1
Fifth stage
Pediatric
Lec. 2
.د
رياض
22/2/2017
ROSEOLA INFANTUM
EXANTHEM SUBITUM
Sixth disease
Epidemiology
• caused by human herpesvirus (HHV) type 6 (HHV-6) for<2yrs old 80% of cases; and
less frequent in
• 10-30% of cases by HHV-7 in older than 2 yr.
• Are DNA viruses, which are of the herpesvirus family
• HHV-6 is a major cause of acute febrile illnesses in infants and may be responsible for
20% of visits to the emergency department for children 6 to 18 months old.
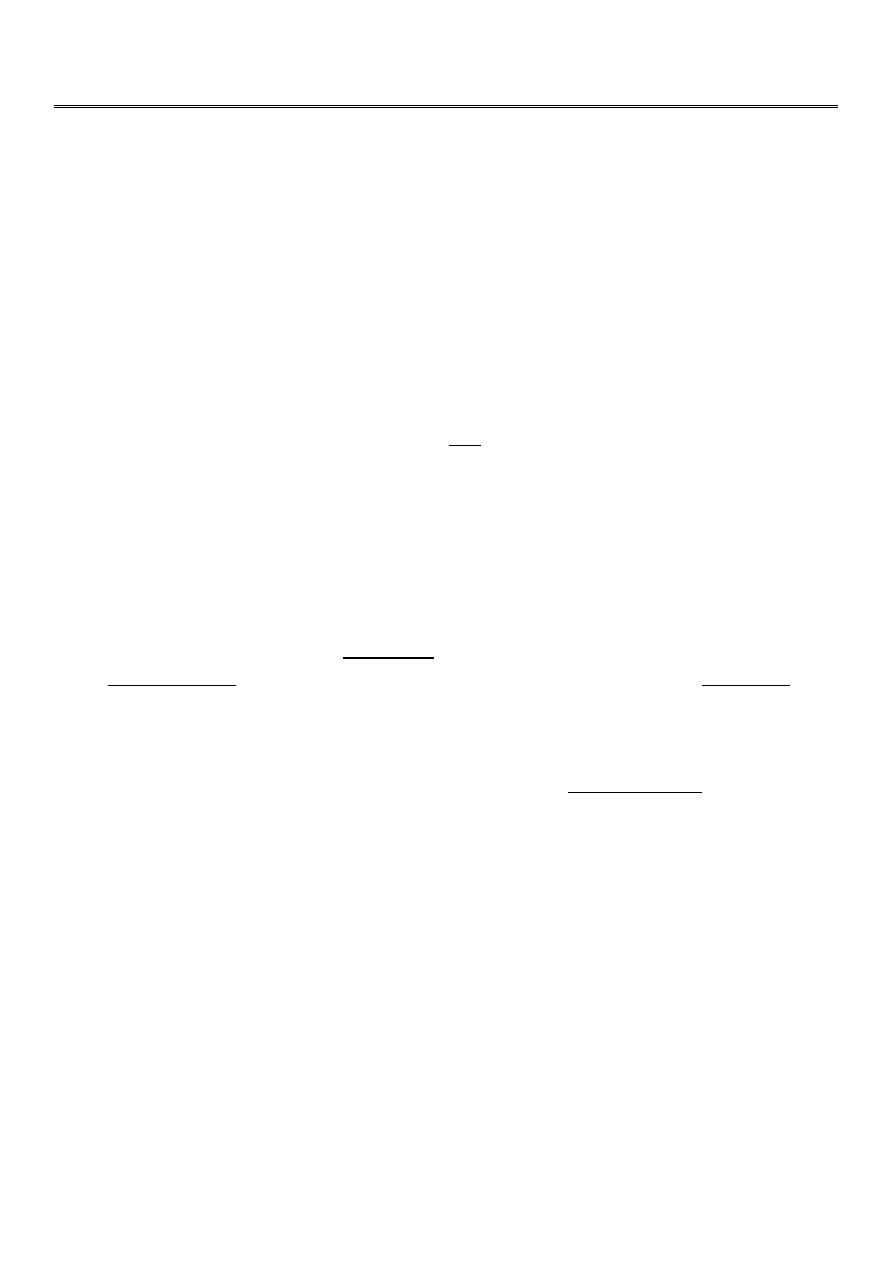
Clinical Manifestations
• Roseola is characterized by high fever (often ≥40°C) lasting 3 to 4 days followed by
maculopapular, rose-colored pruritic rash that appears soon with the remission of
fever.
• The rash usually lasts 1 to 2 days but may fade rapidly
• Roseola is associated with approximately one third of febrile seizures cases.
Treatment
• There is no specific therapy for roseola. Routine supportive care includes maintaining
adequate hydration and antipyretics
2
ERYTHEMA INFECTIOSUM
FIFTH DISEASE
Epidemiology
• caused by the human parvovirus B19
• Single stranded DNA virus.
• Benign self-limited illness affecting any age mostly 5-15 yrs old and even adults.
Incubation period average 15-17 days. It is transmitted by respiratory secretions
airborne route.
• it an important cause of aplastic crisis in patients with hemolytic anemias like
thalassemia, sickle anemia, & spherocytosis. Parvovirus B19 also causes severe fetal
anemia and even hydrops fetalis after primary infection during pregnancy.
Clinical Manifestations
1. usually begin with a mild prodromal nonspecific illness 2-3 days characterized by low
grade fever, malaise, myalgia, and headache.
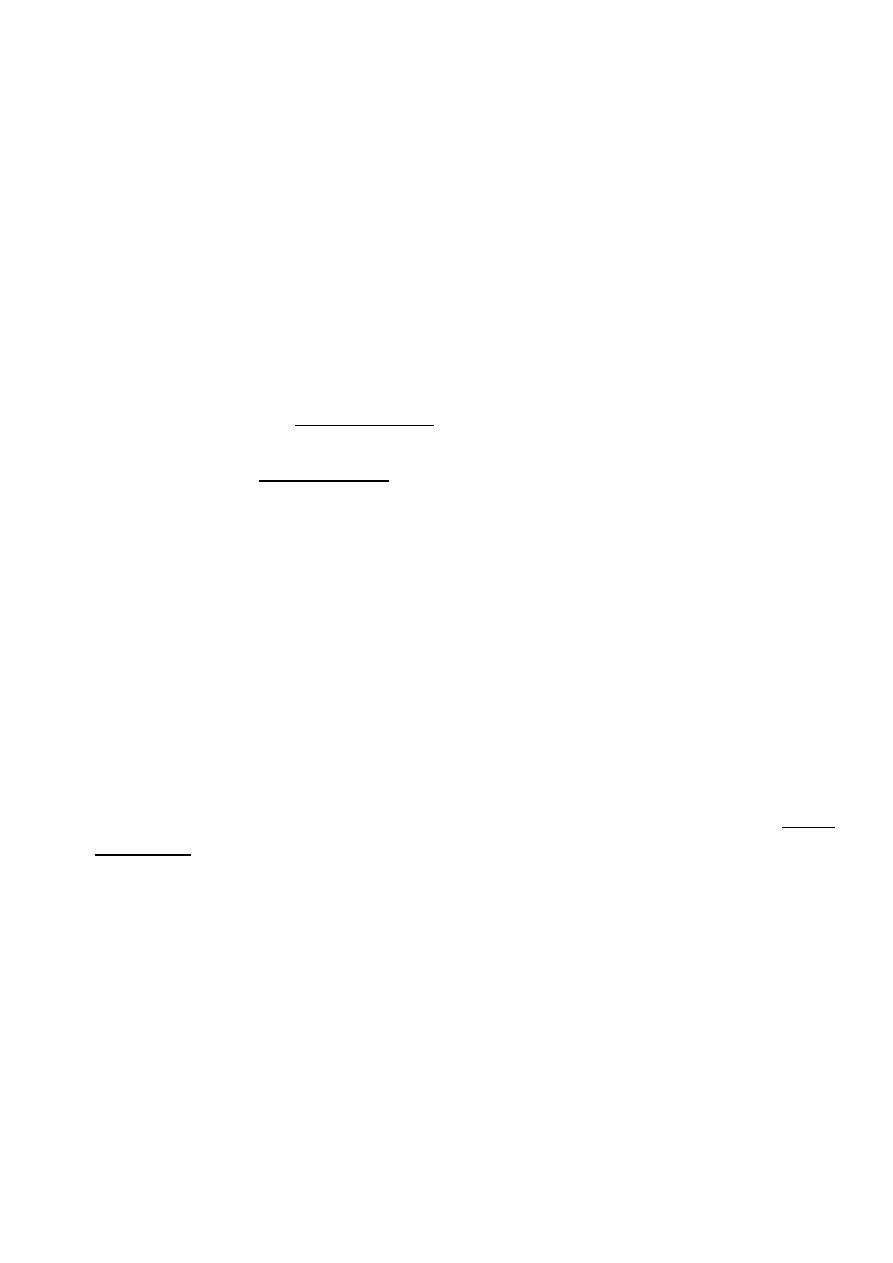
2. This illness is followed by the characteristic rash (Erythema Infectiosum). The rash
appears in two stages:
A. Erythematous cheeks, appearing as a "slapped cheek" rash.
B. After 1-4 days of face rash ; an erythematous symmetric, maculopapular rash, involves
trunk and limbs appears, takes place as distinctive lacy, reticulated rash that lasts few
days to even 1-3 weeks. This rash may be pruritic, does not desquamate – and it waxes
and wanes with exposure to sunlight, heat, bathing, exercise and stress.
3. Arthralgia.
4. anemia due to low RBCs production by bone marrow (suppression) indicated by low
RBC count and low reticulocytes count <1% ; which may be mild anemia or may be
severe called : acquired pure red cell anemia, and in pregnancy= fetal anemia and even
may lead to hydrops fetalis.
Investigations
Includes CBC showing; Low RBC count and; Low Reticulocyte count; and Parvovirus B19 can
be detected by PCR .

3
Treatment
• There is no specific therapy.
• Routine supportive care.
• Transfusions may be required for ; transient aplastic crisis in pt. with hemolytic
diseases or in ; aquired pure red cell anemia.
• Intrauterine transfusion has been performed for hydrops fetalis associated with fetal
parvovirus B19 infection.
VARICELLA-ZOSTER VIRUS INFECTION
Chickenpox
• DNA virus that is a member of the herpes virus family
• Humans are the only natural host.
• VZV (chickenpox) is highly communicable among susceptible individuals.
• It is mild disease in young children but may be severe in adult and in
immunocompromised children
• Both chicken pox( varicella) pt. and pt with zoster lesion (shingles) infect susceptible
child leading to chicken pox illness.
• the period of infectivity to others; ranges from 2 days before to 7 days after the onset
of the rash till the time when all lesions are crusted and dried.

4
Epidemiology
• the peak age of 5 to 10 yr.
• peak seasonal infection in late winter and spring
• Transmission is airborne route by inhalation of the virus in air droplets from pt.
sneezing or coughing; also by direct contact with the lesions before it become dried
or crusted.
Clinical Manifestations
• The incubation period of varicella is generally 14 to 16 days
• Prodromal symptoms ; fever, malaise, and anorexia, running nose may precede the
rash by 1 day
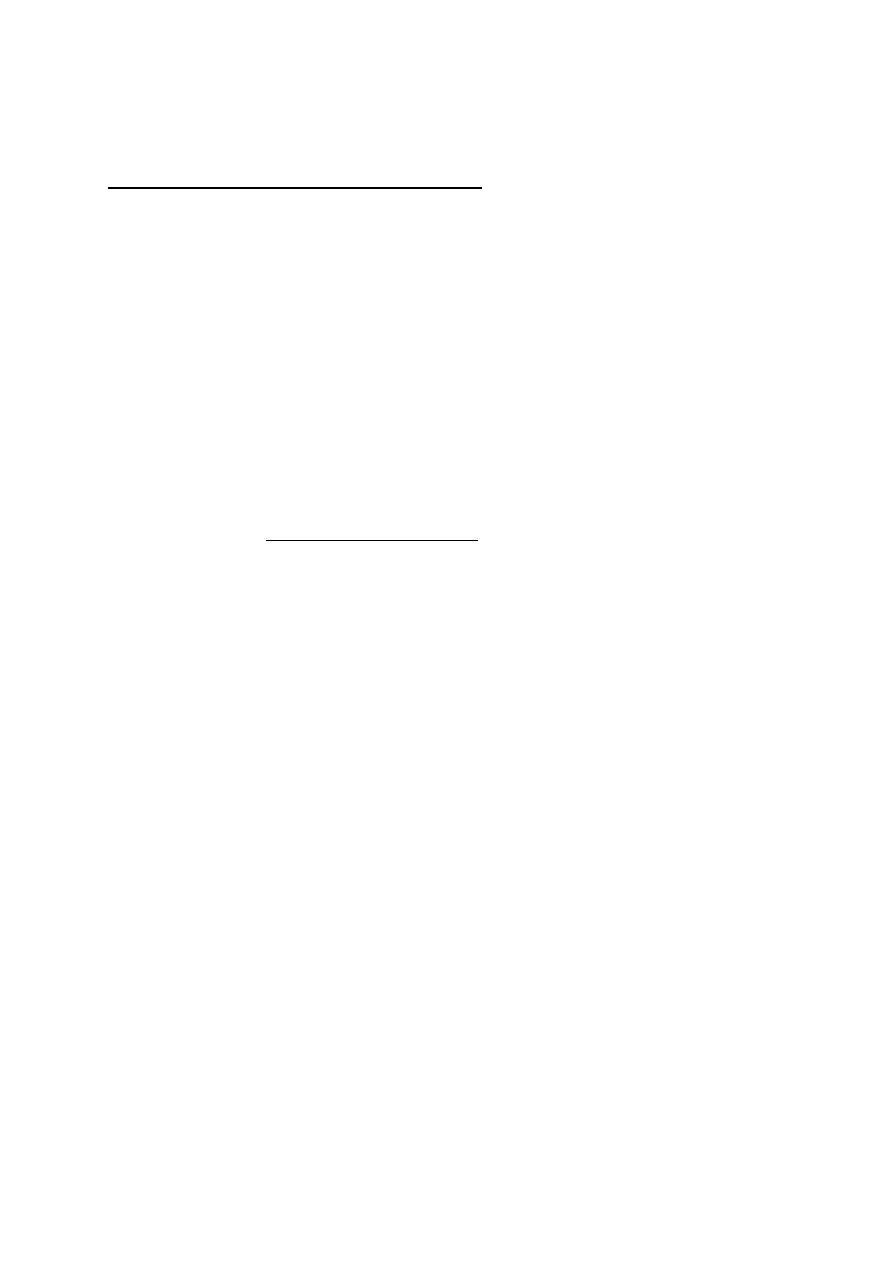
• The characteristic rash appears initially as small red papules that rapidly progress to
oval, "teardrop" vesicles on an erythematous base and appears in crops (different
lesions) of lesions: papules and vesicles. The fluid progresses from clear to cloudy,
and the vesicles then ulcerate, finally; crusted, and dried and heal.
• New rash appear in 3 to 4 days, usually beginning on the trunk followed by the scalp,
the face, conjunctiva, mouth mucosa and, less commonly, the extremities., with all
stages of lesions being present at the same time(crops). Pruritus is universal.
• Periods of illness is about 1-2 weeks .
• Shingles(herpes zoster) is recurrence of VZV infection in previously infected child.
Congenital varicella
• Fetal varicella during first 6 months of pregnancy includes followings pathological
effects: low birth wt, cortical brain atrophy, mental retardation, cataract,
microcephaly, cicatrical scarring of body and limbs with aplasia of fingers and toes.
Complications
1. Secondary bacterial skin infection of the skin by staph. aureus or streptococcus.
2. Pneumonia is uncommon in healthy children, but may occurs in 15% to 20% of healthy
adults and in immunocompromised persons.
3. hemorrhagic lesions (varicella gangrenosa)
4. Reye syndrome when aspirin used.
5. Encephalitis and acute cerecbellar ataxia, Guillain-Barrie syndrome.
5
Treatment
• Symptomatic therapy of varicella includes nonaspirin antipyretics, cool baths, and
careful hygiene.
• ANTIVIRAL(acyclovir) THERAPY indicated; IN infected:
1. immunocompromised persons and in pt under long term corticosteroids therapy,
2. adult above 15 yrs
3. neonates less than 28 days old of un- immunized mother, and in premature baby
whatever the mother immunity; because the baby will not receive immunity from
mother and his illness will be severe.
Prevention
• Varicella vaccine is live attenuated , is recommended for routine administration to
children with 2 doses: at 12 mo and at 4–6 yr of age.
• Passive immunity can be provided by VZIG, which is indicated within72 hours of
exposure to infected pt. in those individuals at increased risk for severe illness,
including:
1. immunocompromised persons in contact ,
2. neonates of infected mothers who had onset of chickenpox within 5 days before
delivery or 48 hours after delivery to prevents getting infection because it will be severe
and may be fatal.
3. Newborn fullterm of un-immunized mother and premature baby as contacts to
infected child.
full-term Newborn of mother with previous immunity, will be protected and no needs
for VZIG if exposed to pt.
4. Adult and ages 15 yr and older, who are exposed to infection.