Breast pathology II

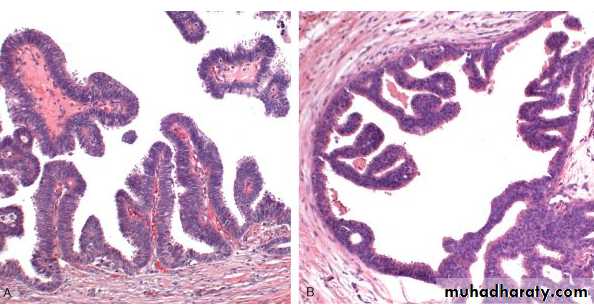
Phyllodes tumors
arise from intralobular stroma.most present in the sixth decade, 10 to 20 years later than the peak age for fibroadenomas
phyllodes is Greek for “leaflike”) due to the presence of nodules of proliferating stroma covered by epithelium

Carcinoma of the Breast
Carcinoma of the breast is the most common malignancy in womenthe incidence of breast cancer began to increase in older women
due to the introduction of mammographic screening in the early 1980s
Since 1994 the breast cancer mortality rate for all women has slowly declined from 30% to 20%
RISK FACTORS
Age
Menarche Age, early menarche is a risk
First-Degree Relatives with Breast Cancer
Breast Biopsies
Race (caucasian the highest)
Estrogen Exposure, prolonged, early menarche, late menopause
Radiation Exposure
Carcinoma of the contralateral breast or endometrium
Obesity
Lack of breast feeding is a risk, Lack of prior pregnancy is a risk.
Tobacco
ETIOLOGY AND PATHOGENESIS
The major risk factors for the development of breast cancer are hormonal and genetic.Breast carcinomas can therefore be divided into sporadic cases, probably related to hormonal exposure, and hereditary cases, associated with germline mutations.
Hereditary Breast Cancer
Mutations in BRCA1 and BRCA2 account for the majority of cancers attributive to single gene mutation (3% of breast cancer)Other genes P53 , CHEK2
Sporadic Breast Cancer
The major risk factors for sporadic breast cancer are related to hormone exposure: gender, age at menarche and menopause, reproductive history, breastfeeding, and exogenous estrogens. The majority of sporadic cancers occur in postmenopausal women
Carcinogenesis and Tumor Progression
The most likely cell type of origin for the majority of carcinomas is the ER-expressing luminal cell, since the majority of cancers are ER-positiveER-negative carcinomas may arise from ER-negative myoepithelial cells
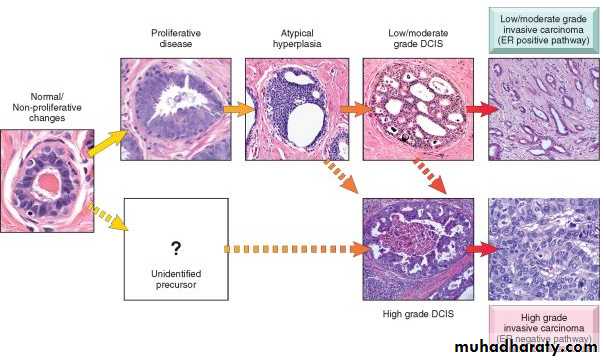
CLASSIFICATION OF BREAST CARCINOMA
divided into in situ carcinomas and invasive carcinomas.Carcinoma in situ refers to a neoplastic proliferation that is limited to ducts and lobules by the basement membrane.
Invasive carcinoma (synonymous with “infiltrating” carcinoma) has penetrated through the basement membrane into stroma.
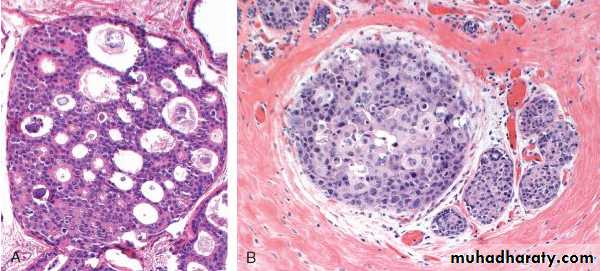
Ductal Carcinoma in Situ
DCIS has been divided into five architectural subtypes: comedocarcinoma, solid, cribriform, papillary, and micropapillaryComedocarcinoma is characterized by the presence of solid sheets of pleomorphic cells with “high-grade” hyperchromatic nuclei and areas of central necrosis

Noncomedo DCIS consists of a monomorphic population of cells with nuclear grades ranging from low to high.
Lobular Carcinoma in Situ (LCIS)
LCIS, and invasive lobular carcinoma all consist of dyscohesive cells with oval or round nuclei and small nucleoli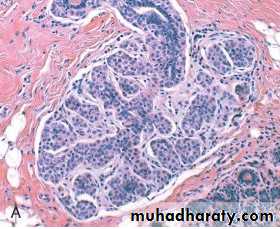
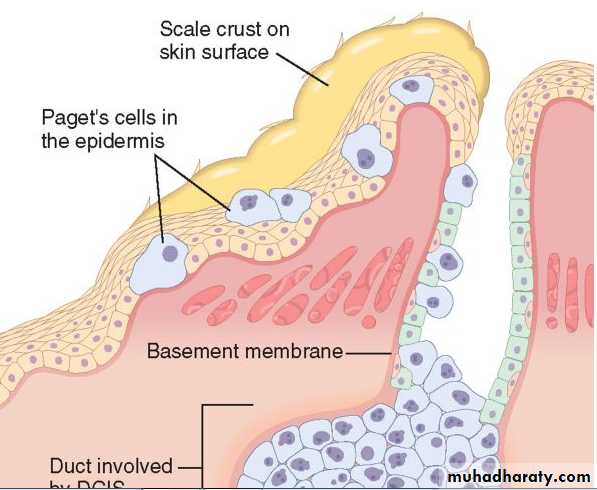
Paget disease of the nipple:
is a rare manifestation of breast cancer (1% to 4% of cases)presents as a unilateral erythematous eruption with a scale crust. Pruritus is common, and the lesion may be mistaken for eczema.
Malignant cells (Paget cells) extend from DCIS within the ductal system, via the lactiferous sinuses, into nipple skin without crossing the basement membrane
Apalpable mass presents in 50%-60% of paget disease indicates presence of underlying invasive ductal carcinoma
DCIS with microinvasion
is an area of invasion through the basement membrane into stroma measuring no more than 0.1 cm.most commonly seen in association with comedocarcinoma
Invasive (Infiltrating) Carcinoma
presents as a palpable mass.Palpable tumors are associated with axillary lymph node metastases in over 50% of patients.
may be fixed to the chest wall or cause dimpling of the skin.
retraction of the nipple may develop
lymphedema and thickening of the skin
mimics the appearance of an orange peel, an appearance referred to as peau d'orange.
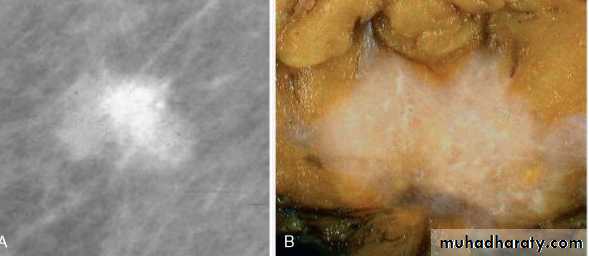
mammography, invasive carcinomas most commonly present as a radiodense mass
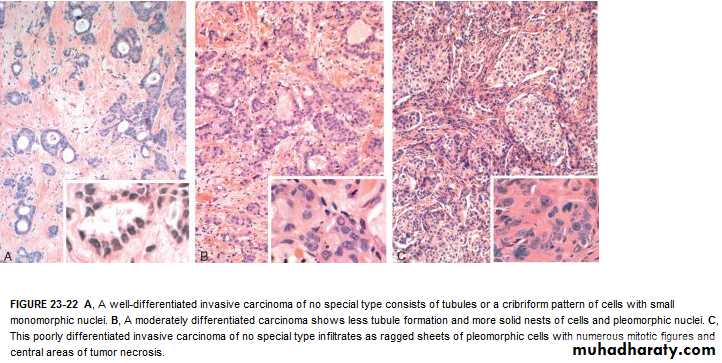
Invasive carcinomas of no special type Invasive Ductal Carcinomainclude the majority of carcinomas (70% to 80%).
Ranging from well differentiated to poorly differentiated
five major patterns of gene expression in the NST group: luminal A, luminal B, normal, basal-like, and HER2 positive
Luminal A” (40% to 55% of NST cancers):
ER positive and HER2/neu negative.
The majority are well- or moderately differentiated, and most occur in postmenopausal women.slow growing and respond well to hormonal treatments
only a small number will respond to standard chemotherapy
Luminal B” (15% to 20% of NST cancers):
expresses ER but is generally of higher grade, has a higher proliferative rate, and often overexpresses HER2/neu.(triple-positive cancers)have lymph node metastases and that may respond to chemotherapy.
Normal breast–like” (6% to 10% of NST cancers):
well-differentiated ER-positive, HER2/neu-negative cancers
Basal-like” (13% to 25% of NST cancers):
absence of ER, PR, and HER2/neu (triple-negative carcinomas)expression of markers typical of myoepithelial cells (e.g., basal keratins, P-cadherin, p63, or laminin)
progenitor cell (e.g., cytokeratins 5 and 6)
include medullary carcinomas, metaplastic carcinomas (e.g., spindle cell carcinoma)
These cancers are generally high grade and have a high proliferation rate.
They are associated with an aggressive course, frequent metastasis to viscera and the brain, and a poor prognosis.
15% to 20% will have a pathologic complete response to chemotherapy
HER2 positive” (7% to 12% of NST cancers):
ER-negative carcinomas that overexpress HER2/neu protein.
These cancers are usually poorly differentiated, have a high proliferation rate, and are associated with a high frequency of brain metastasis.
Invasive Lobular Carcinoma
Lobular carcinomas have been reported to have a greater incidence of bilateralitypresence of dyscohesive infiltrating tumor cells, often arranged in single file or in loose clusters or sheets .
Tubule formation is absent.
Signet-ring cells containing an intracytoplasmic mucin droplet are common.
Desmoplasia may be minimal or absent.
Medullary Carcinoma
most common in women in the sixth decade and presents as a well-circumscribed mass. It may closely mimic a benign lesion clinically and radiologically, or present as a rapidly growing mass.tumor is soft, fleshy (medulla is Latin for “marrow”), and well circumscribed.
Microscopically:(1) solid, syncytium-like sheets of large cells with vesicular, pleomorphic nuclei, and prominent nucleoli, which compose more than 75% of the tumor mass;
(2) frequent mitotic figures;
(3) a moderate to marked lymphoplasmacytic infiltrate surrounding and within the tumor;
(4) a pushing (noninfiltrative) border
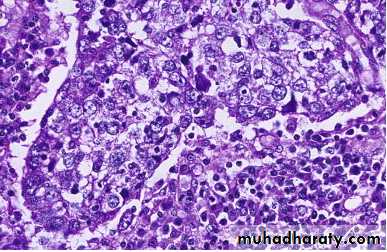
Mucinous (Colloid) Carcinoma
These carcinomas occur in older women (median age 71)
Morphology. The tumor is soft or rubbery and has the consistency and appearance of pale gray-blue gelatin.
The borders are pushing or circumscribed. The tumor cells are arranged in clusters and small islands of cells within large lakes of mucin

Tubular Carcinoma
These tumors consist exclusively of well-formed tubules and are sometimes mistaken for benign sclerosing lesions
PROGNOSTIC AND PREDICTIVE FACTORS
Invasive carcinoma versus in situ diseaseDistant metastases.
Lymph node metastases
Tumor size
Locally advanced disease
Inflammatory carcinoma
Histologic grade, Estrogen and progesterone receptors, HER2/neu, Lymphovascular invasion