
1
Babylon University
College of Medicine
Department of physiology
Dr. Ghafil Saihood Hassan 2016 -2017.
4- Cardiac output, exercise and cardiac hypertrophy.
Objectives:
1. Define cardiac output and stroke volume.
2. Describe how heart rate and stroke volume interact to control cardiac output.
3. State the influence of venous return on cardiac output.
4. Define the terms preload, and after load.
5. Measurement of COP.
6. Conditions that cause increase myocardial contractility.
7. Conditions that cause decrease myocardial contractility
8. Physiology of exercise.
9. Cardiac hypertrophy.
Cardiac output
:
Cardiac output is amount of blood pumped out of the heart each minute.
Cardiac output = Stroke volume x heart rate.
Cardiac output (COP) is affected by body metabolism, exercise, age and size of
the body. In young, healthy men, resting COP average about 5.6 L/minute. For
women, this value is 10-20% less
Stroke volume: It is the volume of blood ejected from the ventricle on each beat,
is expressed by the following equation:
Stroke volume = End-diastolic volume - End-systolic volume.
Ejection fraction: It is the fraction of end-diastolic volume ejected in one beat. It
is normally 55%. It is expressed by the following equation.
Ejection fraction = Stroke volume / End-diastolic volume.
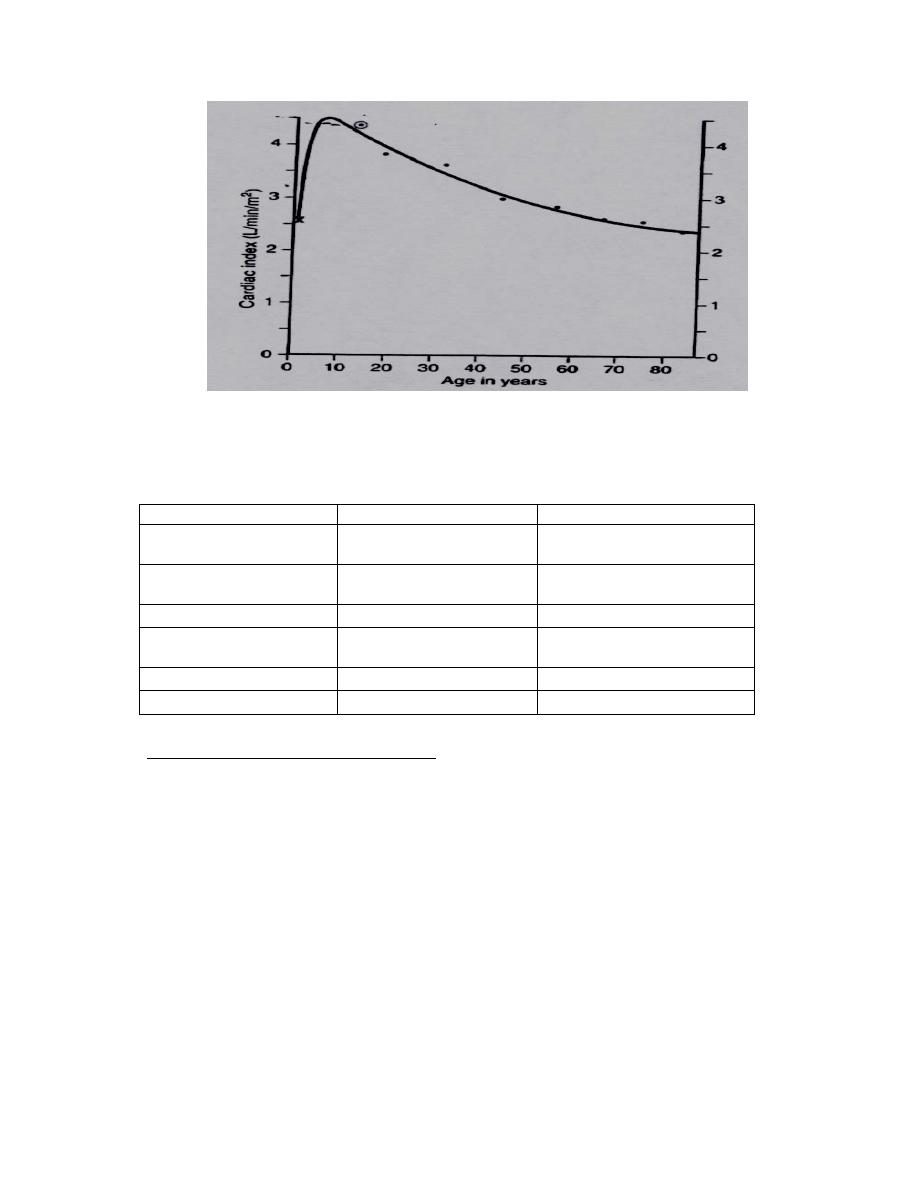
Cardiac index (CI):
Because there is a correlation between resting cardiac output (COP) and surface
area of the body, it is important to find some mean by which COP of different
sized people can be compared with one another. The COP is frequently stated in
term of the cardiac index, which is the cardiac output /minute / m² of body
surface. The normal average of cardiac index for adult is about 3.2 L.
The Cardiac index is rapidly rising from 2.5 L/minute/
m
2
at infant to a level
greater than 4 L/minute/m² at age 10 years, and then declines to about 2.4 L /
minute / m² at age 80 years. See figure 15.
2
Figure (15): Correlation between CI and age (Guyton & Hall 2006).
The effect of various conditions on COP is summarized in table (2).
Table (2): The effect of various conditions on COP.
Causes that increase COP Causes that decrease COP Causes that no effect on COP
1-Anxiety and excitement Sitting or standing from
lying position
Sleep.
2- Eating
Rapid arrhythmia
Moderate change in
environmental temperature
3-Exercise
Heart disease
4- High environmental
temperature.
5- Pregnancy.
6- Epinephrine
Methods of measurement of COP:
In the human, COP is measured by indirect methods that do not require surgery.
1-Direct Fick method:
Output of ventricle = O2 consumption (ml/minute) / A O2 – V O2.
= 250 ml /minute. / 190 ml/ L arterial blood – 140 ml/ L
venous blood in pulmonary artery.
= 250 ml/ minute / 50 ml/ L.
= 5L/minute.
Arterial O2 can be measured from sample taken from any artery in the systemic
circulation as it has same O2 concentration, while venous O2 concentration is
measured from pulmonary artery (by catheterization) because venous O2
concentration differ at different vein of systemic circulation.
2- Indicator dilution method: Dye or a radioactive isotope of known volume and
concentration is injected into an arm vein. The output of heart is equal to the
3
indicator injected divided by its average concentration in arterial blood after a
single circulation through heart.
3-Thermodilution method: The indicator used is cold saline. The saline is
injected into the right atrium through catheter and temperature change in the blood
is recorded in the pulmonary artery as right ventricular output is the same as left
ventricular output. The temperature change is inversely proportionate to amount of
blood flowing through the pulmonary artery. Cold saline is diluted by blood. This
technique has two important advantages: 1- The saline is completely innocuous. 2-
The cold is dissipated in tissue.
The stroke volume is controlled by:
Venous return (preload).
After load.
Myocardial contractility.
Cardiac compliance
A- Preload: It is the degree of myocardium to stretch before it contract according
to Frank-Starling law. Preload depend on the end diastolic volume (EDV). End
diastolic volume depends on the amount of blood return to the heart (venous
return). As end diastolic volume increase stroke volume increase.
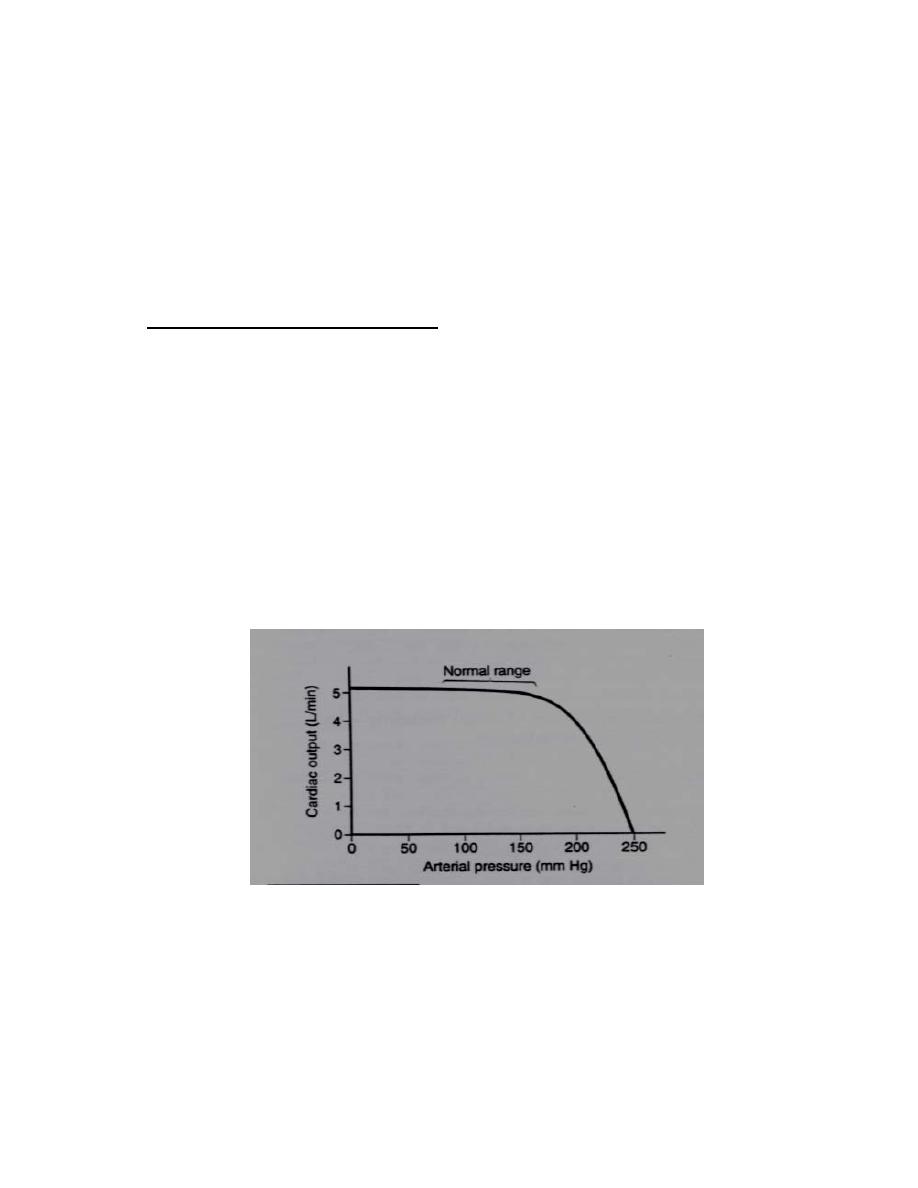
B- After load: Normally the resistance in pulmonary circulation is low, while the
resistance in systemic circulation is much higher. So the pressure in systemic
circulation is much higher than that of the pulmonary circulation. As the resistance
increase as in hypertension and in case of aortic stenosis disease, stroke volume
and COP drop. See figure 16.
Figure (16): Correlation between COP and pressure (Guyton & Hall 2006).
C-
Cardiac compliance:
It is the stretch ability. Decreased compliance in disease condition such as in case
of pericardial effusion affect stroke volume.
D--Myocardial contractility: It is the intrinsic ability of the cardiac muscle fibers
to develop force at a given muscle length. It can be estimated by the ejection
fraction, which is normally 55%. When contractility increases, the ventricle can
4
develop greater tension, pressure during systole and eject a large volume of blood
than normal.
Factors that cause increase myocardial contractility are:
1- Sympathetic stimulation: Sympathetic stimulation and noradrenaline exert a
+ve inotropic effect by increasing cyclic-AMP in the cardiac muscle fibers which
leads to activation of the Ca
+2
channels and more Ca
+2
influx from the ECF.
2- Circulating catecholamine: Catecholamines (epinephrine, norepinephrine and
dopamine) exert positive inotropic effect.
3- Change in ionic concentration:
Hyperkalemia decrease contractility, while hypercalcemia and hypernatremia
increase contractility. Hypernatraemia favors Na
+
influx and Na
+
-Ca
+2
exchanger
carrier, thus it has a +ve inotropic effect. On the other hand, hyponatraemia exerts
a -ve inotropic effect by an opposite mechanism. Hypercalcaemia exerts a +ve
inotropic effect as a result of more cytosolic Ca
+2
. Whereas hypocalcaemia has a
little (or no) -ve inotropic effect, since lowering of the serum Ca
+2
level causes
fatal tetany before affecting the heart. However, hypocalcaemia causes cardiac
flaccidity.
4- Cardiac rate: myocardial contractility increases as heart rate increases because
increase heart rate increase intracellular Ca concentration.
5- Hormones: Thyroid hormone and glucagons which increase the formation of
cAMP.
6- Cardiac rhythm: In ventricle extrasystole, the contraction is stronger than the
preceding normal contraction. Tachycardia causes a +ve inotropic effect while
bradycardia exerts a -ve inotropic action. The +ve inotropic effect in tachycardia is
due to increase intracellular Ca
+2
content.
7- Myethylxanthine: Such as caffeine and theophylline that inhibit the breakdown
of cAMP by phosphodiesterase. So they exert a +ve inotropic effect.
8-Digoxin; This drug inhibit the Na
+
-K
+
ATPase and Na
+
-Ca
+2
exchanger in the
sarcolemma of the cardiac muscle fibers, so the intracellular Na
+
concentration and
the intracellular Ca
+2
concentration increase. Digoxin is the drug used in treatment
of the heart failure.
9-Temperature: A moderate rise of the body temperature strengthens cardiac
contractility (by increasing the Ca
+2
influx and ATP formation in the muscle) while
an excessive rise of the body temperature (e.g. in fever) exhausts the metabolic
substrates in the cardiac muscle and decreases its contractility. Hypothermia also
decreases cardiac contractility.
Factors causes decrease contractility:
1-Myocardial infarction.
2- Myocarditis.
3- Hypercapnia, hypoxia and acidosis. An increase of the blood [H
+
] i.e. drop of
the blood pH (acidosis) produces a –ve inotropic effect, whereas a decrease of the
blood [H
+
] i.e. rise of the blood pH (alkalosis) produces a + ve inotropic effect.
4-Parasympathetic stimulation.
5
5-Drugs: Barbiturates, procainamide (and other anesthetic drugs) as well as Ca
+2
blocker drugs all have a –ve inotropic effect by decreasing Ca
+2
influx into the
cardiac muscle fibers.
6-Toxins: Several toxins (e.g. certain snake venoms and the toxin released by the
diphtheria microorganisms) produce a-ve inotropic effect (mostly by a direct action
on the contractile mechanism of the cardiac muscle).
:
Effect of exercise
1-Blood flow is increase from 5.5 L/min to 20 – 35L/min. The total amount of
oxygen entering blood increase from 250 ml/min at rest to 4000 ml/min
2-Ventilation increases with onset of exercise.
3- When exercise becomes more vigorous, buffering of increased amount of lactic
acid that are produced liberates more CO2, and the further increase ventilation.
4- As result of the accumulation of CO2 and rise in temperature, the capillary
bed of contracting muscle is dilated. Increase metabolic rate of muscle to rise as
much as 100 fold during exercise.
Fatigue is produced by decline in blood pH produced by lactic acidosis.
COP increase during exercise by:
1-Sympathetic stimulation.
2- Increase catecholamine release.
3-Increase venous return.
4 - Decrease after-load
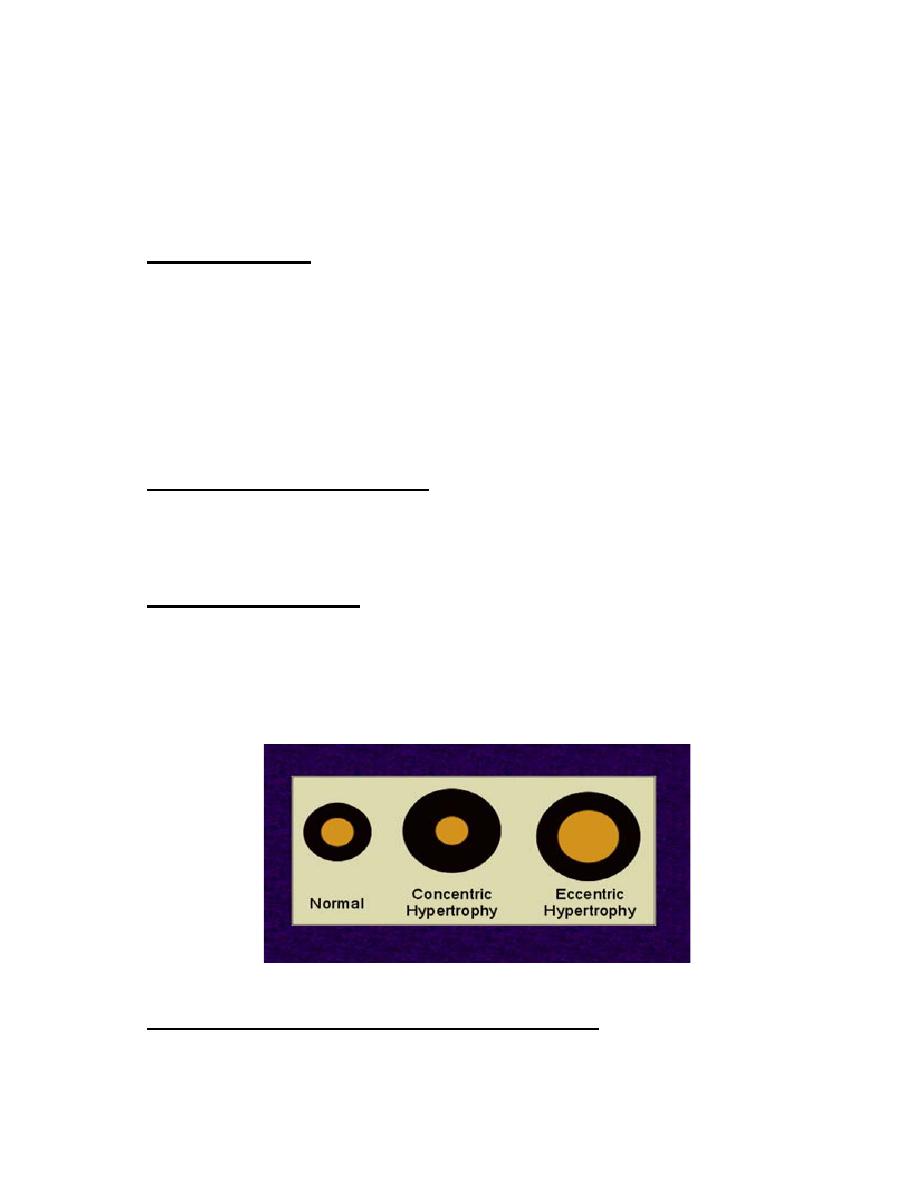
Cardiac hypertrophy:
1-Prolonged volume over load: It leads to eccentric hypertrophy. Increase in left
ventricle volume, with little increase in wall thickness. The stroke volume is triple.
2-Prolonged pressure over load: It will cause concentric hypertrophy of
ventricular wall, an increase in thickness of ventricular wall, but ventricular end-
diastolic volume remains unchanged. Figure (17).
Figure (17): Effect of volume and pressure overload.
Conditions associated with prolong volume over load:
1-Chronic exercise in the athlete.
6
2- Anaemia, due to lower viscosity of blood, lower resistance of venous
return by decrease TPR because lack of O2 delivery to tissue due to low
RBC and Hb.
3- Mitral regurgitation.
4- Aortic regurgitation
.
5- Systemic arteriovenous fistula.
6- Left to right shunt due to ventricular-septal defect.
7- Hyperthyroidism
.
Conditions associated with increased pressure over load:
Increase in the left ventricular pressure by:
1- Hypertension and aortic stenosis.
2- Increase in the right ventricular pressure by pulmonary artery hypertension and
pulmonary valve stenosis.