1
Dehydration
The following children are at increased risk of dehydration:
Infants, particularly those under 6 months of age or those born with low birthweight.
If they have passed ≥6 diarrheal stools in the previous 24 h.
If they have vomited three or more times in the previous 24 h.
If they have been unable to tolerate (or not been offered) extra fluids.
If they have malnutrition.
Infants are at particular risk of dehydration:
They have a greater surface area to weight ratio than older children, leading to greater
insensible water losses.
They have higher basal fluid requirements (100–120 ml/kg per day, i.e. 10–12% of
bodyweight).
They have immature renal tubular reabsorption.
They are unable to obtain fluids for themselves when thirsty.
Investigations:
Usually, no investigations are indicated.
Stool culture is required if the child appears septic, if there is blood or mucus in the
stools or the child is immunocompromised, it may be indicated following recent
foreign travel, if the diarrhea has not improved by day 7 or the diagnosis is uncertain.
Plasma electrolytes, urea, creatinine and glucose should be checked if intravenous
fluids are required or there are features suggestive of hypernatremia.
Blood culture when antibiotics are started.
Ibnlatef
Notes
Pediatrics
2
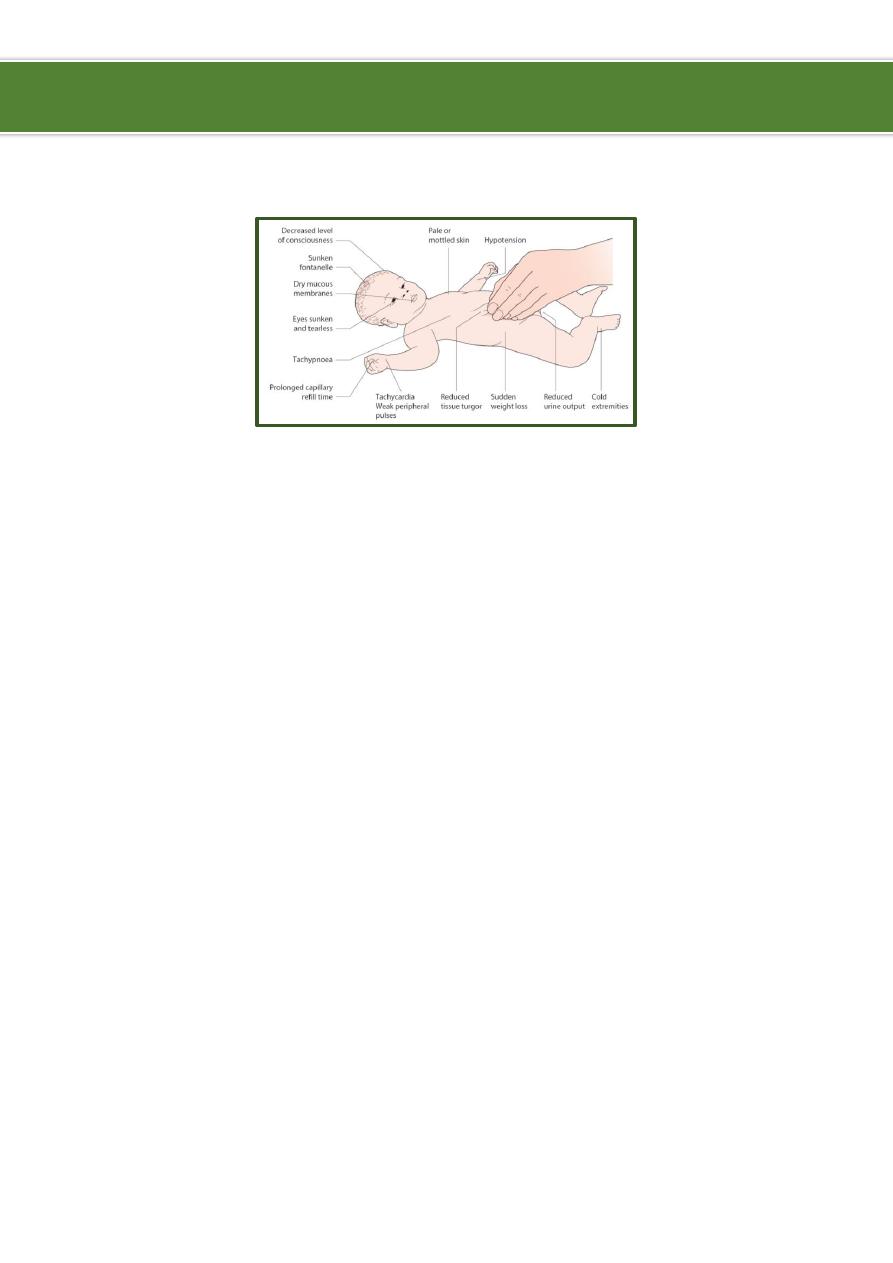
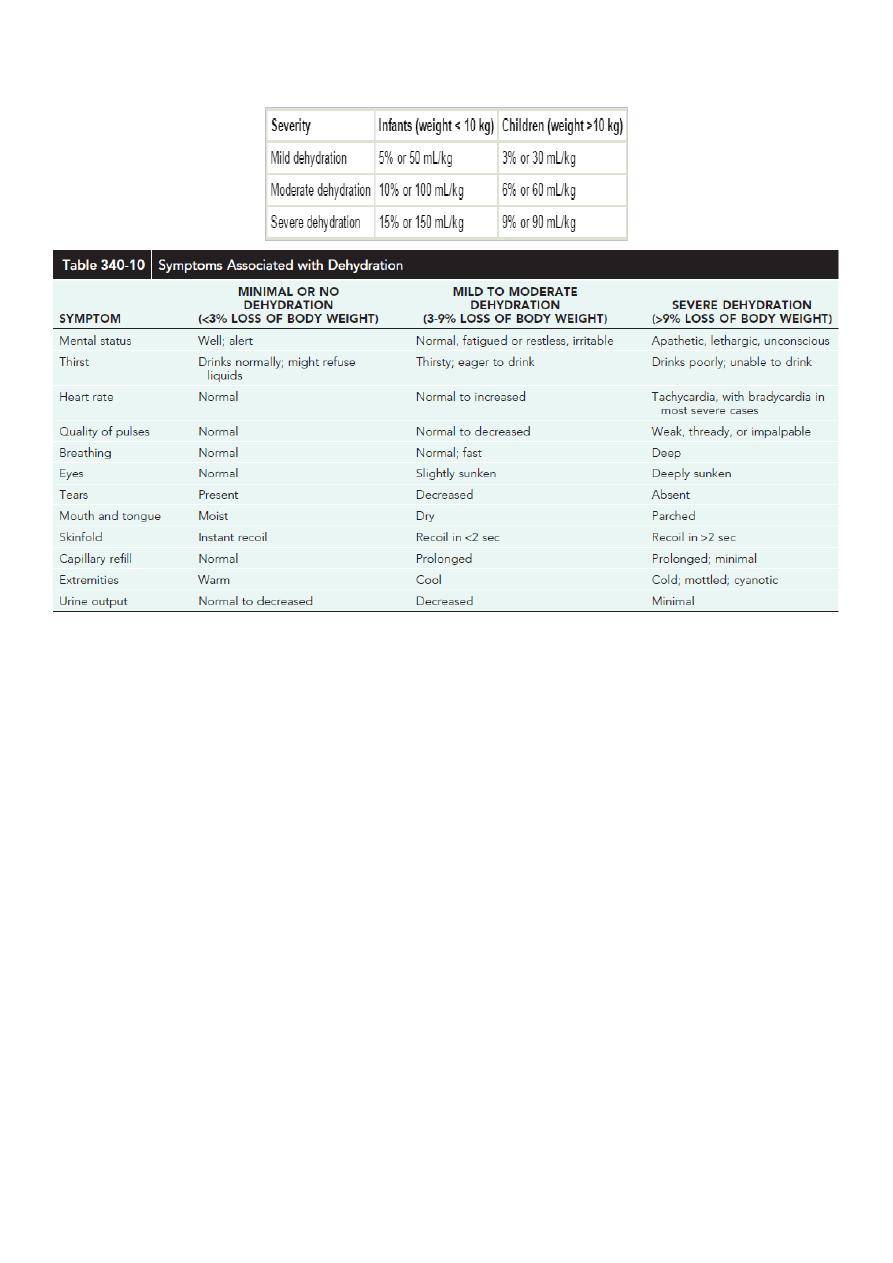
Clinical assessment of dehydration:
Oral rehydration solution (OSR):
The low-osmolality World Health Organization (WHO) oral rehydration solution (ORS)
containing 75 mEq of sodium, 64 mEq of chloride, 20 mEq of potassium, and 75 mmol
of glucose per liter, with total osmolarity of 245 mOsm/L.
It is now the global standard of care and more effective than home fluids, including
decarbonated soda beverages, fruit juices, and tea. These are not suitable for
rehydration or maintenance therapy because they have inappropriately high
osmolalities and low sodium concentrations.
Oral rehydration should be given to infants and children slowly, especially if they have
emesis.
It can be given initially by a dropper, teaspoon, or syringe, beginning with as little as 5
mL at a time, the volume is increased as tolerated.
Oral rehydration can also be given by a nasogastric tube if needed, this is not the usual
route.
Limitations to oral rehydration therapy include shock, an ileus, intussusception,
carbohydrate intolerance (rare), severe emesis, and high stool output (>10 mL/kg/hr).
Mild to moderate dehydration from diarrhea of any cause can be treated effectively
using a simple, oral rehydration solution (ORS) containing glucose and electrolytes.

3
The ORS relies on the coupled transport of sodium and glucose in the intestine
(Facilitated transport of SODIUM by absorption of GLUCOSE )
ORT is less expensive than IV therapy and has a lower complication rate.
IV therapy still may be required for patients with severe dehydration; patients with
uncontrollable vomiting; patients unable to drink because of extreme fatigue, stupor,
or coma, or patients with gastric or intestinal distention.
Treatment of minimal or no dehydration:
Rehydration therapy no need.
Replacement of losses:
o
Less than 10 Kg 60-120 ml ORS for each diarrheal tool or vomiting episode.
o
More than 10 Kg 120-140 ml ORS for each diarrheal tool or vomiting episode.
Nutrition continue breastfeeding or resume age-appropriate normal diet after
initial hydration (first 3-4 hours), including adequate caloric intake for maintenance.
Treatment of mild to moderate dehydration:
Rehydration therapy ORS, 50-100 ml/kg body weight over 3-4 hr.
Replacement of losses:
o
Less than 10 Kg 60-120 ml ORS for each diarrheal tool or vomiting episode.
o
More than 10 Kg 120-140 ml ORS for each diarrheal tool or vomiting episode.
Nutrition continue breastfeeding or resume age-appropriate normal diet after
initial hydration (first 3-4 hours), including adequate caloric intake for maintenance.
Treatment of severe dehydration:
Rehydration therapy:
o
By I.V fluid (normal saline or ringer lactate).
o
Phase 1:
Bolus in emergency.
Give 20 ml/kg I.V.
Give it in 20 min or 1 hour.
Can be repeated for 3 times.
Can use more than one line at the same time.
Assess the success of rehydration by examining heart rate, capillary refill, urine
output, mental state.
In cardiogenic shock give inotropic drug (dopamine).
In anaphylactic shock give anti-histamine.
In septic shock give antibiotics.

4
o
Phase 2:
Deficit:
10% X body weight.
% is the percentage of dehydration form the clinical manifestation.
If 5% give 50 ml.
If 10% give 100 ml.
If 15% give 150 ml.
Example: 10% loss 10/100 X 10 kg = 1 liter (1000 ml we substrate the bolus
from this 1000 ml and give the remaining as maintenance).
Maintenance:
First 10 Kg 100 cc/Kg/24 hr.
Second 10 Kg 50 cc /Kg/24 hr.
> than 20 Kg 20 cc /Kg/24 hr.
The maximum total fluid per day is normally 2,400 ml.
Ongoing losses:
Calculated CC for CC and mmol for mmol and added to the rehydrating
solution.
Replacement solutions should have approximately the same electrolyte
composition as the fluid that is lost.
Electrolyte content can be measured directly, or a solution can be selected
based on the typical electrolyte composition of diarrhea or gastric losses
Replacement of losses:
o
Less than 10 Kg 60-120 ml ORS for each diarrheal tool or vomiting episode.
o
More than 10 Kg 120-140 ml ORS for each diarrheal tool or vomiting episode.
o
If unable to drink, administer through nasogastric tube or administer 5% dextrose in
normal saline with 20 mEq/L potassium chloride IV.
Nutrition continue breastfeeding or resume age-appropriate normal diet after
initial hydration (first 3-4 hours), including adequate caloric intake for maintenance.
Notes:
In rehydration phase:
o
Blood is an appropriate fluid choice for a child with acute blood loss.
o
Potassium is not usually included in the intravenous fluids until the patient voids.
o
The resuscitation or rehydration phase (treatment of shock state) is same in iso,
hypo, & hypernatremic dehydration.
o
If improvement is not observed after 60 mL/kg of fluid administration, other
etiologies of shock (eg, cardiac, anaphylactic, septic) should be considered.
Hemodynamic monitoring and inotropic support may be indicated.
Solutions used in bolus:
o
Normal saline better to start with it (no K).

5
o
Ringer solution contain potassium, better than N.S. but need good urine output
and good renal function.
Maintenance fluid:
o
Maintenance requirements of electrolytes:
Sodium: 2 - 3 mEq/kg/day.
Potassium: 1 - 2 mEq/kg/day.
o
Composition of Maintenance fluids:
Child WT < 10Kg D5 + ¼ NS (38.5mEq/L) + 20 mEq/L of [K].
Child WT > 10Kg D5 + ½ NS (77mEq/L) + 20 mEq/L of [K].
o
It consist of water, glucose, K, Na to reduce starvation, ketoacidosis, protein
degeneration, in longstanding parenteral feeding.
o
N.S cause rapid rehydration (decease hospital admission and duration), so we can
use it in the whole deficit but we cannot use it in maintenance (use Ringer).
o
These guidelines assume that there is no disease process present that would
require an adjustment in either the volume or the electrolyte composition of
maintenance fluids.
o
The daily maintenance fluid is added to the fluid deficit, in general, the
recommended administration is one half of this volume administered over 8 hours
and administration of the remainder over the following 16 hours.
o
Continued losses (eg, emesis, diarrhea) must be promptly replaced.
o
If the child is isonatremic (130-150 mEq/L), the sodium deficit incurred can
generally be corrected by administering the fluid deficit plus maintenance as 5%
dextrose in 0.45-0.9% sodium chloride. Potassium (20 mEq/L potassium chloride)
may be added to maintenance fluid once urine output is established and serum
potassium levels are within a safe range.
Isonatraemic dehydration (Na 135-150 meq/l):
Most common type.
Patient with usual signs of dehydration.
Loss of Na is parallel to loss of water.
The losses of sodium and water are proportional and plasma sodium remains within
the normal range.
Hyponatraemic dehydration (Na <135 mEq/L):
When children with diarrhea drink large quantities of water or other hypotonic
solutions, there is a greater net loss of sodium than water, leading to a fall in plasma
sodium (hyponatraemic dehydration).
This leads to a shift of water from extra to intracellular compartments.

6
The increase in intracellular volume leads to an increase in brain volume, which may
result in convulsions, whereas the marked extracellular depletion leads to a greater
degree of shock per unit of water loss.
This form of dehydration is more common in poorly nourished infants in developing
countries.
Treatment:
o
Treatment of hypovolemic hyponatremia requires administration of IV fluids with
sodium to provide maintenance requirements and deficit correction and to replace
ongoing losses.
o
Most patients with hyponatremic dehydration do well with the same basic strategy
for correction of Isonatremic dehydration.
o
The initial goal in treating hyponatremia is correction of intravascular volume
depletion with isotonic fluid (NS or LR).
o
An overcorrection in the serum sodium concentration (>135mMol/L) is associated
with an increased risk of central pontine myelinolysis (CPM).
o
The risk of CPM also increases with overly rapid correction of the serum sodium
concentration, so it is best to avoid increasing the sodium by >12 mEq/L each 24 hr.
o
Emergency treatment of symptomatic hyponatremia, such as seizures, uses IV
hypertonic saline to increase the serum sodium concentration rapidly, which leads
to a decrease in brain edema.
o
Each 1 ml/Kg of 3% sodium chloride increases the serum sodium by approximately
1 mEq/L.
o
A child often improves after receiving 4 to 6 mL/kg of 3% sodium chloride.
o
The aim should be to increase the serum sodium concentration to not more than
130 mEq/L.
Hypernatraemic dehydration (Na >150 mEq/L):
Hypernatremic dehydration is the most dangerous form of dehydration due to
complications of hypernatremia and of therapy.
Hypernatremia can cause serious neurologic damage, including central nervous system
hemorrhages and thrombosis.
This appears to be secondary to the movement of water from the brain cells into the
hypertonic extracellular fluid, causing brain cell shrinkage and tearing blood vessels
within the brain.
Clinical manifestations:
o
Children with hypernatremic dehydration often appear less ill than children with a
similar degree of isotonic dehydration.
o
Urine output may be preserved longer, and there may be less tachycardia.

7
o
Children with hypernatremic dehydration are often lethargic and irritable when
touched.
o
The pinched abdominal skin has a "doughy" feel.
o
Hypernatremia may cause fever, hypertonicity, and hyperreflexia.
o
More severe neurologic symptoms may develop if cerebral bleeding or thrombosis
occurs.
Treatment:
o
Too rapid treatment of hypernatremic dehydration may cause significant morbidity
and mortality.
o
Idiogenic osmoles are generated within the brain during the development of
hypernatremia.
o
These idiogenic osmoles increase the osmolality within the cells of the brain,
providing protection against brain cell shrinkage secondary to movement of water
out of cells into the hypertonic ECF, they dissipate slowly during correction of
hypernatremia.
o
With rapid lowering of the extracellular osmolality during correction of
hypernatremia, there may be a new gradient created that causes water movement
from the extra-cellular space into the cells of the brain, producing cerebral edema.
o
Symptoms of the resultant cerebral edema can produce seizures, brain herniation,
and death.
o
To minimize the risk of cerebral edema during correction of hypernatremic
dehydration, the serum sodium concentration should not decrease more than 12
mEq/L every 24 hours.
o
The deficits in severe hypernatremic dehydration may need to be corrected over 2
to 4 days.
o
The initial resuscitation-rehydration phase of therapy remains the same as for other
types of dehydration.
Typical fluids:
o
D5 in ¼ NS ( ½ NS) + 20 mEq/L [K]
o
Seizures are the most common manifestation of cerebral edema from an overly
rapid decrease of the serum sodium concentration during correction of
hypernatremic dehydration
o
Acutely, increasing the serum concentration via an infusion of 3% sodium chloride
can reverse the cerebral edema.

8
Management of dehydration:
Fluid management of dehydration:
o
Restore intravascular volume.
o
Normal saline: 20 mL/kg over 20 min (repeat until intravascular volume restored)
(maximum = 1 L over 2 hr).
o
Calculate 24-hr water needs.
o
Calculate deficit water.
o
Calculate maintenance water.
o
Select an appropriate fluid (based on total water and electrolyte needs).
o
Administer half the calculated fluid during the first 8 hr, first subtracting any
boluses from this amount.
o
Administer the remainder over the next 16 hr.
o
Replace ongoing losses as they occur.
o
Note: most children do not require specific antiemetic therapy; careful oral
rehydration therapy is usually sufficient.
Monitoring therapy:
o
Vital signs Pulse, Blood pressure.
o
Intake and output Fluid balance, UOP, specific gravity.
o
Physical examination Weight, Clinical signs of depletion or overload.
o
Electrolytes.
Antimicrobial:
o
Campylobacter Erythromycin.
o
Clostredia difficle Vancomycin, Metronidazol.
o
Salmonella Amp, TMP-SMZ, Chloram, 3rd GCS.
o
Shigella Co-TMZ, Nalidixic acid, 3rd GCS.
o
V.cholerae Tetracycline, Co-TMZ.
o
G.lambilia Metronidazole.
o
E.histolytica Metronidazole.
o
Nitazoxanide G. lamblia, E. histolytica, C. difficile, and rotavirus.
Racecadotril:
o
An enkephalinse inhibitor, has inconsistently been shown to reduce stool output in
patients with diarrhea.
o
Experience with this drug in children is limited, and for the average child with acute
diarrhea it may be unnecessary.
Antiemetic agents:
o
Such as the phenothiazines are of little value and are associated with potentially
serious side effects (lethargy, dystonia, malignant hyperpyrexia).
o
Ondansetron is an effective and less-toxic antiemetic agent.
o
Because persistent vomiting can limit oral rehydration therapy, a single sublingual
dose of an oral dissolvable tablet of ondansetron (4 mg 4-11 yr and 8 mg for
children >11 yr [generally 0.2 mg/kg]) may be given.

9
Antimotility agents:
o
Such as loperamide are contraindicated in children with dysentery and probably
have no role in the management of acute watery diarrhea in otherwise healthy
children.
Probiotic:
o
The use of probiotic nonpathogenic bacteria for prevention and therapy of diarrhea
has been successful in developing countries.
o
In addition to restoring beneficial intestinal flora, probiotics can enhance host
protective immunity.
o
A variety of organisms (Lactobacillus, Bifidobacterium) have a good safety record.
Enteral feeding and diet selection:
o
Continued enteral feeding in diarrhea aids in recovery from the episode, and a
continued age-appropriate diet after rehydration is the norml.
o
Once rehydration is complete, food should be reintroduced while oral rehydration
is continued to replace ongoing losses from emesis or stools and for maintenance.
o
Breastfeeding or non-diluted regular formula should be resumed as soon as
possible.
o
Foods with complex carbohydrates (rice, wheat, potatoes, bread, and cereals), lean
meats, yogurt, fruits, and vegetables are also tolerated.
o
Fatty foods or foods high in simple sugars (juices, carbonated sodas) should be
avoided.
Zinc Supplementation:
o
Zinc administration for diarrhea management can significantly reduce all cause
mortality by 46% and hospital admission by 23%, also reduce duration and severity
of diarrhea.
o
All children older than 6 months of age with acute diarrhea in at-risk areas should
receive oral zinc (20 mg/day) in some form for 10-14 days during and continued
after diarrhea.
Prevention:
o
Promotion of exclusive breastfeeding.
o
Improved complementary feeding practices.
o
Rotavirus immunization.
o
Improved water and sanitary facilities and promotion of personal and domestic
hygiene.
o
Improved case management of diarrhea.

10
Acidotic breathing in child with dehydration (causes of acidosis in children):
Gastroenteritis with dehydration → low renal perfusion → ↓GFR → ↓ excretion of
acids by kidney (pre-renal failure).
Gastroenteritis with diarrhea → loss of inlet juice → losing bicarbonate (HCO3) → no
compensatory loss of acids by kidney due to ↓ GFR (which is the only organ can
excrete acids from the body) → acidosis.
Renal failure due to diseased kidney:
o
Congenital >> Horse shoe kidney, renal agenesis, duplication.
o
Acquired >> Chronic glomerulonephritis, nephritic syndrome, nephritis.
Ketoacidosis → DM.
RTA → (renal tubular acidosis):
o
Proximal RTA → problem in reuptake of HCO3. inefficient proximal tubules no
recollection of CHO acidosis.
o
Distal RTA → problem in excretion of H ion & retaining Na ions.
----------------------------------------------------------------------------------------------
www.facebook.com/ibnlatef
https://goo.gl/RpvNsl