
The Breast pathology
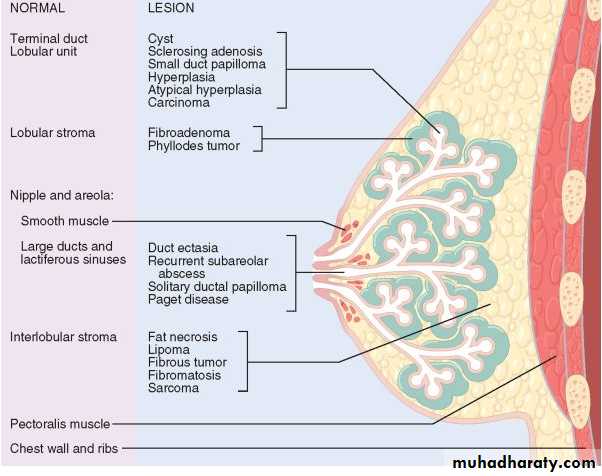
paired mammary glands rest on the pectoralis muscle on the upper chest wall.The breasts are composed of specialized epithelium and stroma
The human breast contains six to ten major ductal systems.
large ducts eventually leads to the terminal duct lobular unit.
Two cell types line the ducts and lobules : myoepithelial cells & luminal cells
There are also two types of breast stroma. The interlobular stroma: dense fibrous tissue + adipose tissue
The intralobular stroma consists of fibroblast-like cells admixed with lymphocytes
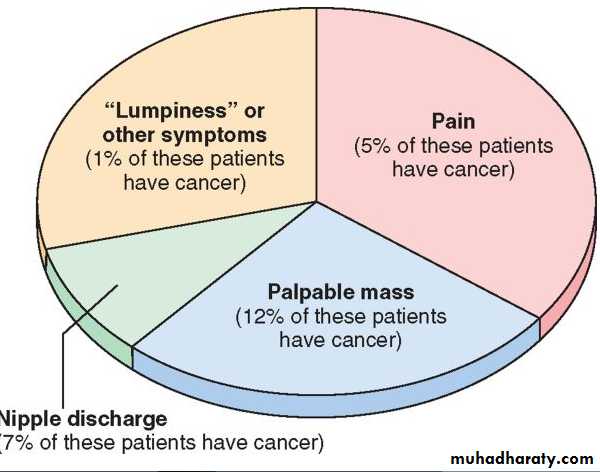
Clinical Presentations of Breast Disease
Pain (mastalgia or mastodynia) is a common symptom that may be cyclic with menses or noncyclic ( due to rupture cyst , infection, physical trauma, etc)
Discrete palpable masses The most common palpable lesions are invasive carcinomas, fibroadenomas, and cysts.
Nipple discharge is a less common finding that is most worrisome when it is spontaneous and unilateral,(ductectasia, intraductal papilloma & carcinoma)
Inflammatory Disorders
ACUTE MASTITIS almost all cases occur during lactation (staph.aureus & less common strept.)MAMMARY DUCT ECTASIA
occur in the fifth or sixth decade of life
Patients present with a poorly defined palpable mass ,thick white nipple secretions and skin retraction.
Morphology dilation of ducts, inspissation of breast secretions and a marked periductal and interstitial chronic inflammatory reaction , granulomatous inflammation
Fibrosis may eventually produce skin and nipple retraction
FAT NECROSIS
present as a painless palpable mass, skin thickening or retractionwomen have a history of breast trauma or prior surgery.
Calcification in mamogram
GRANULOMATOUS MASTITIS
The causes include systemic granulomatous diseases (sarcoidosis)
and granulomatous infections caused by mycobacteria or fungi in immunocompromised patients
or foreign body reaction
Benign Epithelial Lesions
NONPROLIFERATIVE BREAST CHANGES (FIBROCYSTIC CHANGES)
There are three principal morphologic changes:
• cystic change, often with apocrine metaplasia;
• fibrosis; and (3) adenosis.
Cysts.
Small cysts form by the dilation and unfolding of lobules, and may coalesce to form larger cystsCysts are lined either by a flattened atrophic epithelium or by metaplastic apocrine cells. The latter cells, which have an( abundant granular, eosinophilic cytoplasm and round nuclei

Fibrosis.
Cysts frequently rupture, releasing secretory material into the adjacent stroma. The resulting chronic inflammation and fibrosis contribute to the palpable firmness of the breast.Adenosis.
increase in the number of acini per lobule. The acini are often enlarged (blunt-duct adenosis) Calcifications are occasionally present within the lumens.The acini are lined by columnar cells or flat epithelium.
Adenosis.
increase in the number of acini per lobule. The acini are often enlarged (blunt-duct adenosis) Calcifications are occasionally present within the lumens.
The acini are lined by columnar cells or flat epithelium.
Sclerosing Adenosis.
The number of acini per terminal duct is increased to at least double the number found in uninvolved lobulesThe acini are compressed and distorted by stromal fibrosis
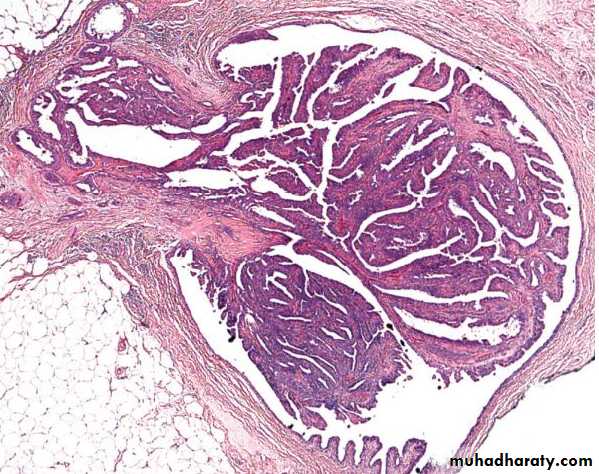
Papillomas
Growth occurs within a dilated duct.multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells
Large duct papillomas are usually solitary and situated in the lactiferous sinuses of the nipple.
Small duct papillomas are commonly multiple and located deeper within the ductal system.
More than 80% of large duct papillomas produce a nipple discharge
Fibroadenoma
a very common benign breast lesion typically occurring in patients between the ages of 20 and 35 years.Grossly,
is a sharply demarcated, firm mass . The cut surface is solid, grayish white, and bulging, with a whorl-like pattern and slit-like spaces. Necrosis is absent
Microscopically: glandular & stroma(loose fibrous tisssue with muccopolysacchride)