1
D. Rasha Pathology L4
GRANULOMATOUS DISEASES
Sarcoidosis
Sarcoidosis is a systemic disease of unknown cause characterized by noncaseating
granulomas in many tissues and organs. Sarcoidosis presents many clinical patterns, but
bilateral hilar lymphadenopathy or lung involvement is visible on chest radiographs in
90% of cases. Eye and skin lesions are next in frequency .Since other diseases, including
mycobacterial or fungal infections and berylliosis, can also produce noncaseating (hard)
granulomas, the histologic diagnosis of sarcoidosis is made by exclusion.
Etiology and Pathogenesis.
Although the etiology of sarcoidosis remains unknown, several
lines of evidence suggest that it is a disease of disordered immune regulation in
genetically predisposed individuals exposed to certain environmental agents.”
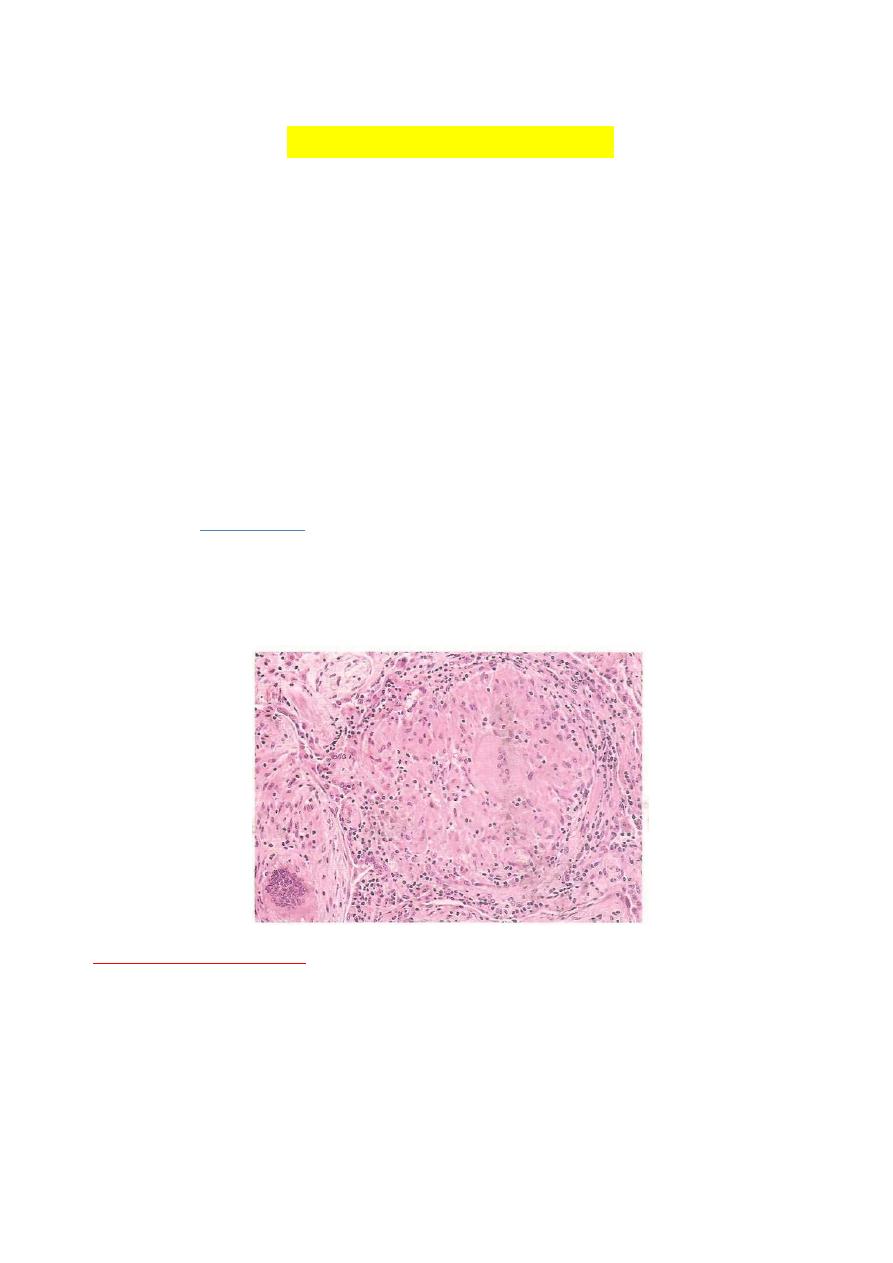
Morphology.
Histologically,
all involved tissues show the classic noncaseating granulomas,
each composed of an aggregate of tightly clustered epithelioid cells, often with Langhans
or foreign body type giant cells. Central necrosis is unusual. With chronicity, the
granulomas may become enclosed within fibrous rims or may eventually be replaced by
hyaline fibrous scars.
PULMONARY INFECTIONS:
Respiratory tract infections are more frequent than infection of any other organ. The
vast majority are upper respiratory tract infections caused by viruses (common cold,
pharyngitis) but bacterial, viral, mycoplasmal, fungal infections of the lung (pneumonia)
still account enormous amount of morbidity and are responsible sixth of all deaths in the
United States. Pneumonia very broadly defined as any infection of the lung parenchyma
(although the same term is used for many interstitial lung diseases that are not infectious
in origin, such as interstitial pneumonia).

2
Pulmonary defense mechanisms:
pneumonia result when these defense mechanisms are
impaired or whenever the resistance of the host in general is lowered.
Factors that affect general resistance include
chronic diseases, immunologic deficiency
diseases and treatment with immunosuppressive agents.
The clearing mechanisms can be interfered with by many factors, such as the following:
Loss or suppression of the cough reflex, as a result of coma, anesthesia,
neuromuscular disorders, drugs, or chest pain.
Injury to the mucociliary apparatus, by either impairment of ciliary function or
destruction of ciliated epithelium, due to cigarette smoke, inhalation of hot or
corrosive material, viral diseases, or genetic disturbances.
Interference with the phagocytic or bactericidal action of alveolar macrophages by
alcohol, tobacco smoke.
Accumulation of secretions in conditions such as cystic fibrosis and bronchial
obstruction.
COMMUNITY-ACQUIRED ACUTE PNEUMONIAS
Community-acquired pneumonias may be bacterial or viral. Often, the bacterial infection
follows an upper respiratory tract viral infection. Bacterial invasion of the lung
parenchyma causes the alveoli to be filled with an inflammatory exudate, thus causing
consolidation (“solidification”) of the pulmonary tissue. Many variables, such as the
specific etiologic agent, the host reaction, and the extent of involvement, determine the
precise form of pneumonia. Predisposing conditions include extremes of age, chronic
diseases (congestive heart failure, COPD, and diabetes), congenital or acquired immune
deficiencies, and decreased or absent splenic function (sickle cell disease or post
splenectomy, which puts the patient at risk for infection with encapsulated bacteria such
as pneumococcus). First we describe pneumonias caused by various organisms and then
the morphologic and clinical features common to most pneumonias.
Streptococcus Pneumonia:
Streptococcus pneumonia, is the most common cause of community-acquired acute
pneumonia. Examination of Gram-stained sputum is an important step in the diagnosis of
acute pneumonia. The presence of numerous neutrophils containing the typical Gram-
positive diplococci supports the diagnosis of pneumococcal pneumonia.
Haemophilus Influenzae
Huemophilus influenzae is a pleomorphic, Gram-negative organism that is a major cause
of life-threatening acute lower respiratory tract infections and meningitis in young
children. In adults, it is a very common cause of community-acquired acute pneumonia.
3
Staphylococcus Aureus
Staphylococcus aureus is an important cause of secondary bacterial pneumonia in
children and healthy adults. Staphylococcal pneumonia is associated with a high incidence
of complications such as lung abscess and empyema.
Legionella pneumophila:
This transmitted by contaminated drinking water. Legionella pneumonia is common in
individuals with some predisposing condition such as ‘cardiac, renal, immunologic, or
hematologic disease. Transplant recipients are particularly susceptible.
Morphology.
Bacterial pneumonia has two
gross
patterns of anatomic distribution: lobular
bronchopneumonia and lobar pneumonia. Patchy consolidation of the lung is the
dominant characteristic of bronchopneumonia. Lobar pneumonia is an acute bacterial
infection resulting in fibrinosuppurative consolidation of a large portion of lung or of an
entire lobe.
In lobar pneumonia
, four stages of the inflammatory response have classically been
described: congestion, red hepatization, gray hepatization, and resolution. Present-day
effective antibiotic therapy frequently slows or halts the progression.
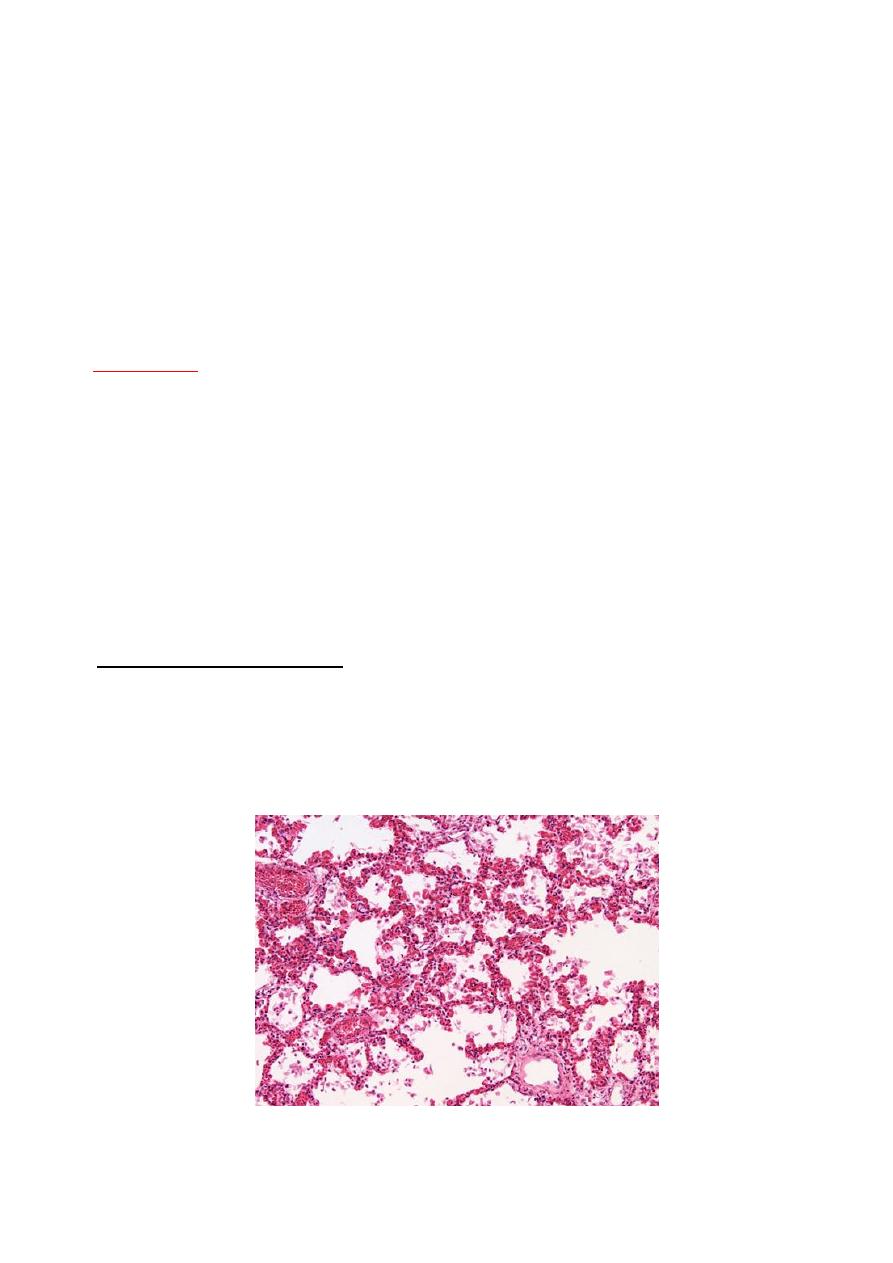
In the first stage of congestion:
Heavy, boggy, and red lung.
Intraalveolar fluid with few neutrophils.
Presence of numerous bacteria.
4
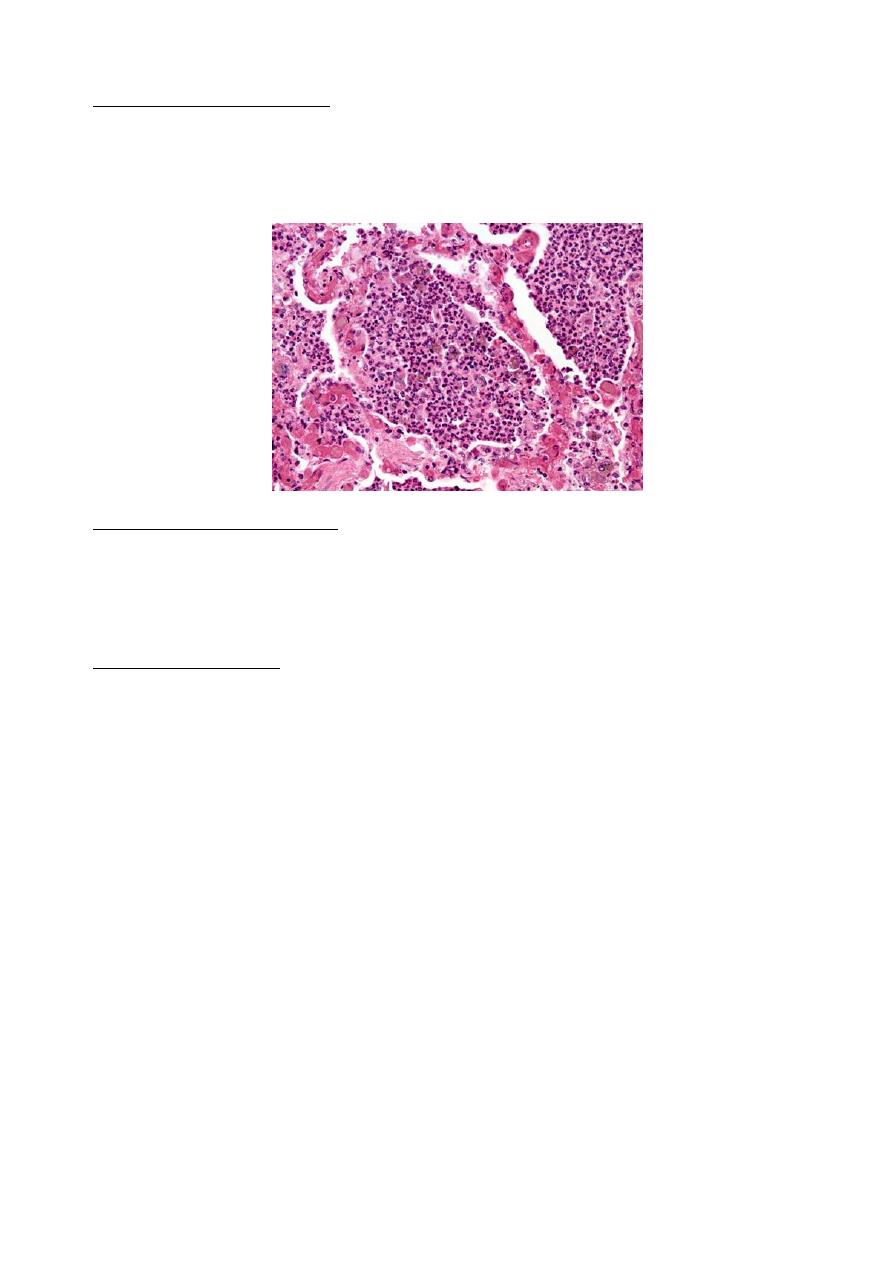
The stage of red hepatization:
Massive confluent exudation with red cells (congestion).
Neutrophils and fibrin filling the alveolar spaces.
Liver like consistency of the affected lobe (firm, red, and airless).
The stage of grey hepatization:
Disintegration of red cells.
Persistence of fibrinosuppurative exudates.
Grayish brown dry surfaces.
The stage of resolution:
-
the exudates undergoes progressive enzymatic digestion of the inflammatory exudates
produce a granular, semifluid debris that is resorbed, ingested by macrophages, coughed
up, or organized.
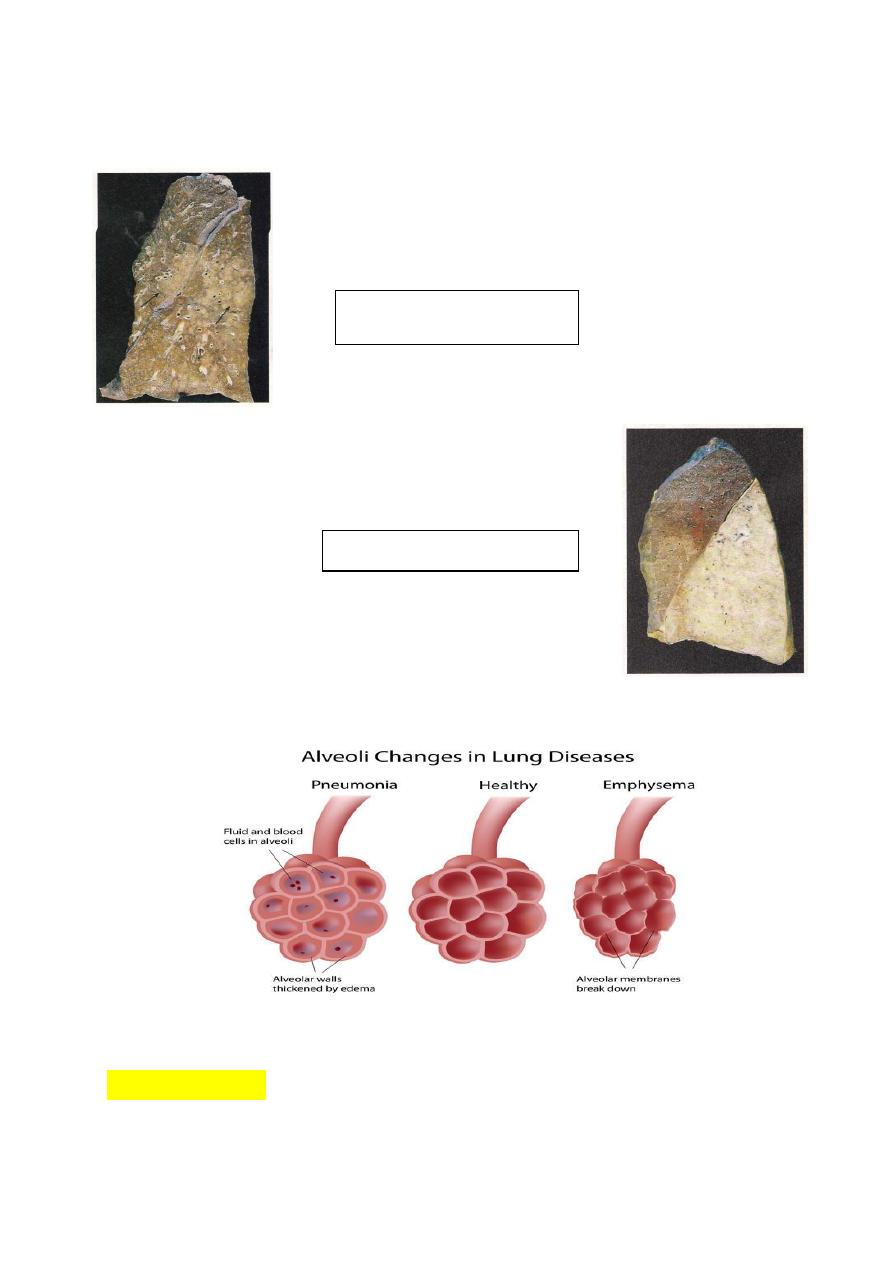
Bronchopneumonia:
They are consolidated areas of acute supportive inflammation. The consolidation may be
patchy through one lobe , multilobular, or bilateral. Well-developed lesions are usually 3
to 4 cm in diameter, dry granular, gray red to yellow.
Histologically.
Suppurative, neutrophil- rich exudates that full the bronchi, bronchioles,
and adjacent alveolar spaces.
COMPLICATIONS:
1. abcess formation.
2. Empyema.
3. Organization of the exudates.
4. Bacterial dissimination.
5
C/F: high fever, productive cough, may have hemoptysis.
RX: antibiotic therapy.
Mubark A. Wilkins
Bronchopneumonia
Lobar pneumonia