1
Turner's syndrome
Turner's syndrome (45, X):
Usually
(>95%) this results in early miscarriage.
In live-born females, the incidence is about 1 in 2500.
Short stature may be the only clinical abnormality in children
.
Clinical features:
In the newborns:
o
SGA.
o
Webbing of the neck.
o
Protruding malformed ears.
o
Lymphedema of the hands and feet.
o
Although many newborns are phenotypically normal.
Older children and adults:
o
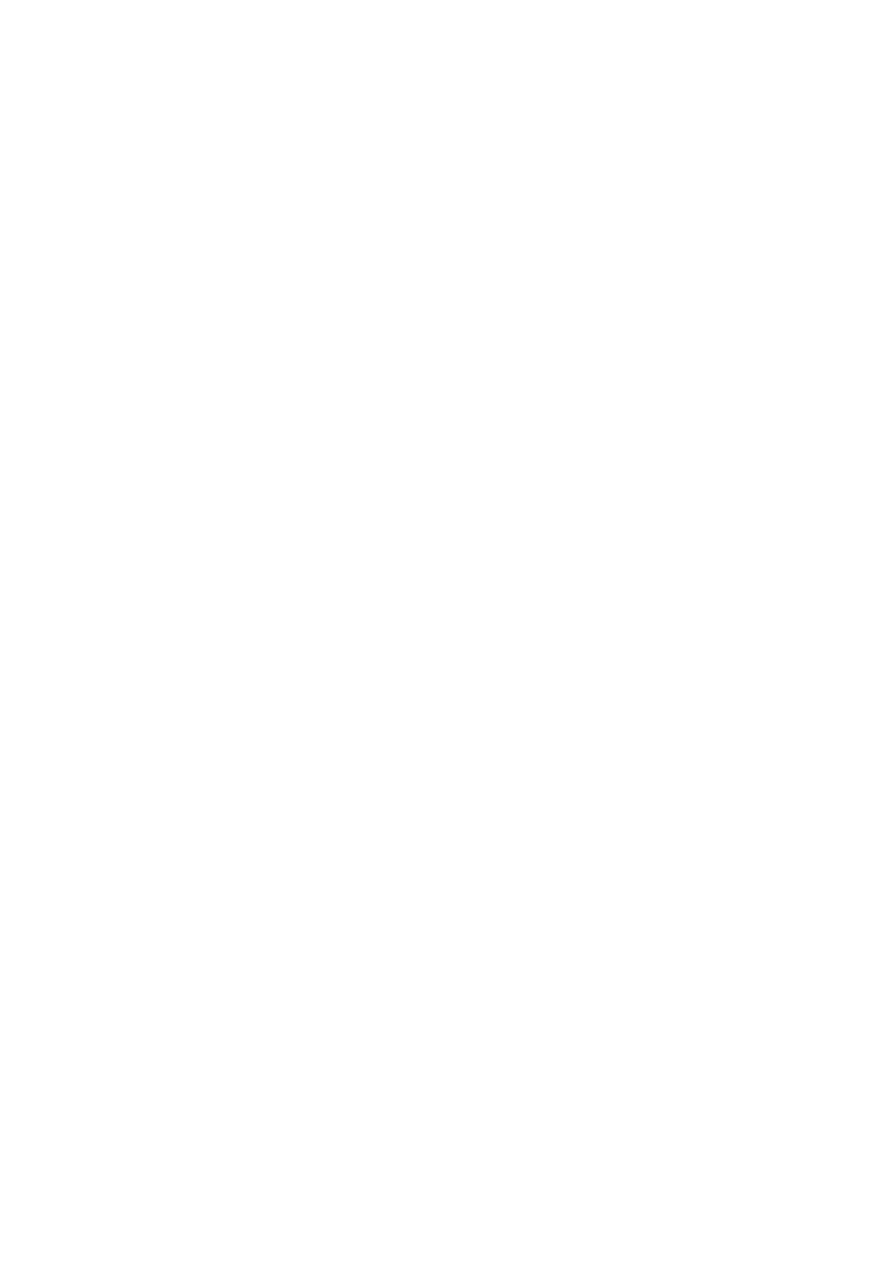
Short stature - cardinal feature (SS may be the only clinical abnormality in children).
o
Neck webbing or thick neck.
o
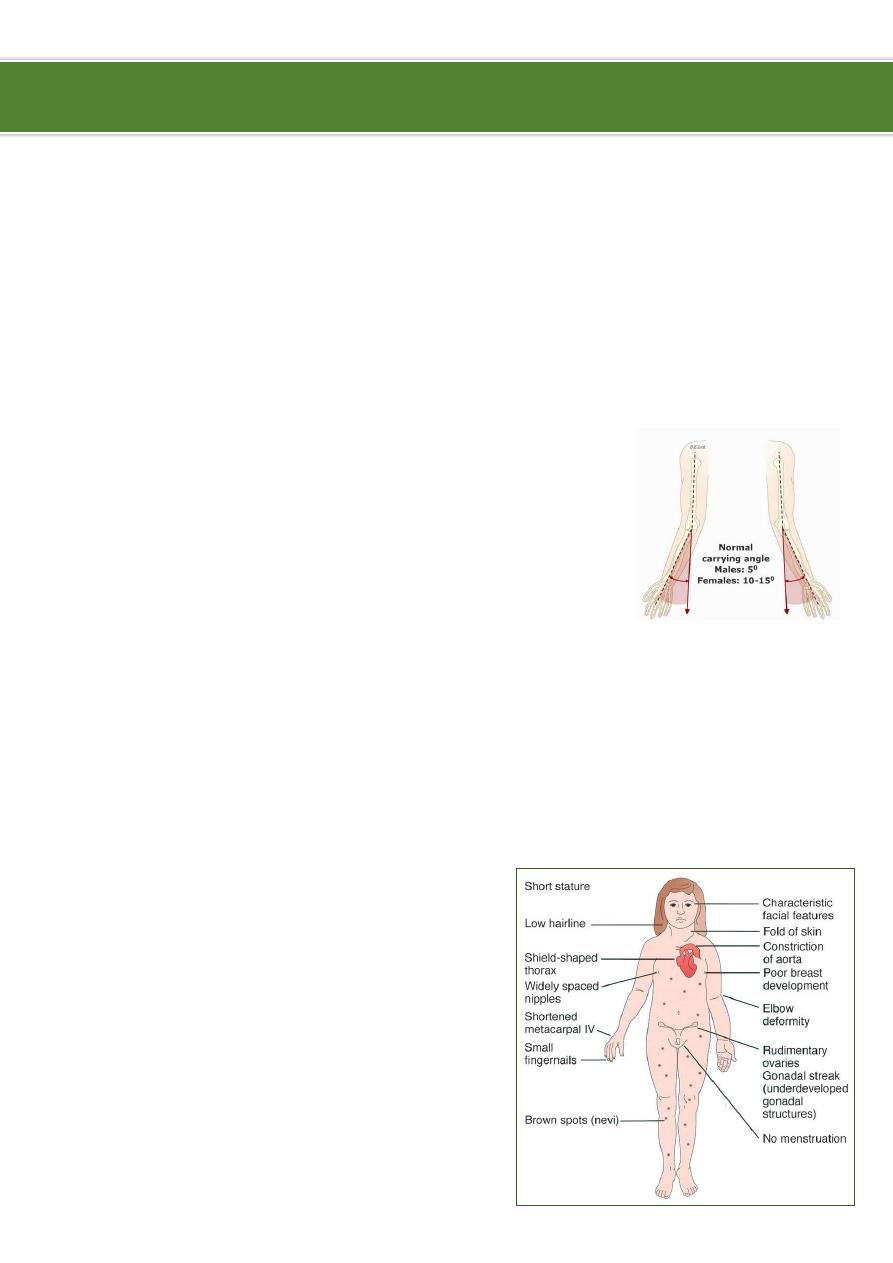
Wide carrying angle (cubitus valgus).
o
Widely spaced nipples.
o
Congenital heart defects (particularly coarctation of the aorta).
o
Delayed puberty.
o
Ovarian dysgenesis resulting in infertility, although pregnancy may be possible with
in-vitro fertilisation (IVF) with donated ova.
o
Hypothyroidism.
o
Renal anomalies.
o
Pigmented moles.
o
Recurrent otitis media.
o
Most patients tend to be of normal
intelligence, but intellectual disability is
seen in up to 6% of affected children.
Ibnlatef
Notes
Pediatrics
2
Management:
Medical Care
o
Turner syndrome is a lifelong condition.
o
Health supervision involves careful medical follow-up care, which includes
screening for commonly associated chronic diseases.
o
Early preventive care and treatment are also essential.
o
In childhood, growth hormone therapy is standard to prevent short stature as an
adult.
o
Estrogen replacement for development of secondary sexual characteristics at
the time of puberty (but infertility persists).
o
Androgen replacement therapy is not the standard of care, but may have favorable
effects.
Surgical care:
o
Patients are suspected of having a high risk of keloid formation.
o
Subacute bacterial endocarditis (SBE) prophylaxis may be required prior to any
dental or surgical procedure in women with cardiac valve disease to prevent SBE.
Consultations:
o
Endocrinologist:
Growth and development, thyroid status, and osteoporosis prevention with
growth hormone, estrogens, and progestins.
Patients on growth hormone should be seen every 3-6 months.
o
Cardiologist:
Patients with systemic hypertension or aortic valve anomalies are at higher risk
for aortic dissection.
Patients found to have significant anomalies should have long-term follow-up
care and possibly SBE prophylaxis.
Because of the risks of aortic root dilatation and mortality due to aortic
dissection, cardiac evaluation (including echocardiography) may be worthwhile
every 5 years, even in patients with normal findings on initial cardiovascular
examination.
Patients contemplating pregnancy should have a complete cardiovascular
evaluation prior to attempting assisted reproduction or conception.
Patients with a bicuspid aortic valve, coarctation of the aorta, or dilation of the
aorta have a higher risk of dissecting aortic aneurysm or rupture.
o
Nephrologist or urologist:
Almost a third of patients have renal anomalies that may require evaluation and
follow-up care by a nephrologist.
At a minimum, such patients should have a yearly urine culture and an annual
measurement of BUN and creatinine levels.
Girls with horseshoe kidneys have an increased risk of Wilms tumor.

3
Patients with horseshoe kidneys should have renal ultrasound examinations
every 4-6 months until the age 8 years and every 6-12 months thereafter.
o
Psychologist:
Overall psychological health is good, but specific perceptual weaknesses or
learning disabilities may be present.
Assessment of intelligence, learning ability, motor skills, and social maturity
should be made prior to enrollment in kindergarten.
Problems with math and with visual spatial skills (eg, map reading) are common.
Attention deficit hyperactivity disorder is more common in girls with Turner
syndrome than in girls in general.
Intelligence is usually normal, but individuals with ring chromosomes may have
impaired intelligence.
As with any chronic illness, attention should be paid to fostering healthy
socialization and to appropriate career and vocational planning.
Patients with Turner syndrome are more likely to be employed than other adult
women, although less likely to be married.
o
Genetics:
Turner syndrome is not an inherited disorder, and the recurrence risk is low.
Because of infertility, the syndrome is rarely passed to offspring.
Consultation is helpful when the condition is diagnosed in utero or when Turner
syndrome is suspected in the setting of a normal peripheral blood karyotype.
Patients should be tested for the presence of Y-chromosomal material using a Y-
centromeric probe.
Diet:
o
Dietary requirements are similar to those of other children or adults.
o
Both short stature and ovarian failure are risk factors for osteoporosis, and care
should be taken to ensure adequate daily intake of calcium (1.0-1.5 g) and vitamin
D (at least 400 IU).
o
Patients should avoid obesity because it increases already high risks of
hypertension and insulin resistance.
o
Patients with short stature require fewer calories than those of normal height.
Activity
o
Physical activity should be encouraged as prevention for obesity and osteoporosis.
o
Eligibility for competitive sports should be established by a cardiologist after a
comprehensive evaluation.
----------------------------------------------------------------------------------------------
www.facebook.com/ibnlatef
https://goo.gl/RpvNsl