Upper limb articulations

OBJECTIVES
…
To classify joints according to their shape &
structure
To describe the anatomy of upper limb joints
To apply to some clinical conditions
JOINTS:
Joints are sites where skeletal structures (bones &/or cartilages) are
connected to each other
Joints are designed for movements though some are immobile
All bones (except the hyoid) are connected to joints
There are 230 joints in human body!
Structural types:
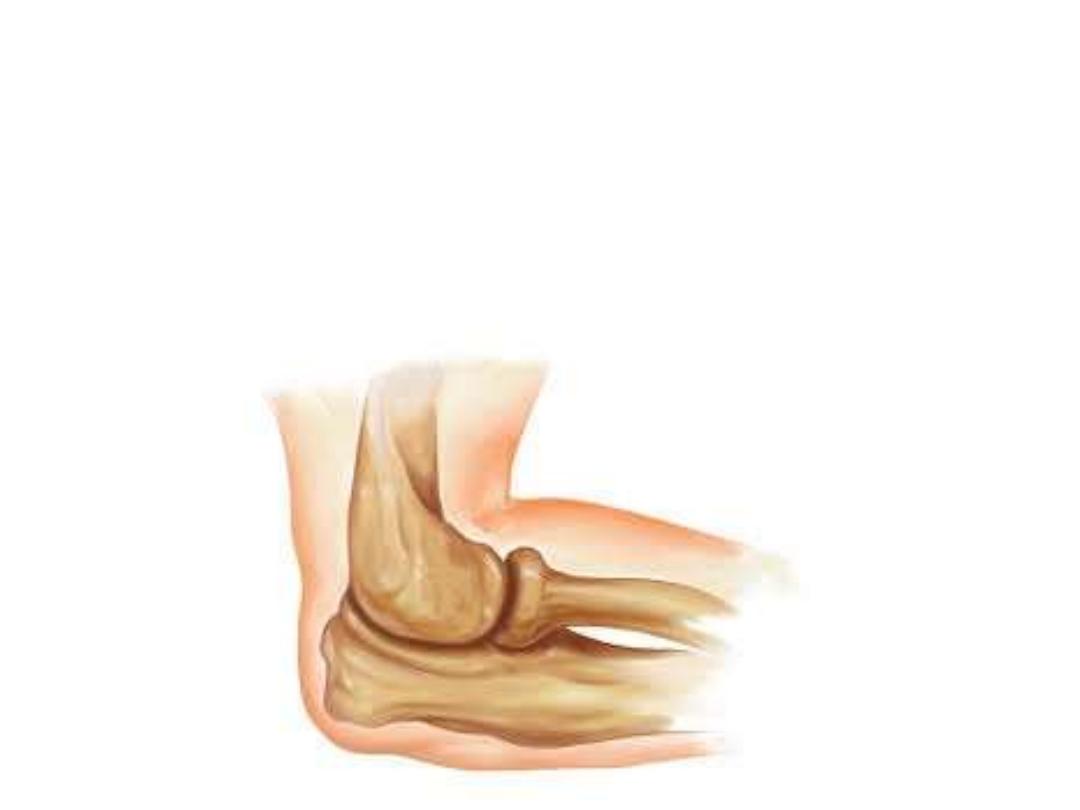
Fibrous joints:
-Articulating surfaces are fastened together by dense connective tissue
containing collagen
-Most of them are immobile
-Examples; skull sutures, tibiofibular joints
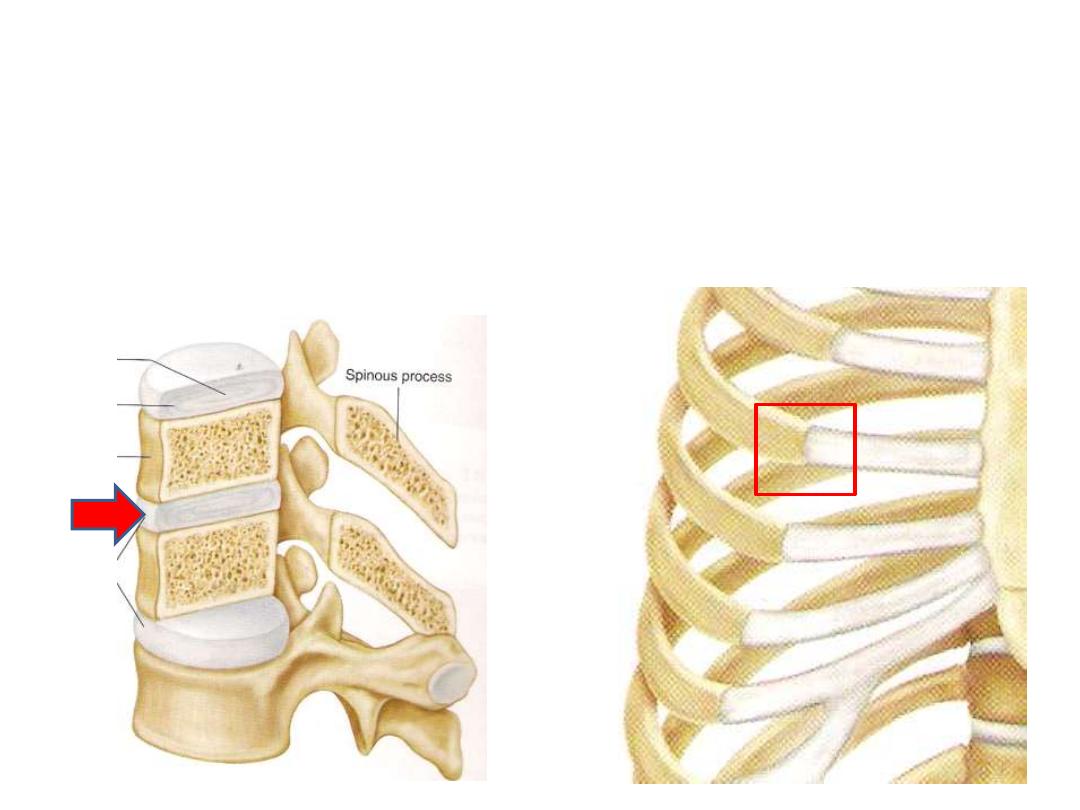
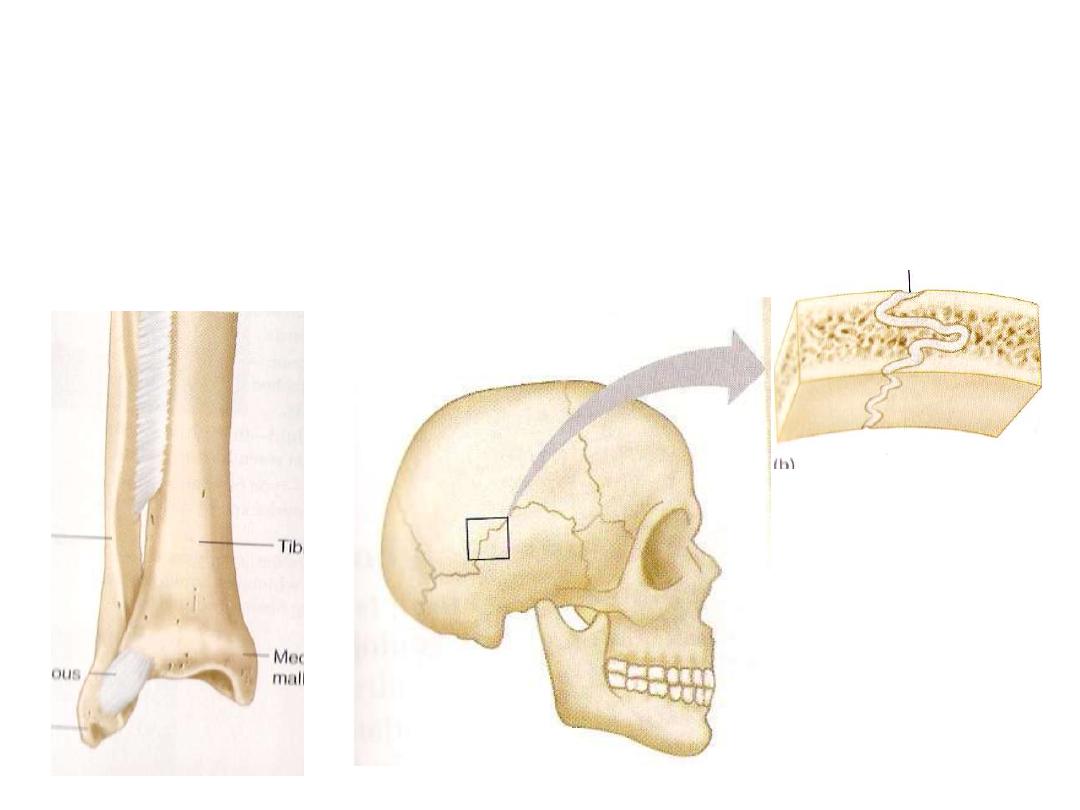
Cartilagenous joints:
-Articulating surfaces are connected by hyaline cartilage or fibrocartilage
-They provide little or no movement
1- Primary cartilagenous joints;
bone meets hyaline cartilage, like the costo-chondral
joint
2- Secondary cartilagenous joints (symphesis);
Bones covered by a hyaline cartilage &
held by fibrocartilage, like intervertebral discs
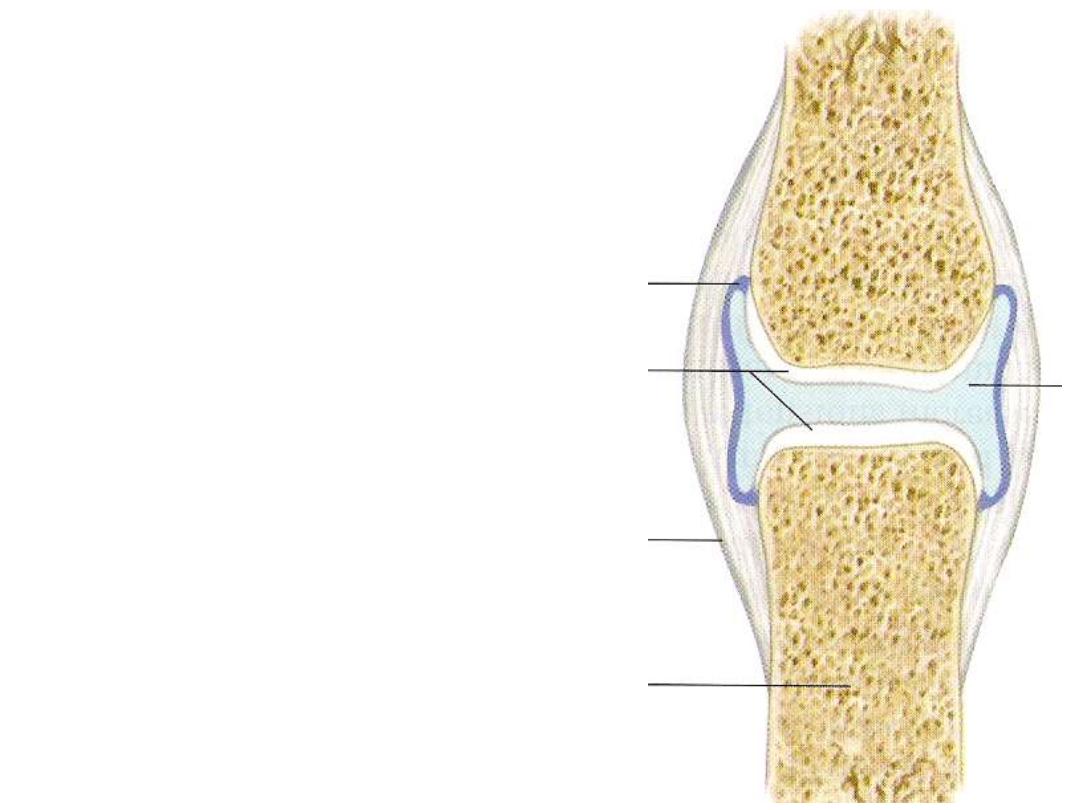
Synovial joints:
Characterized by:
1- Surrounded by a joint capsule
2- Supported by ligaments
3- Lined with synovial membrane
4- Covered by hyaline cartilage
5- Contains synovial fluid
1
4
5
3
example
Possible movement
Description
Joint type
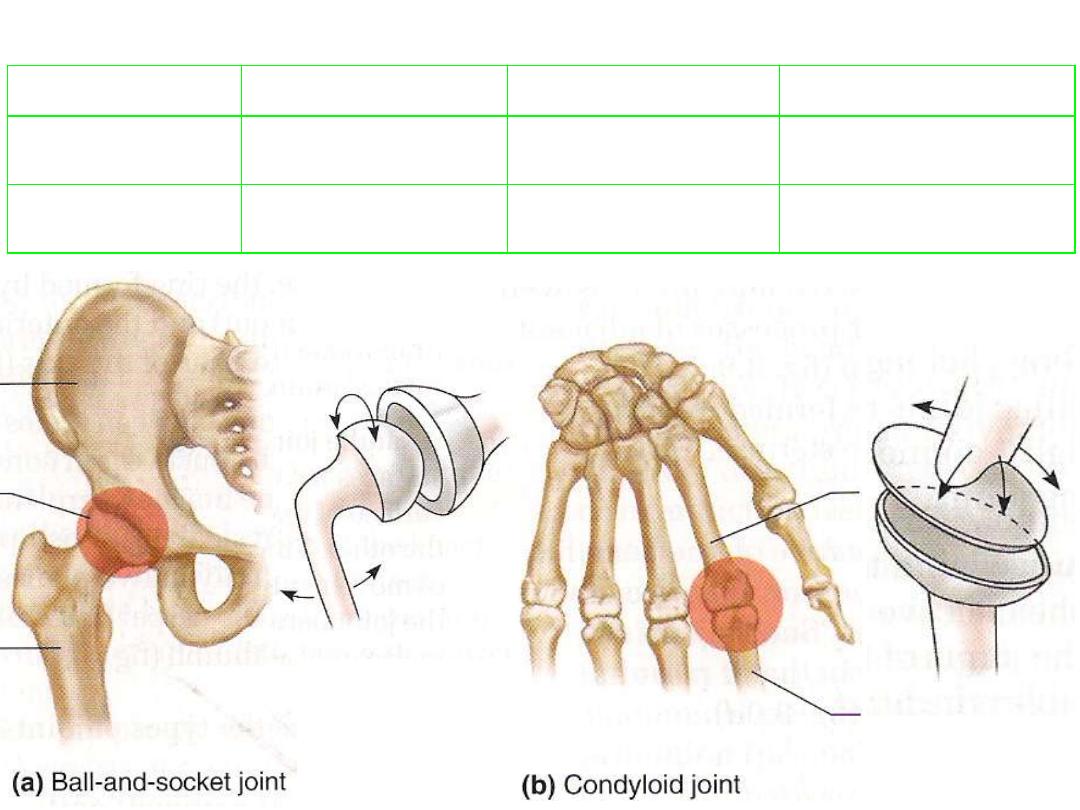
Hip, shoulder
Free + rotation
Ball-shaped head +
cup-shaped socket
1- Ball & socket
Metacarpo-phalyngeal
Free without rotation
Oval condyle +
elliptical cavity
2- Condyloid
Morphological types:
example
Possible movement
Description
Joint type
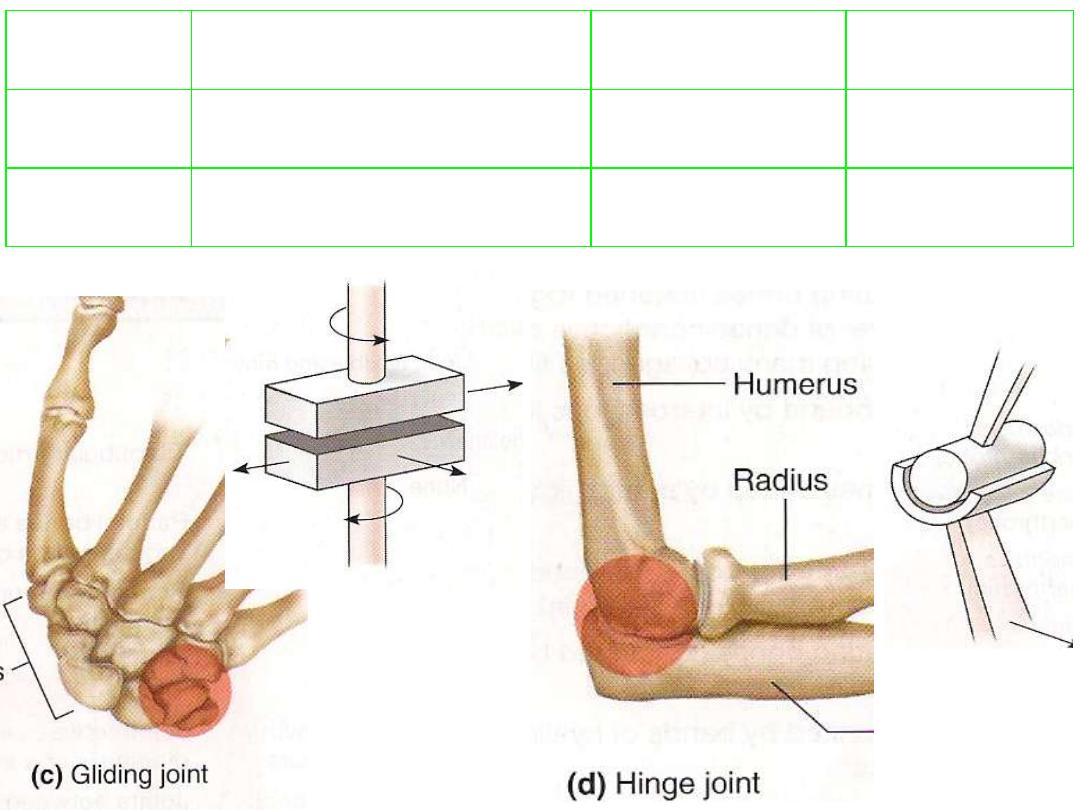
Intermetacarpal
Sliding or twisting
Articulating surfaces are flat or
slightly curved
3- Gliding
Elbow
Flexion-extension
Convex surface + concave one
4- Hinge
example
Possible
movement
Description
Joint type
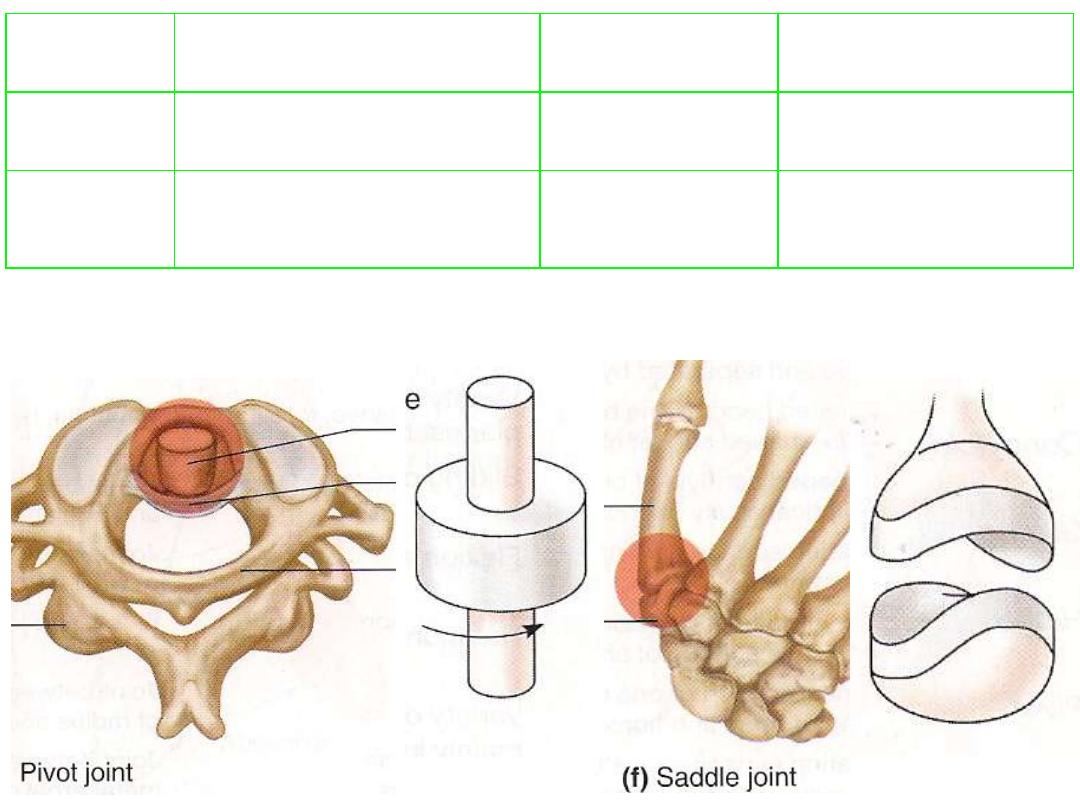
Atlantoaxial
Rotation
Cylindrical surface + ring
surface
5- Pivot
Carpometacarpal joint
of thumb
Mainly movements
in two planes
Articulating surface is both
convex & concave against
complementary surface
6- Saddle
Joint stability:
The stability of joint is maintained by three main factors:
• Morphological
• Lligamentous
• Muscular
All these factors usually share in joint stability, although one of them will
prdominates in specific joints
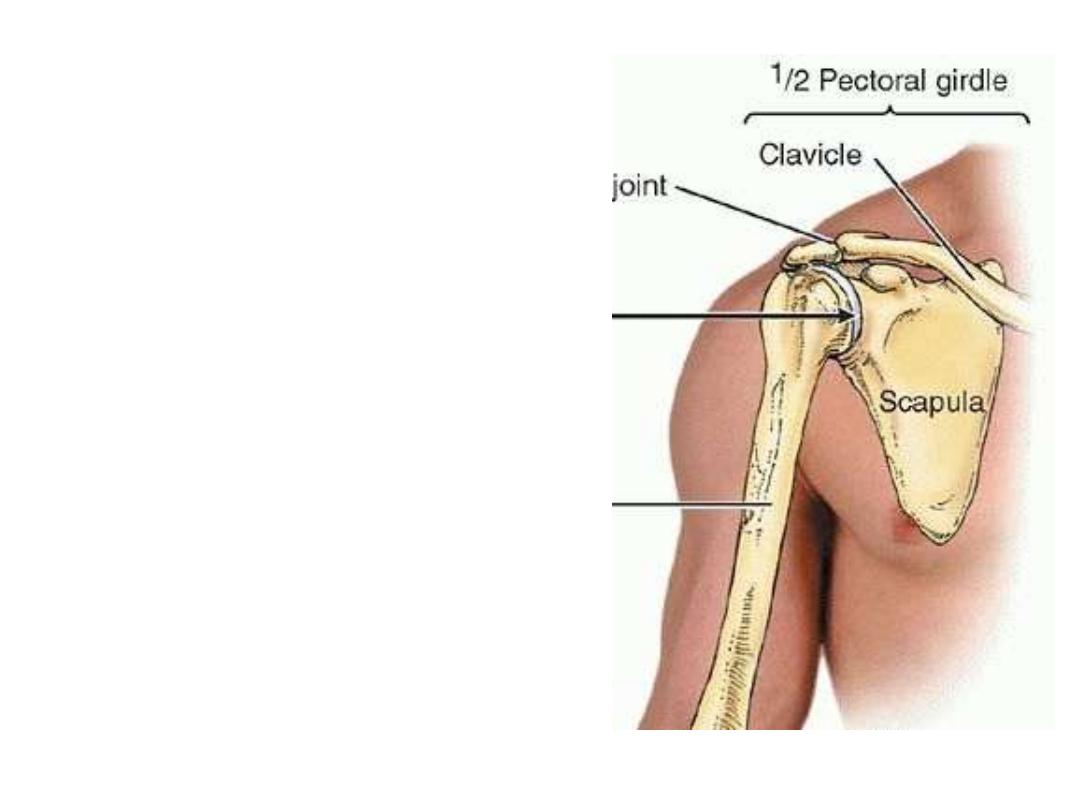
The shoulder joint:
• The shoulder is the region of
upper limb attachment to the
trunk and neck.
• The bony framework of the
shoulder
consists
of
the
clavicle,
scapula
&
the
proximal end of the humerus
• The shoulder constitutes 3
joints; the sternoclavicular,
the
acromioclavicular
&
glenohumeral joints.
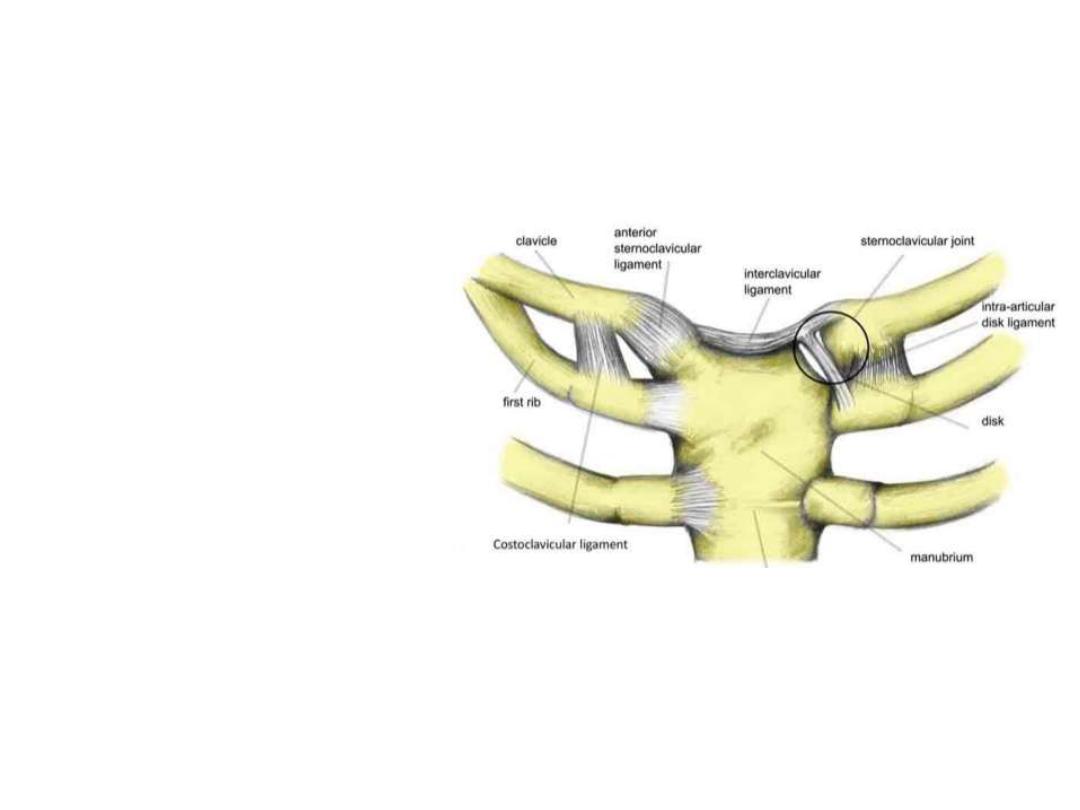
Sternoclavicular joint:
•It is synovial & saddle-shaped.
•The
articular
cavity
is
completely separated into two
compartments by an articular
disc.
•It allows movement of the
clavicle, predominantly in the
anteroposterior
and
vertical
planes, although some rotation
also occurs.
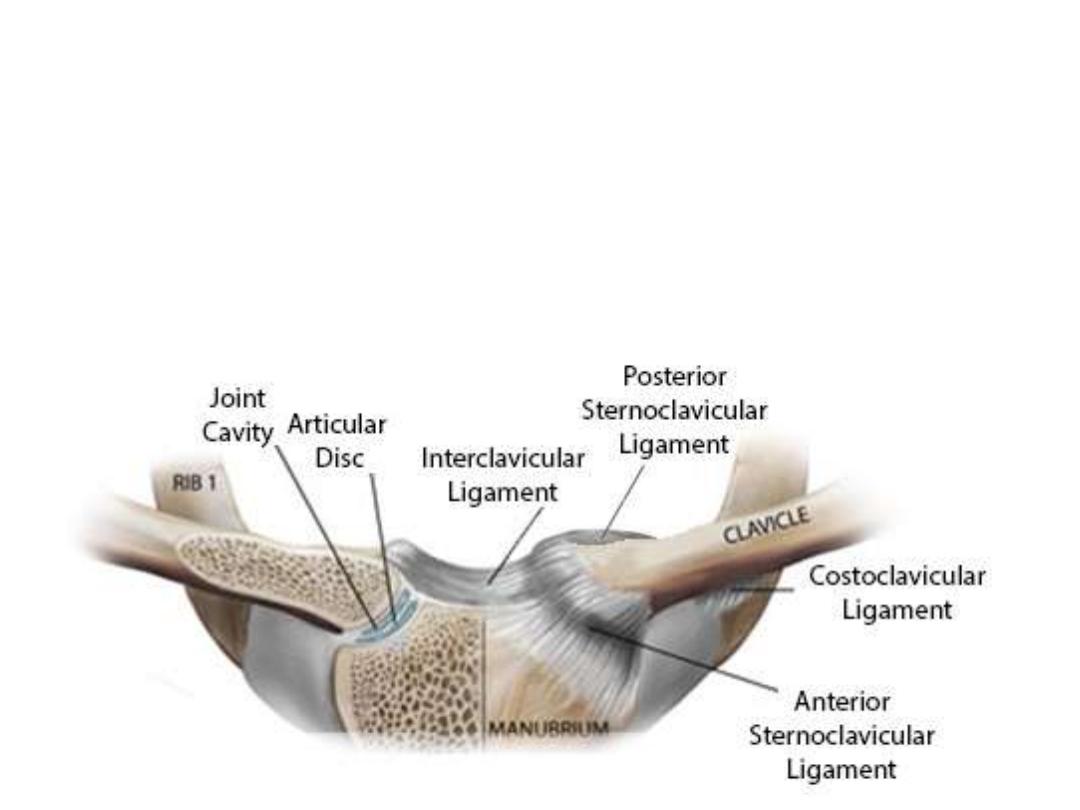
Ligaments:
•Anterior and posterior sternoclavicular ligaments are anterior and posterior,
respectively, to the joint;
•Interclavicular ligament links the ends of the two clavicles to each other
•Costoclavicular ligament is positioned laterally to the joint and links the
proximal end of the clavicle to the first rib and related costal cartilage.
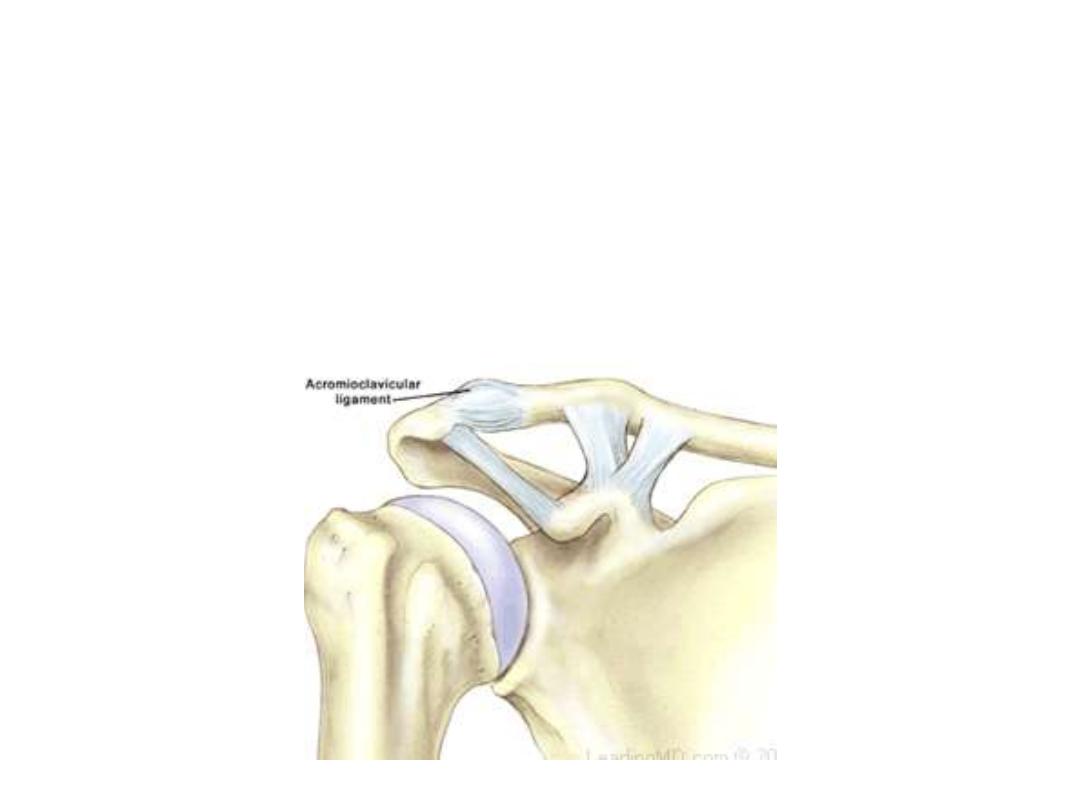
Acromioclavicular joint:
- A small synovial joint between the small oval facet on the medial surface of the
acromion and a similar facet on the acromial end of the clavicle.
- It allows movement in the anteroposterior and vertical planes together with
some axial rotation.
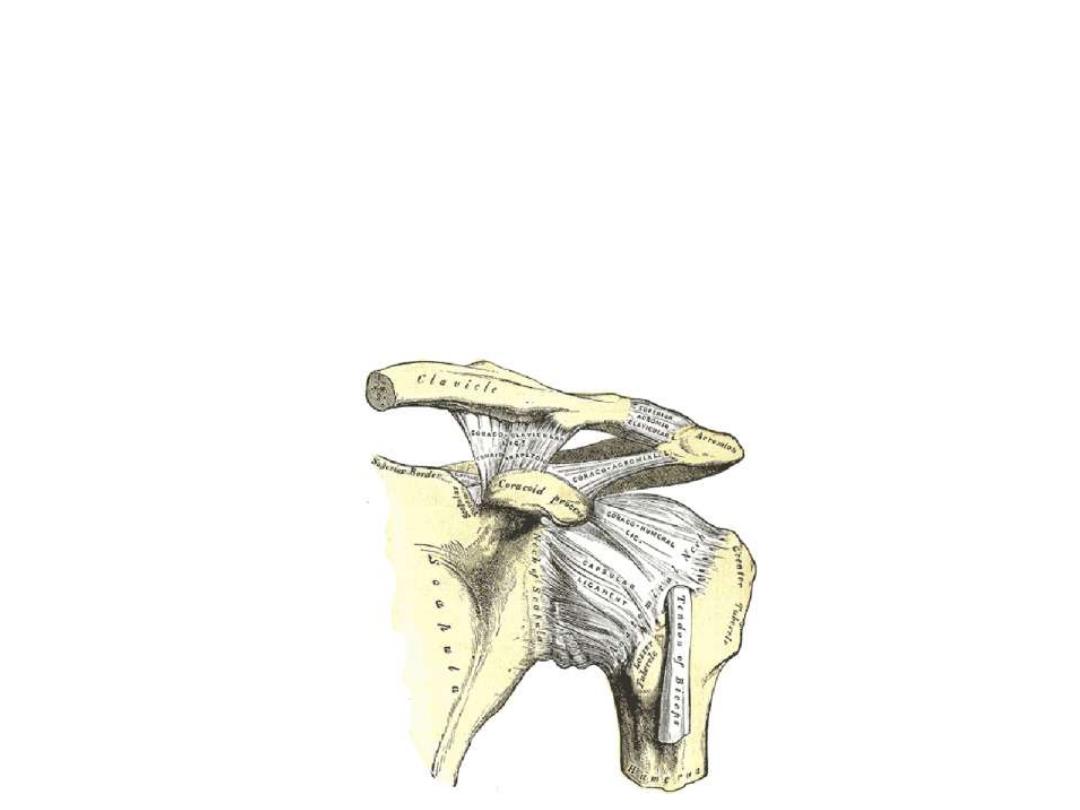
•The acromioclavicular joint is surrounded by a joint capsule and is reinforced
by a small acromioclavicular ligament superior to the joint
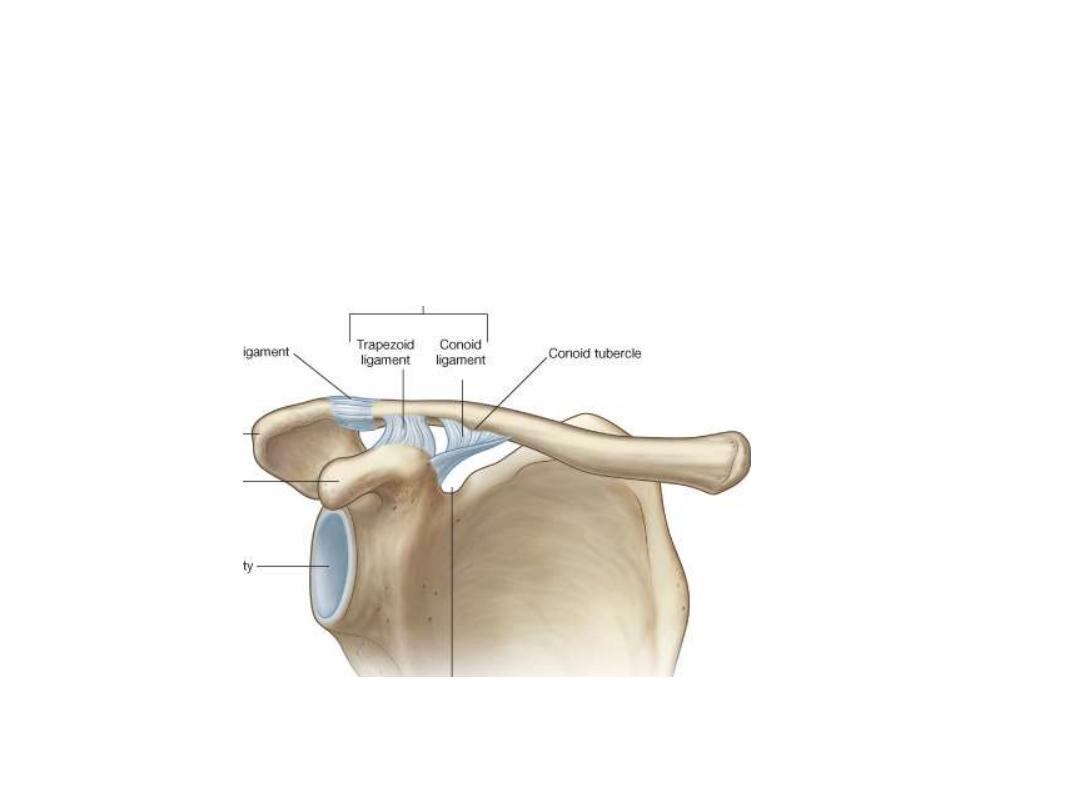
•A much larger coracoclavicular ligament, is an important strong accessory
ligament, providing much of the weight bearing support for the upper limb on
the clavicle and maintaining the position of the clavicle on the acromion &
comprises an anterior trapezoid and a posterior conoid ligaments (which
attaches to the related tubercles on the clavicle).
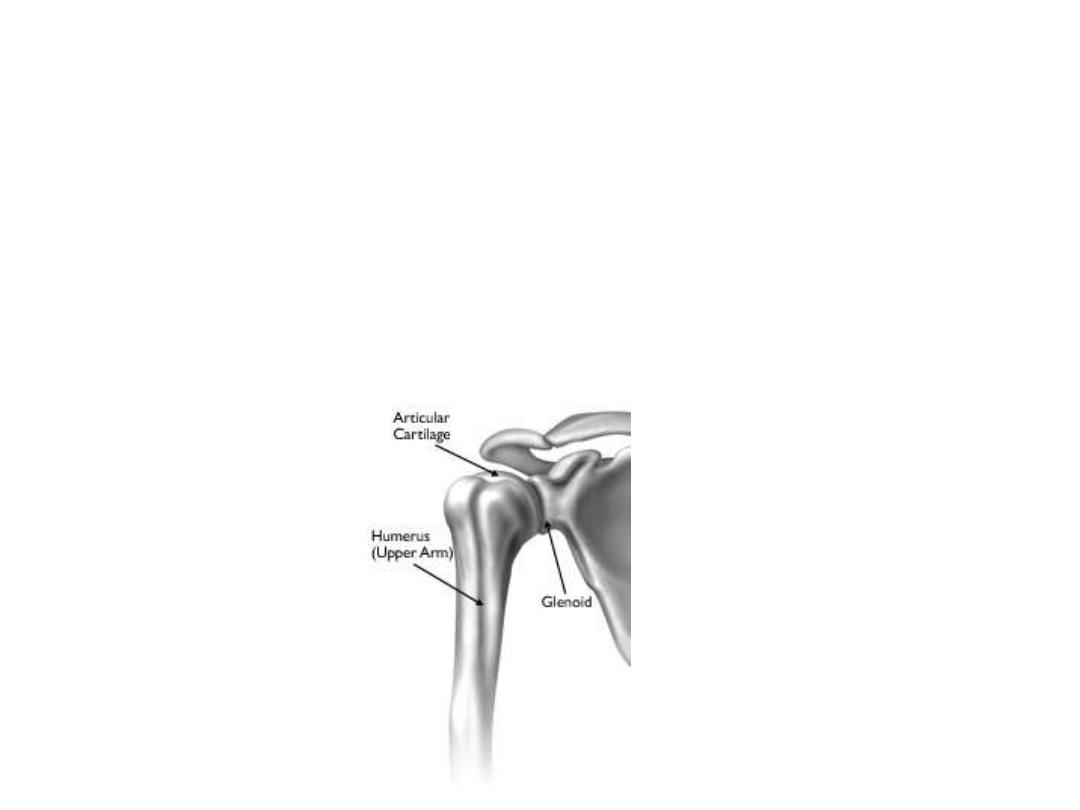
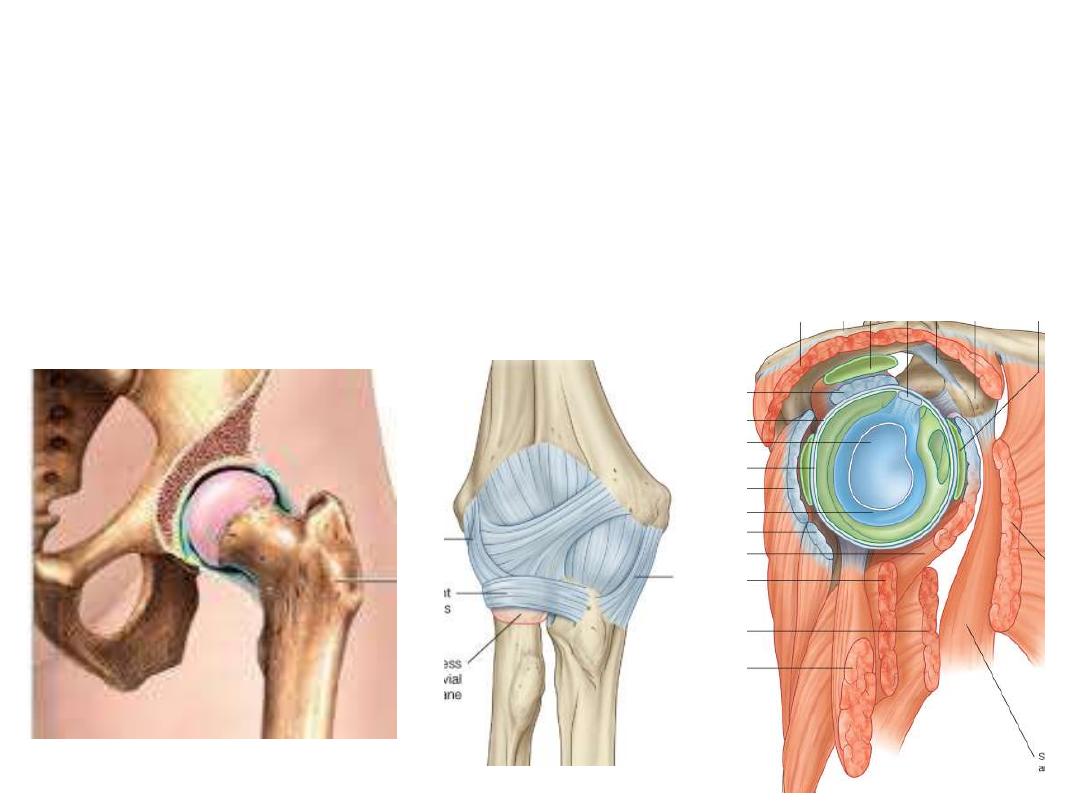
Glenohumeral joint:
-A synovial ball and socket articulation between the head of the humerus and the
glenoid cavity of the scapula.
-It is multiaxial with a wide range of movements provided at the cost of skeletal
stability.
-Joint stability is provided, instead, by the rotator cuff muscles, the long head of the
biceps and extracapsular ligaments.
-.
The articular surfaces:
• The large spherical head of the humerus
accounts three folds the area of the
small glenoid cavity of the scapula.
• Each of the surfaces is covered by
hyaline cartilage.
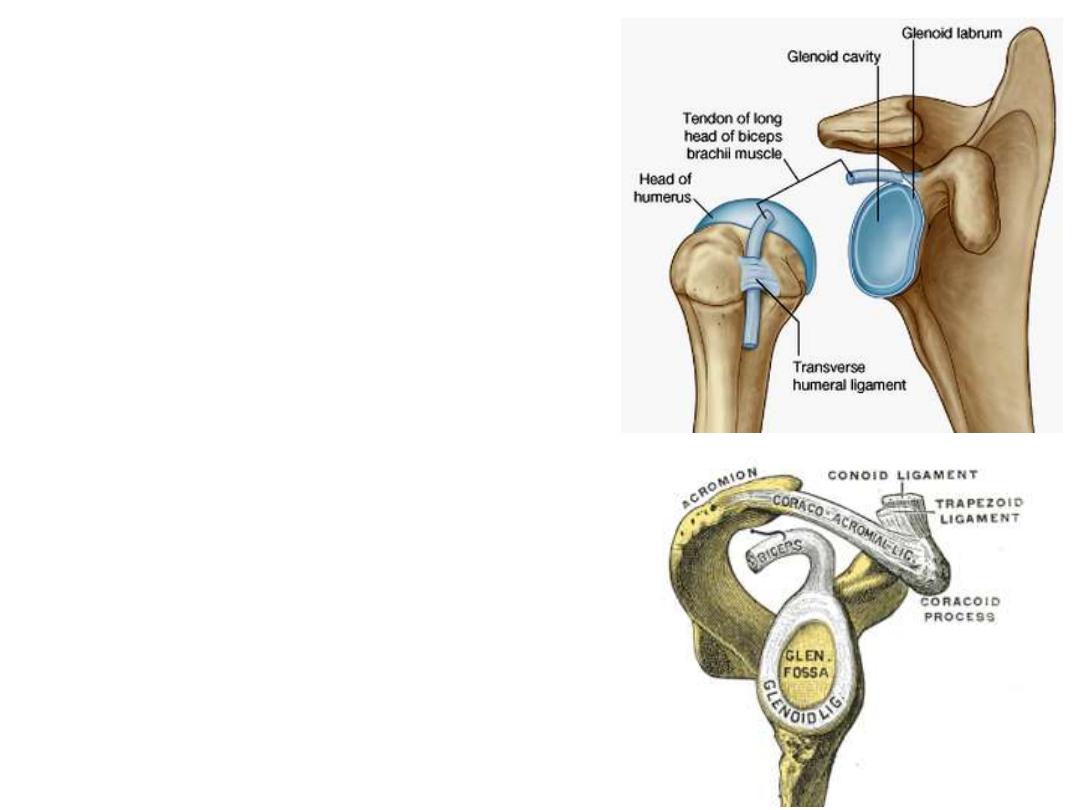
• The glenoid cavity is deepened and
expanded
peripherally
by
a
fibrocartilaginous collar (the glenoid
labrum), which attaches to the margin of
the fossa.
• Superiorly, this labrum is continuous
with the tendon of the long head of the
biceps brachii muscle, which attaches to
the supraglenoid tubercle and passes
through the articular cavity
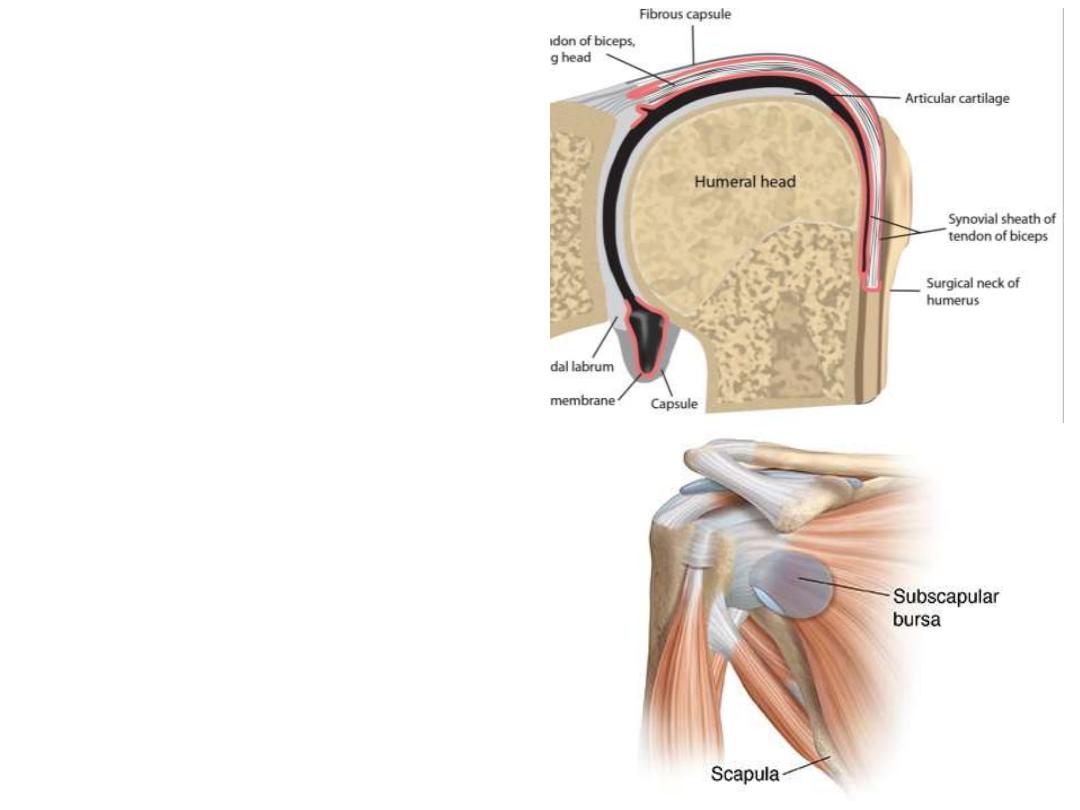
Synovial membrane:
-The synovial membrane attaches
to the margins of the articular
surfaces and lines the joint capsule
-It protrudes through apertures in
the fibrous membrane to form
bursae, which lie between the
tendons of surrounding muscles
and the fibrous membrane.
-The most consistent is the bursa of
subscapularis, which lies between
the subscapularis muscle and the
capsule.
The fibrous membrane (capsule):
• The capsule attaches to the
margin of the glenoid cavity,
outside the attachment of the
glenoid labrum and the long head
of the biceps brachii, and to the
anatomical neck of the humerus
• On the humerus, the medial
attachment occurs more inferiorly
& more loose to accommodates
abduction of the arm
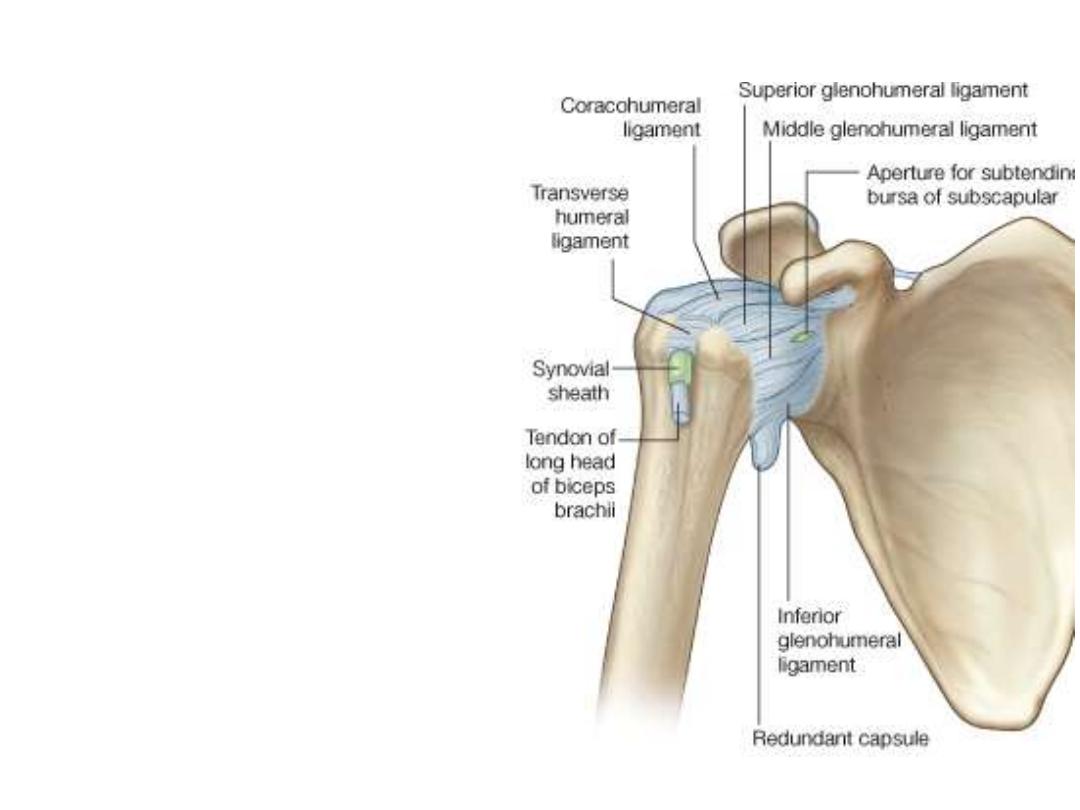
Ligaments:
•The joint capsule is thickened anterosuperiorly in three locations to form superior,
middle, and inferior
glenohumeral ligaments
, which pass between the superomedial
margin of the glenoid cavity to the lesser tubercle & anatomical neck of the humerus
•Coracohumeral ligament
lies superiorly between the base of the coracoid process
and the greater tubercle
•Transverse humeral ligament
lies between the greater and lesser tubercles of the
humerus
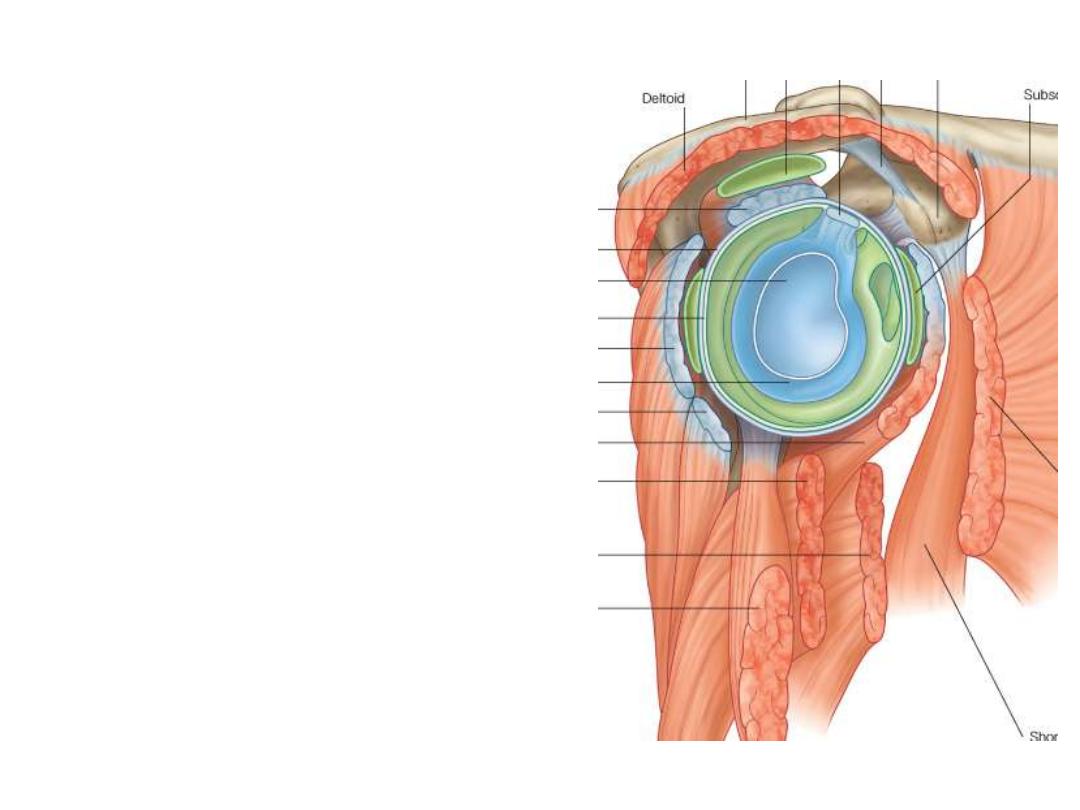
The surrounding muscles:
• Tendons of the rotator cuff muscles (the
supraspinatus,
infraspinatus,
teres
minor, and subscapularis muscles)
blend with the joint capsule & form a
collar that surrounds the joint except
inferiorly
• This cuff holds the head of the humerus
in the glenoid cavity of the scapula
without
compromising
the
arm's
flexibility and range of motion.
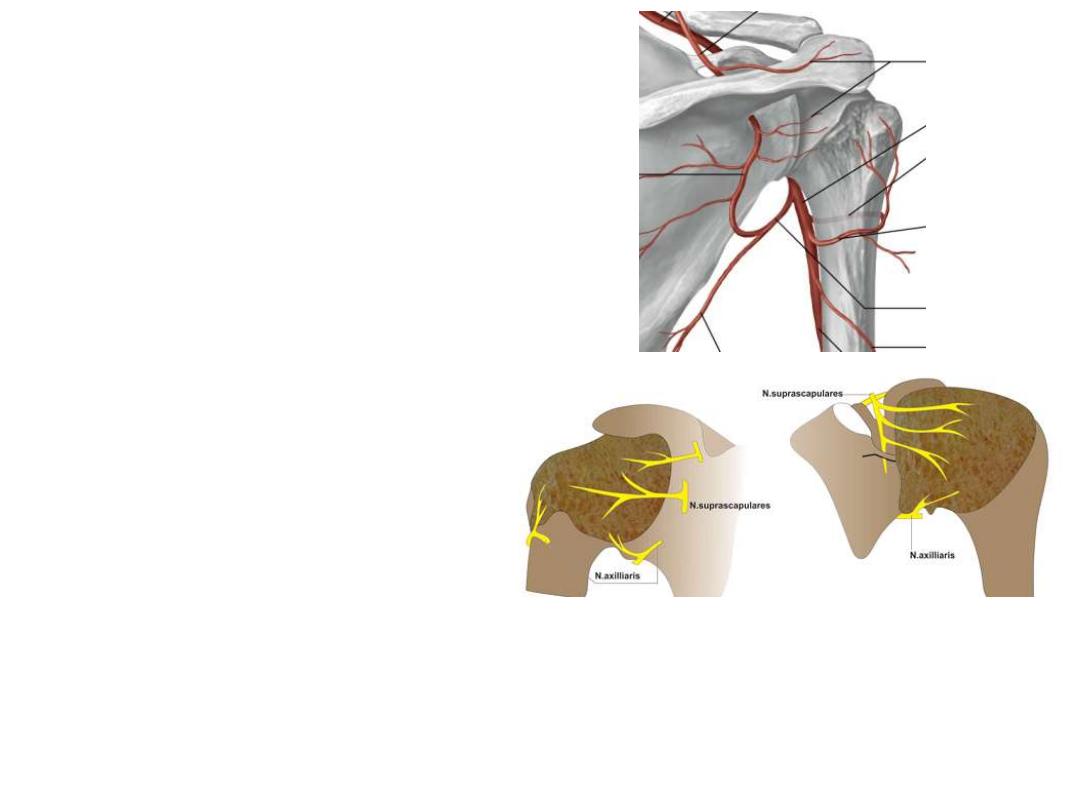
Blood supply:
Branches of the anterior and posterior
circumflex humeral and suprascapular
arteries.
Innervation:
• Posterior cord of the brachial plexus
• Suprascapular n
• Axillary n
• Lateral pectoral n
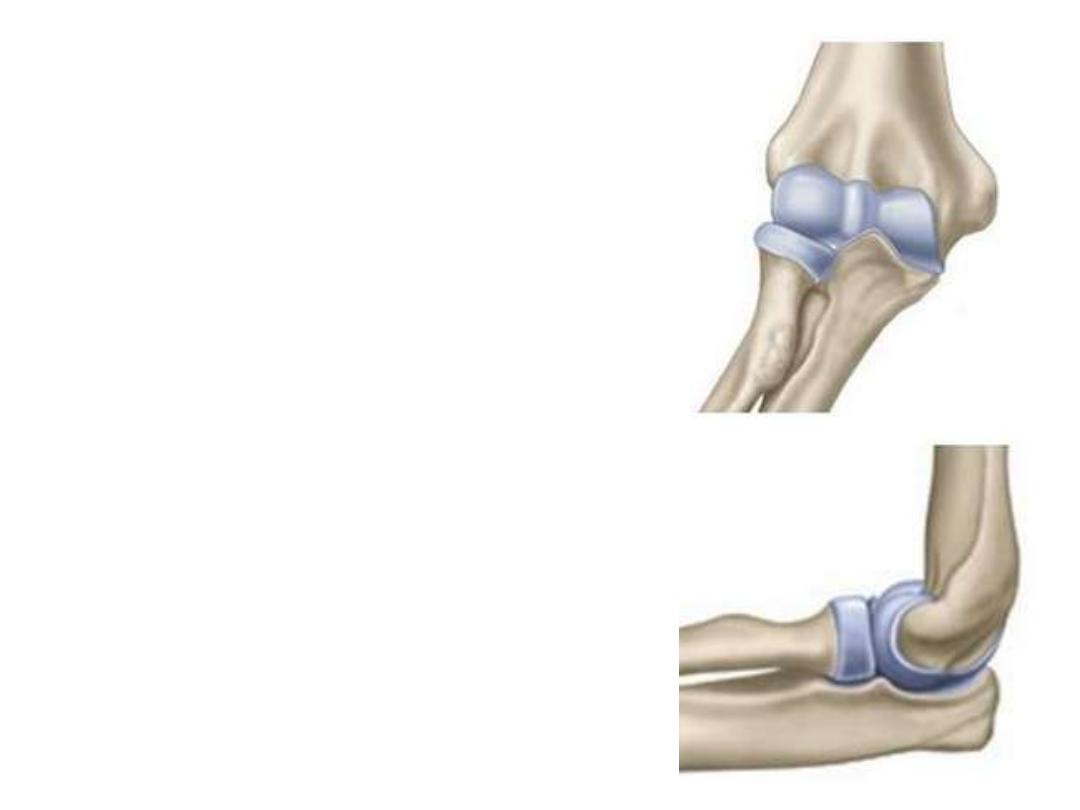
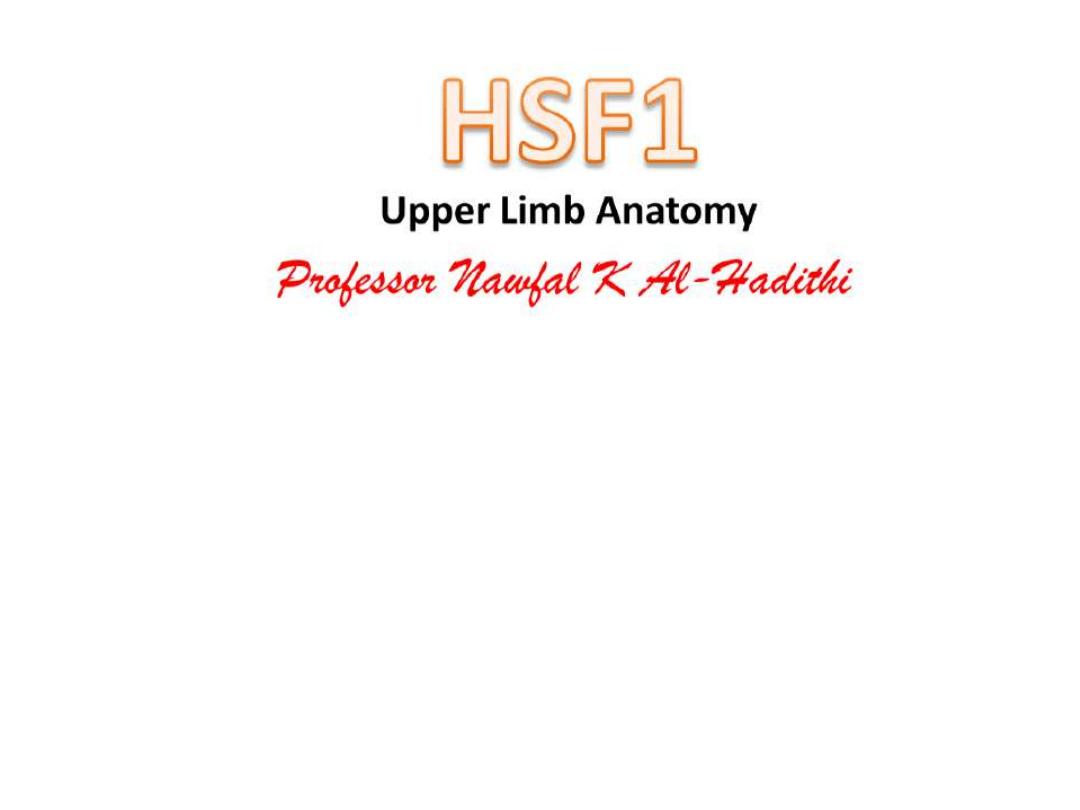
The elbow joint:
A complex joint involving three separate
articulations, which share a common
synovial cavity:
1- The joints between the trochlear notch of
the ulna and the trochlea of the humerus
2- The joint between the head of the radius
and the capitulum of the humerus
These two joints are primarily involved with
hinge-like flexion-extension of the forearm
on the arm & represent the principal elbow
joint.
3- The joint between the head of the radius
and the radial notch of the ulna (proximal
radio-ulnar joint) is involved with pronation
and supination of the forearm
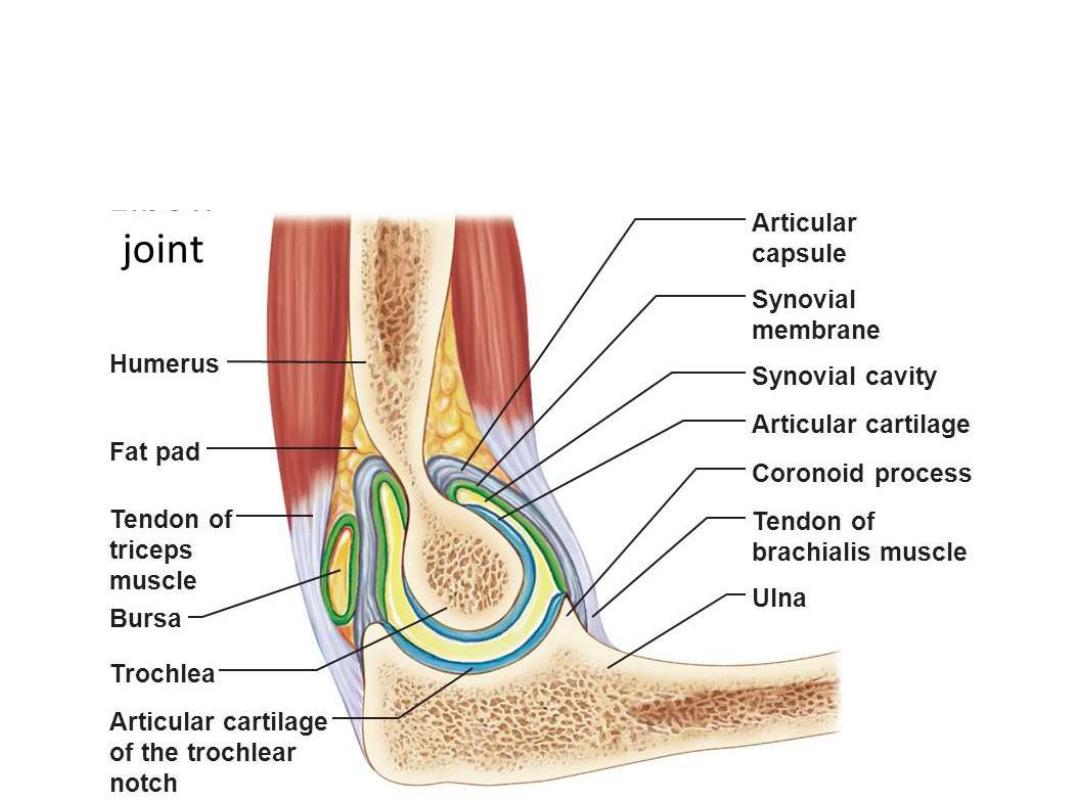
• Articular surfaces of the bones are covered with hyaline cartilage
• Synovial membrane originates from the edges of the articular cartilage and
lines the deep surface of the joint capsule & all capsular contents apart
from the articular surfaces
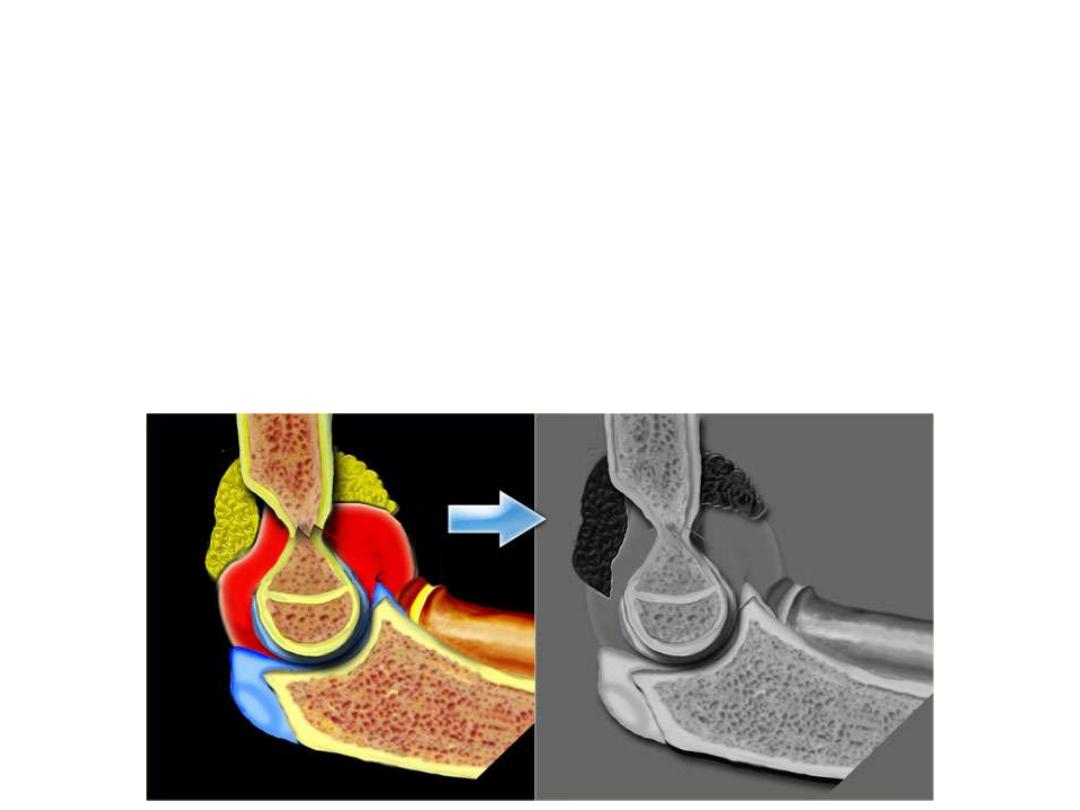
-The synovial membrane is separated from the capsule by pads of fat in
regions overlying the coronoid fossa, the olecranon fossa, and the radial
fossa.
-These fat pads accommodate the articular parts during extension and flexion
of the elbow.
-Attachments of the brachialis and triceps to the joint capsule overlying these
regions pull these pads out of the way when the adjacent bony processes are
moved into the fossae
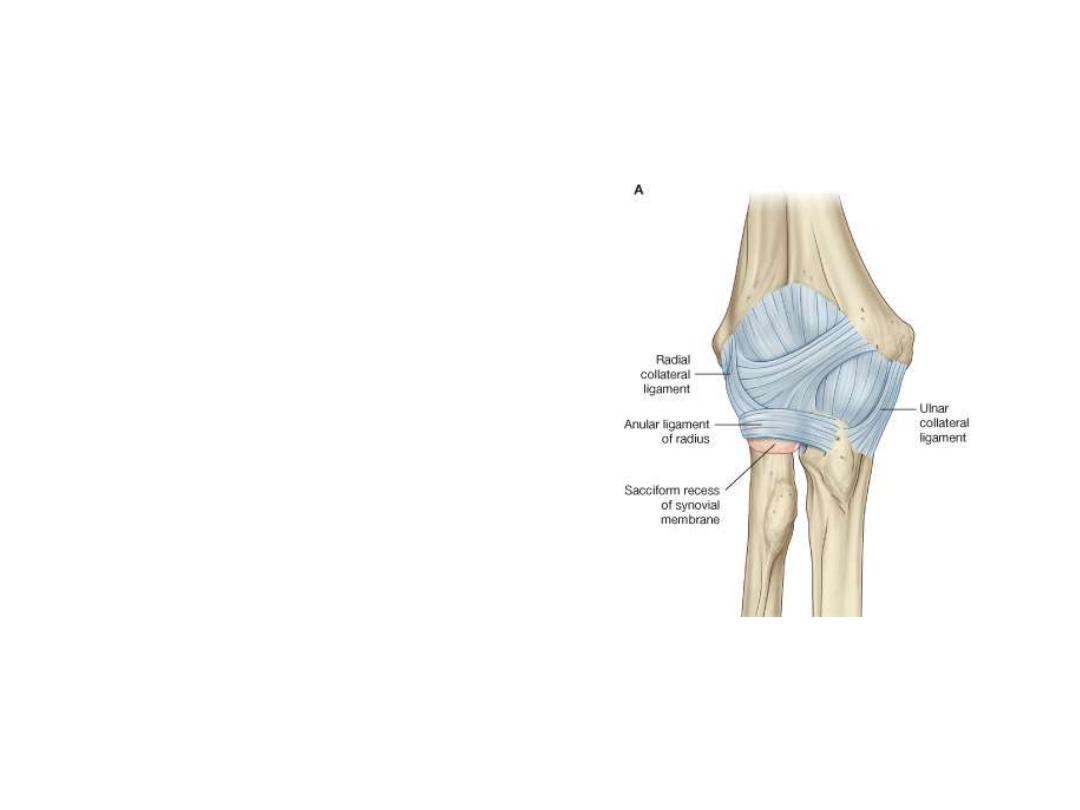
Ligaments:
1- Medial & lateral collateral ligaments:
thickenings in the fibrous membrane
to support the flexion and extension
movements
2- Annular ligament:
the joint capsule
is reinforced laterally where it cuffs the
head of the radius with a strong
annular ligament which separates from
the capsule posteriorly.
The anular ligament of radius and
related joint capsule allow the radial
head to slide against the radial notch
of the ulna and pivot on the capitulum
during pronation and supination.
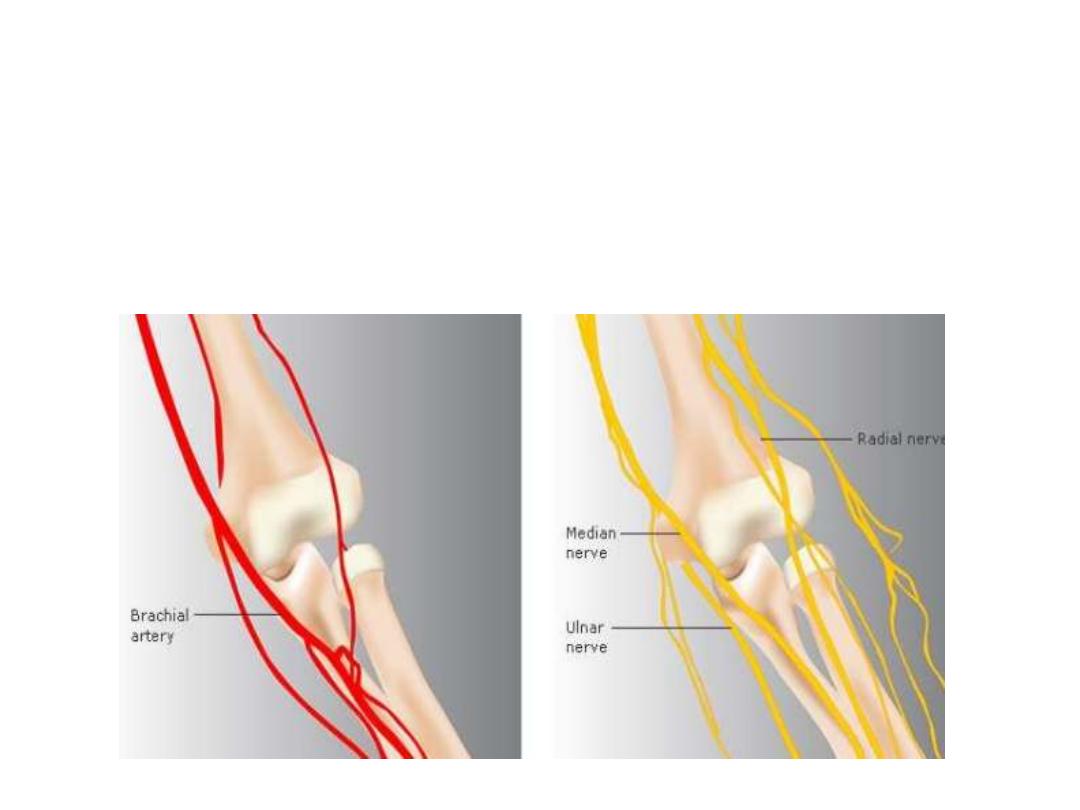
Vascular supply:
Anastomosis around the elbow
Innervation:
Predominantly by branches of the radial and musculocutaneous nerves.
There may be some innervation by branches of the ulnar and median nerves
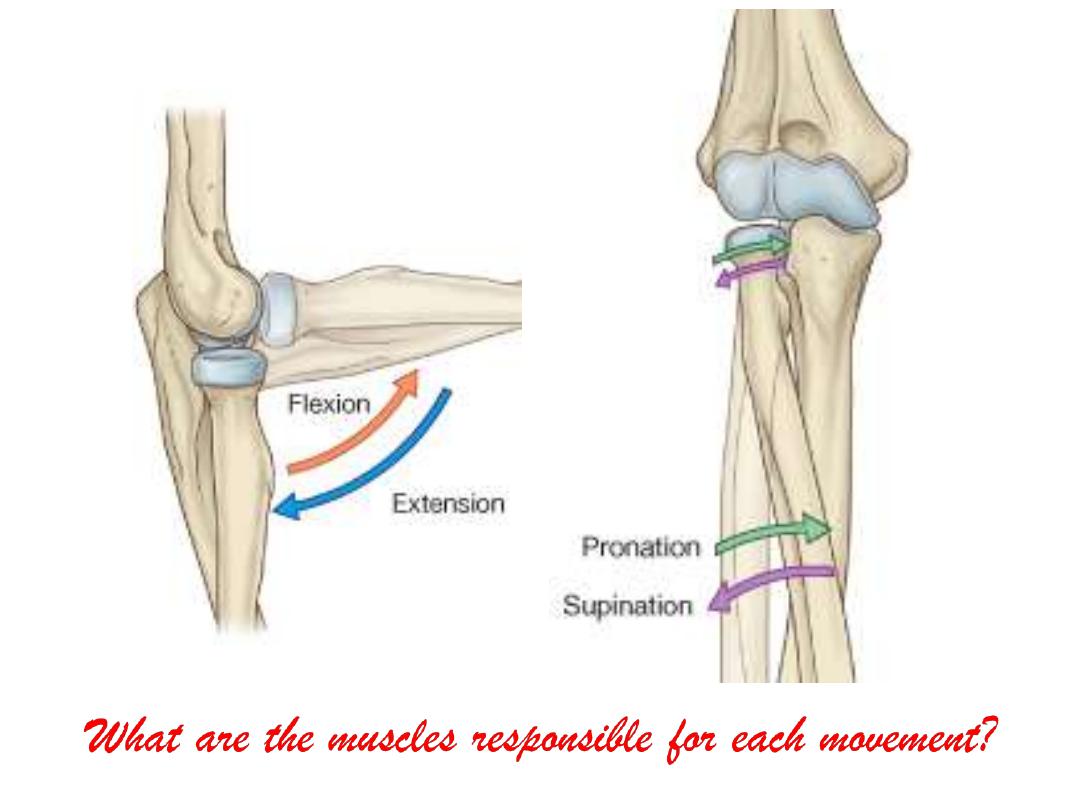
Basic movements of the elbow:
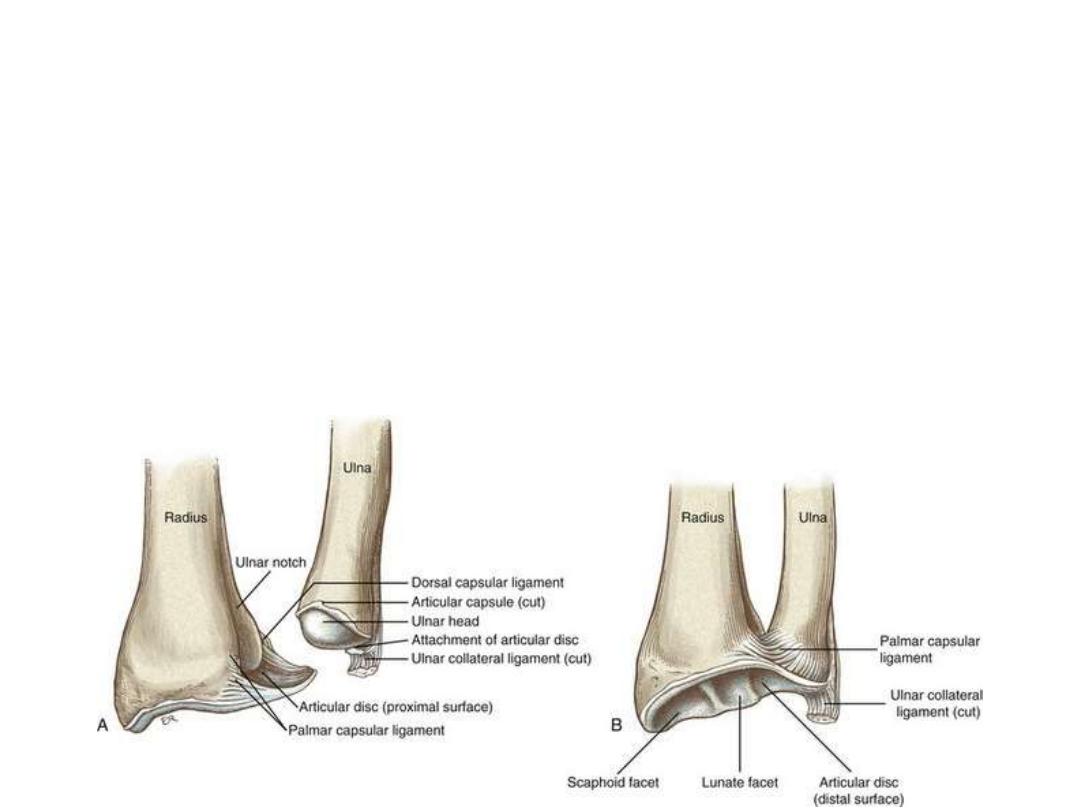
The distal radio-ulnar joint:
-Occurs between the head of the ulna with the ulnar notch of the radius, and with a
fibrous articular disc, which separates the joint from the wrist joint
- The articular disc is attached by its apex to the ulna & by its base to the angular
margin of the radius near the ulnar notch
-Synovial membrane is attached to the margins of this joint and is covered on its
external surface by a fibrous joint capsule
-The distal radio-ulnar joint allows the distal end of the radius to move
anteromedially over the ulna
Wrist joint :
In anatomy the wrist includes:
• Inferior RUJ
• Radiocarpal J
• Intercarpal J
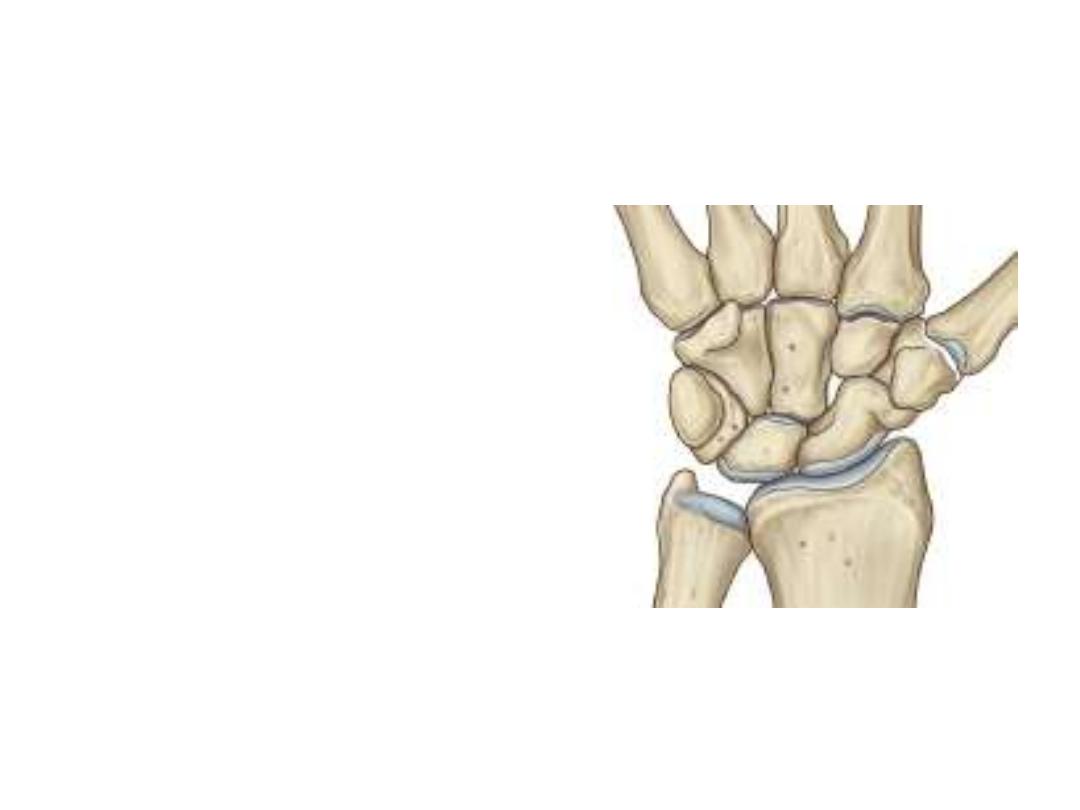
The radiocarpal joint:
-Is a synovial joint between the distal end of
the radius and the articular disc overlying
the scaphoid & lunate bones
-The articular surfaces of the carpals form
an oval shape with a convex contour, which
articulates with the corresponding concave
surface of the radius and articular disc
-The wrist joint allows movement around
two axes (abduction-adduction & flexion-
extension)
-Because the radial styloid process extends further distally than does the
ulnar styloid process, the hand can be adducted to a greater degree than it
can be abducted
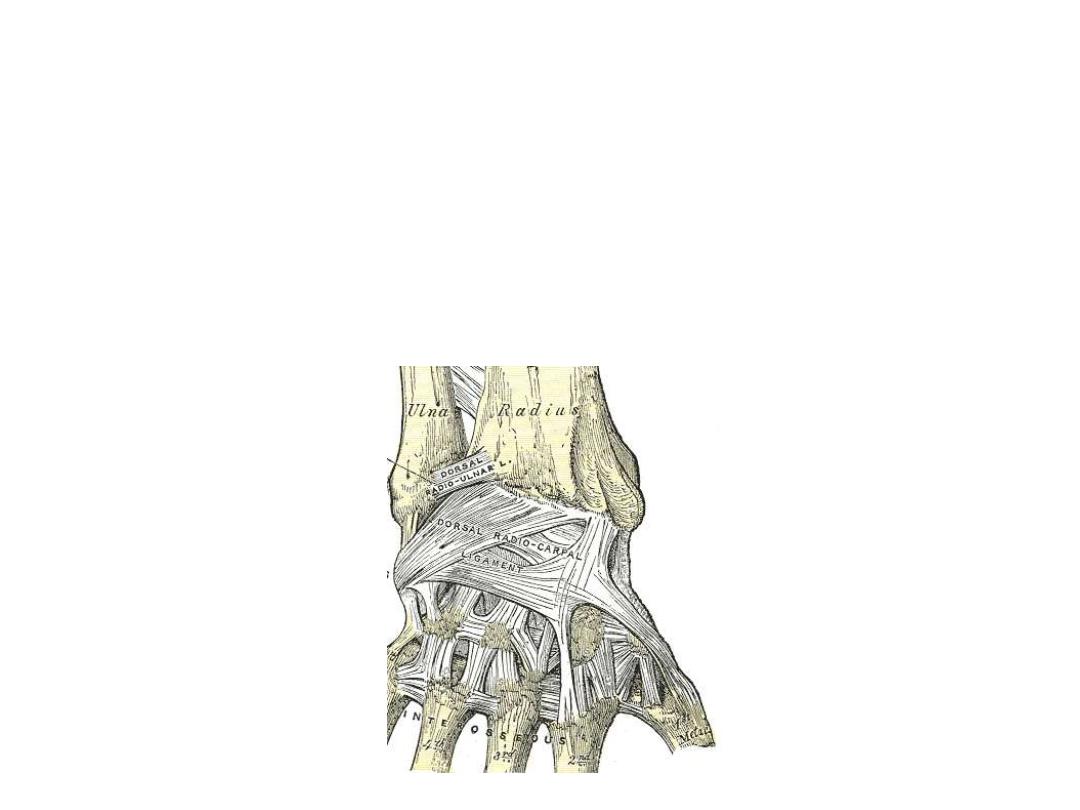
-The capsule of the wrist joint is reinforced by radiocarpal & ulnocarpal
ligaments
-Radial and ulnar collateral ligaments span the distance between the styloid
processes of the radius and ulna and the adjacent carpal bones.
Carpal joints:
-The synovial joints between the carpal bones share a common articular
cavity.
-The joint capsule of the joints is reinforced by numerous ligaments.
-Although movement at the carpal joints (intercarpal joints) is limited, they do
contribute to the positioning of the hand in abduction, adduction, flexion,
and, particularly, extension.
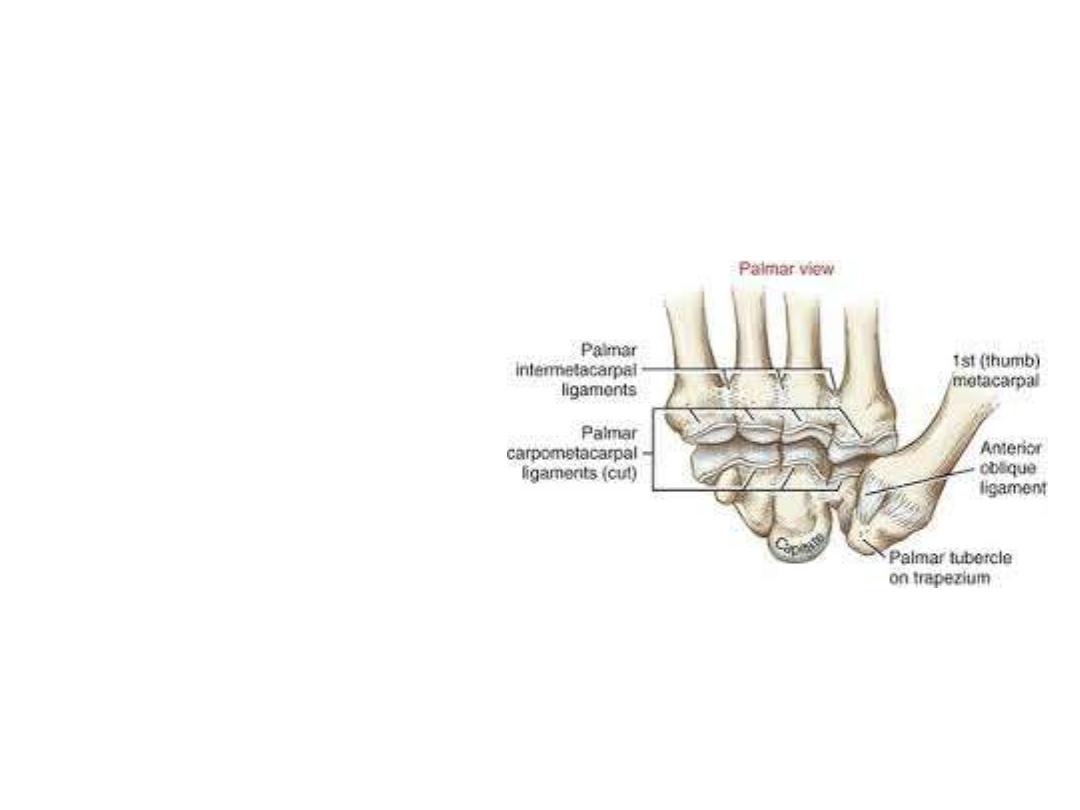
Carpometacarpal joints:
-Are 5 in number
-The
saddle
joint
between
metacarpal I and the trapezium,
imparts a wide range of mobility
to the thumb
-Other CMCJ are much less
mobile allowing only limited
gliding movements
-Movement
of
the
joints
increases medially so metacarpal
V slides to the greatest degree
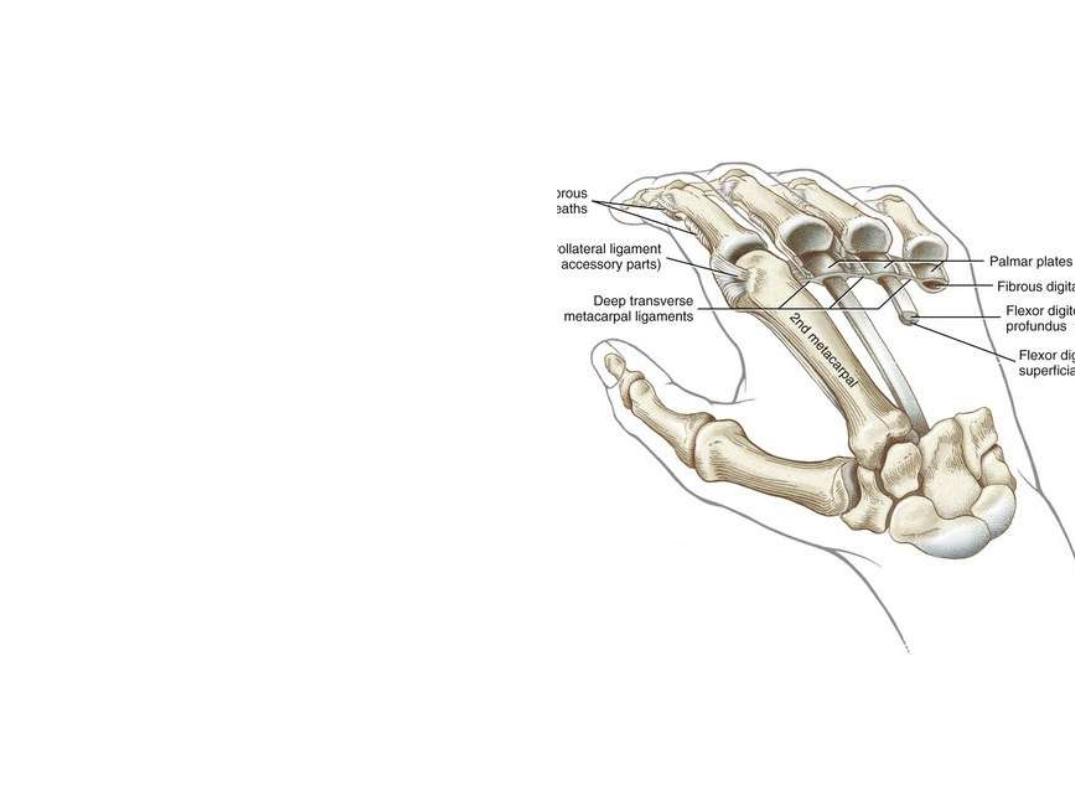
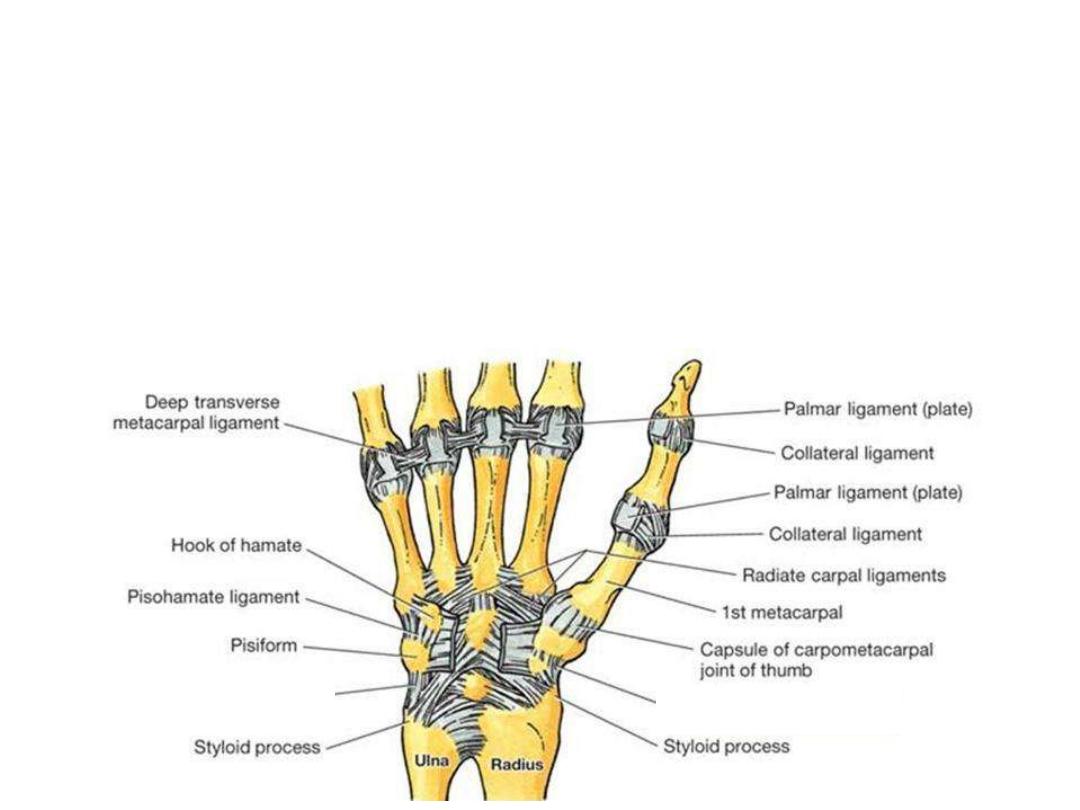
Metacarpophalangeal joints:
-These are condylar joints, which allow
all movements except rotation
- The capsule of each joint is reinforced
by the palmar ligament and by medial
and lateral collateral ligaments
-The three deep transverse metacarpal
ligaments
connecting
the
palmar
ligaments of these joints to each other
-The absence of this ligament, and the
presence of a saddle joint between
metacarpal I and the trapezium, are
responsible for the increased mobility of
the thumb

Interphalangeal joints:
-The interphalangeal joints of the hand are hinge joints that allow mainly
flexion and extension.
-They are reinforced by medial and lateral collateral ligaments and palmar
ligaments.