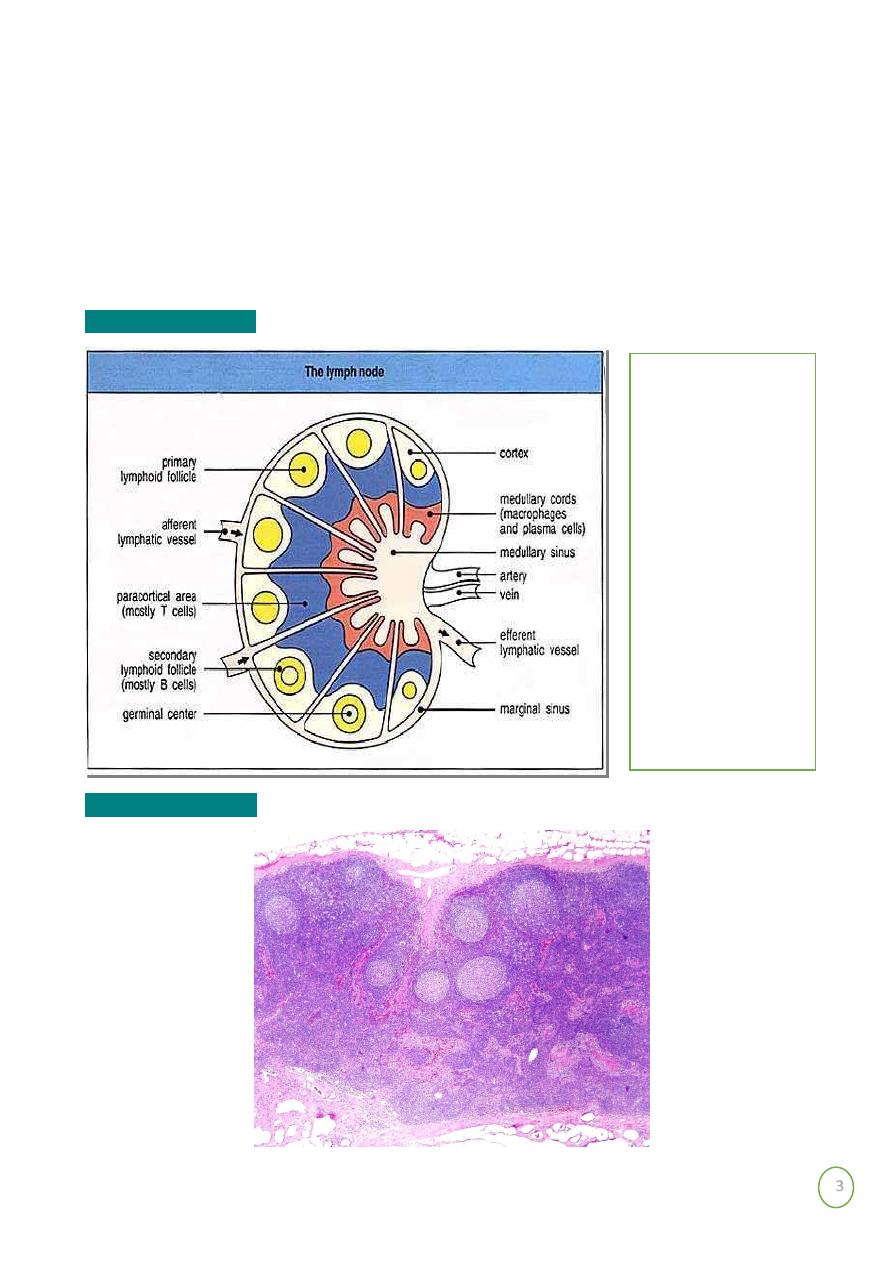
Both cortex and medulla represent B zones and are therefore associated with
humoral types of immune response
The paracortex is the zone situated between the cortex and the medulla, which
contains the mobile pool of T lymphocytes responsible for cell-mediated. Immune
response
Lymph node anatomy
Lymph node histology
To recognize
lymph node
pathology, one has
to be familiar with
normal lymph
node anatomy
and cytology
4
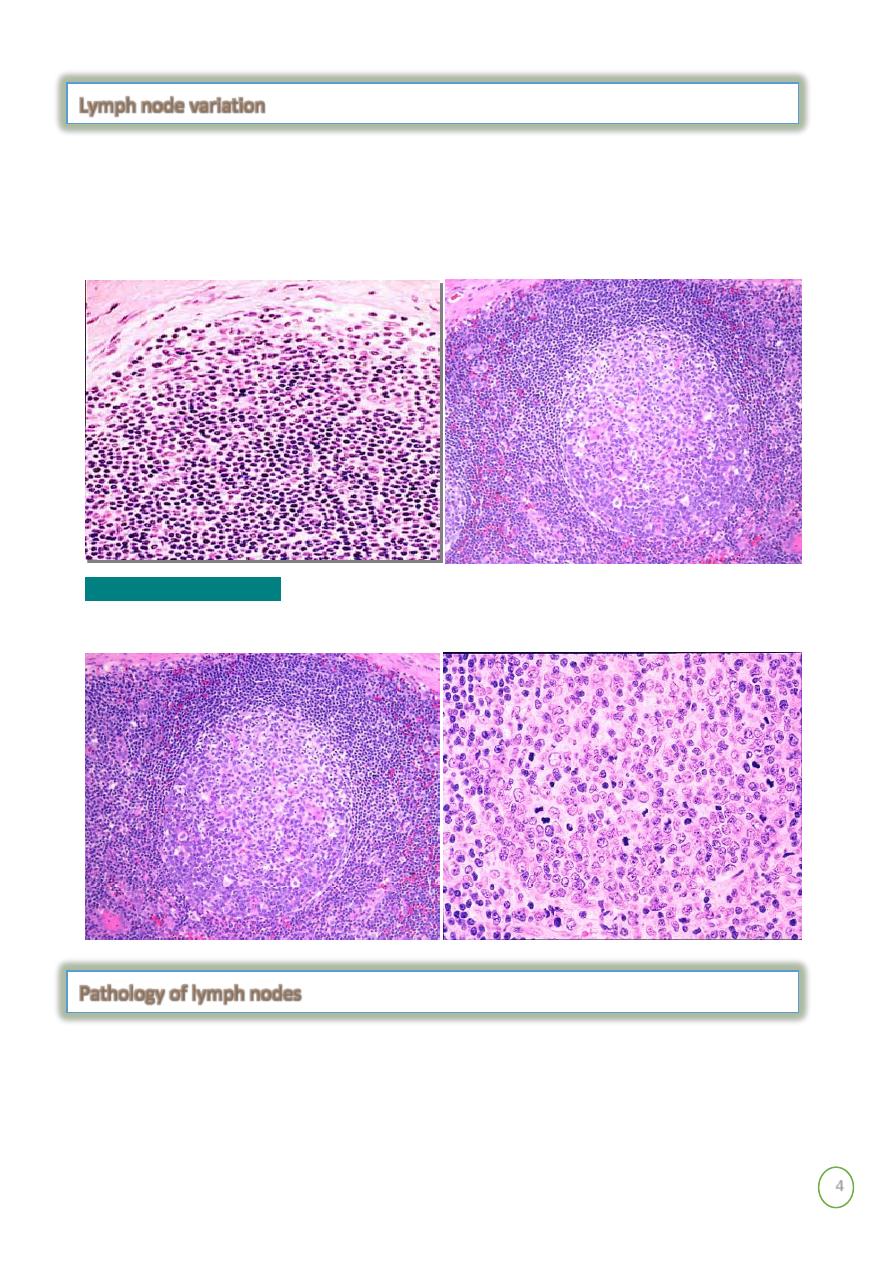
Lymph node histology is dynamic: follicles
o In the absence of immune stimulation, primary follicles on the left.
o In the presence of immune stimulation, secondary follicles or germinal centers
on the right.
Reactive germinal center
Infections
Reactive hyperplasias
Sarcoidosis
Metastatic tumors
Pathology of lymph nodes
Lymph node variation
5
Malignant lymphomas
- Non-Hodgkin’s lymphoma-NHL
- Hodgkin’s lymphoma
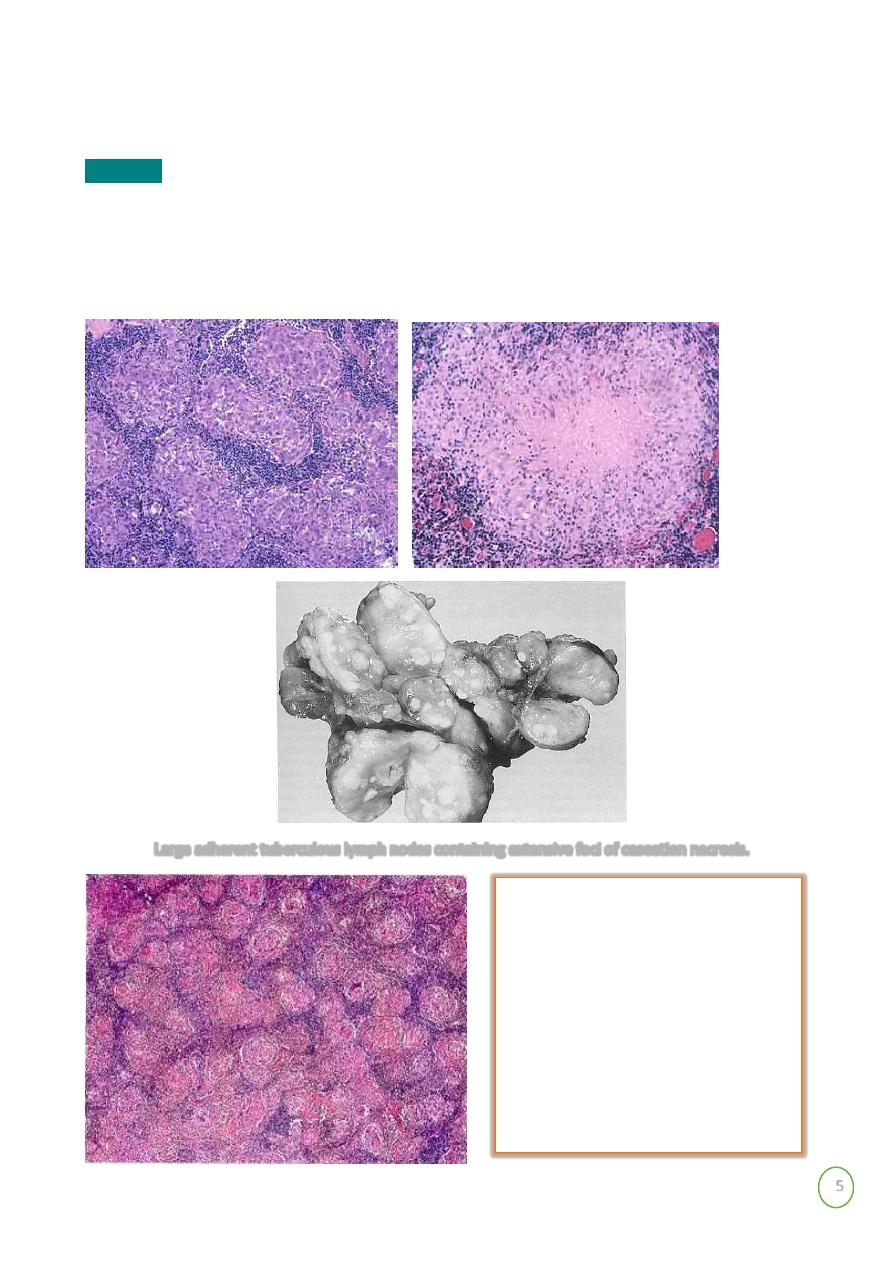
Infections
Bacterial
Acute inflammation, abscess formation
Granulomatous, caseous and noncaseous
Diagnosis by culture, serologies, and/or special stains
Large adherent tuberculous lymph nodes containing extensive foci of caseation necrosis.
Numerous confluent non-
necrotizing granulomas mainly
Composed of epithelioid cells in a
lymph node affected by

6
Exaggerations of normal histology.
o Expansion of all regions or selective expansion
o Some types characteristic of certain diseases, but most not
Follicular hyperplasia
- increase in number and size of germinal centers, spread into
paracortex, medullary areas
o Collagen vascular diseases
o Systemic toxoplasmosis
o Syphillis
Interfollicular hyperplasia
- paracortex
o Skin diseases
o Viral infections
o Drug reactions
Sinus histiocytosis
- expansion of the medullary sinus histiocytes-
o Adjacent cancer
o Infections
Reactive hyperplasia
Mubark A. Wilkins
Asteroid body in the cytoplasm of a
multinucleated giant cell in
sarcoidosis