1
Babylon University
College of Medicine
Department of physiology
Dr. Ghafil Saihood Hassan 2016 - 2017
3- Electrical and mechanical events of the heart.
Objectives:
1- Define resting membrane potentials of cardiac cells.
2- Define action potential of cardiac cells.
3- Describe action potential of ventricle, atria, and the purkinje system (Fast
response).
4- State the benefit of plateau to cardiac cells.
5- Action potential in SA node (Slow response).
6- Latent pacemaker.
7- Refractory period.
8- Mechanical events of left ventricle.
Resting membrane potentials of cardiac cells:
The resting membrane potential is expressed in milli volts (mV). Intracellular
potential is expressed relative to extracellular potential. The resting membrane
potential of cardiac cells is determined primarily by potassium ions. The
conductance (permeability) to K ion at rest is high, while the conductance to
sodium is low. The normal concentration of K in the cell is about 150 mM, and
about 4 mM out the cell. While the normal concentration of Na is about 20 mM
inside the cell and 145 mM outside the cell. Myocardial cells have a resting
membrane potential of approximately – 85, instead – 90 mV. Changes in
membrane potential are caused by flow of ions into or out of the cell.
Action potential of cardiac muscles:
The action potential of cardiac muscle differs from skeletal muscles in
prolonged action potential (Plateau) and in strength of contraction (more calcium
ions enter cardiac muscle cells from ECF and sarcoplasmic reticulum).
Depolarization causes the membrane potential to become less negative. It occurs
when there is movement of positive charge (sodium or calcium ions) into the cell.
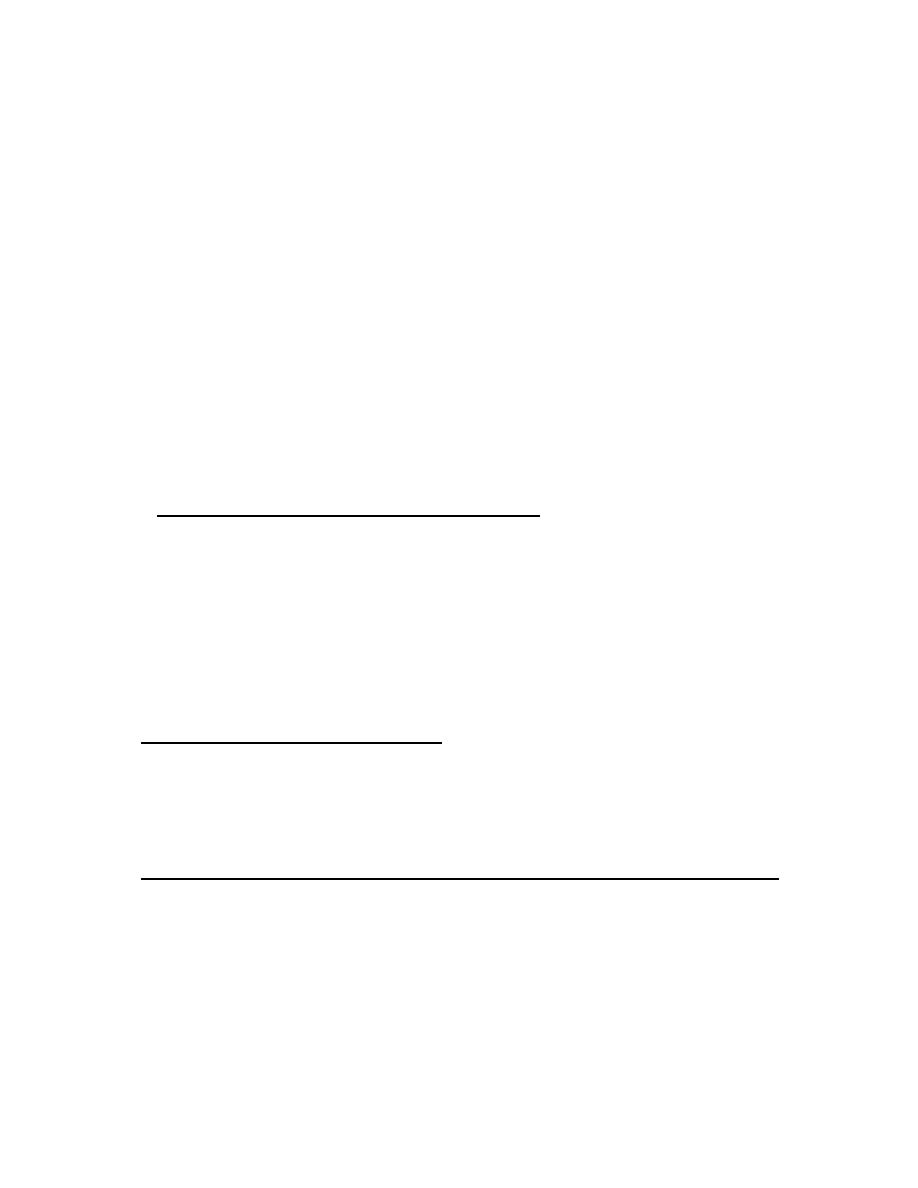
Action potential of ventricle, atria, and the purkinje system (Fast response):
Action potential of single cardiac muscle cell in these tissues is characterized by
rapid depolarization due to opening fasting sodium channels and a slow
depolarization during a plateau. The action potential duration is long, varies from
150 ms in the atria to 250 ms in the ventricle to 300 ms in purkinje system and
consequently the long refractory period. The resting membrane potential in these
tissues is stable. The initial depolarization is due to Na ion influx through rapidly
opening Na ion channels. The Ca ions influx through more slowly opening Ca ion
channels produces the plateau phase, and repolarization is due to K ion efflux
through three types of K ion channels.
2
The action potential has five phases:
1- Stage 4 (Resting membrane potential); the membrane potential is stable, inward
and outward currents are equal. The resting membrane potential about (- 90 mV).
Resting membrane potential of cardiac cells is determined primarily by potassium
ions.
2- Stage 0 (Rapid depolarization); this is caused by opening of voltage-gated fast
Na channels (it open for short time only). The opening of fast Na channels
change the action potential from –85 mV to + 20 mV. These channels are self
inactivating. Their conductance is controlled by two different gates, active gate,
open quickly at threshold potential producing the sudden rise in Na permeability
inactive gate, begins to close at same time as active gate open but moves less
quickly. It inactivate channel automatically after a few milliseconds.
3- Stage 1 (Early repolarization or spike); It is caused by the closure of Na
channels, chloride ions influx, and outward current of K ion (transient outward K
ion current).
4-stage 2 (Plateau); Plateau will prevent myocyte from repolarization. It is
caused by the passage of Ca into cell through the slowly voltage gated Ca
channels. They open when the cell depolarized beyond –35 mV (during rapid
depolarization).
5-Stage 3 (Delay repolarization); at late of plateau most of the Ca and Na ions
channels are inactivated. The repolarization is due to net K
+
efflux through
multiple types of potassium channels. See figure (11).
Figure (11): Action potential of ventricular cardiac cell (Fox 2006).
The benefits of plateau to cardiac cell are:
A- It will prolong the duration of excitation (absolute refractory period).
B- Prolong the duration of high cytoplasm Ca concentration, so it increase the
force of cardiac muscle contraction.
3
c- It gives more time that all cardiac cells can be activated together and contract
as one unit in the atria and ventricles.
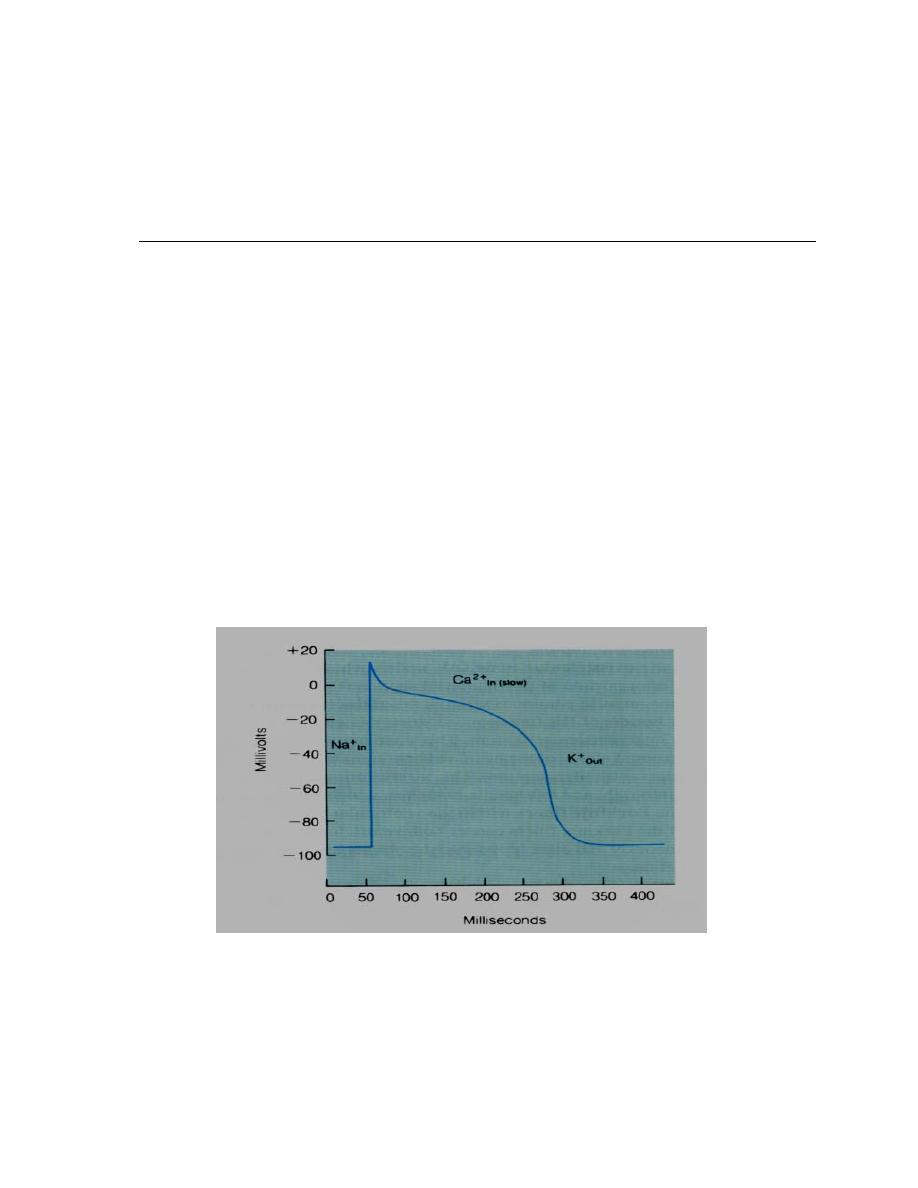
Action potential in SA node (Slow response):
The resting membrane potential of the sinus node is about -60 millivolts in
comparison with -85 millivolts for ventricular muscle fibers. The cause of this
lesser negativity is that the cell membrane of sinus fibers is leaky to sodium ions.
It has four phases:
Stage 4 (Pre-potential or pacemaker potential): SA node called pacemaker
because it can generate an action potential spontaneously.
Action potential in pacemaker tissue decline from – 60 mV to – 40 mV (called
prepotencies). The 1
st
. 2/3 of pacemaker potential is caused by Na ion influx
through the activated Na channels, the last 1/3 is due to Ca ion influx through
transient type Ca channel.
Stage 0: It is due to opening of long lasting type Ca cannel, that causes Ca ion
influx, and open at action potential –40 mV. The fast Na channels are not opened
because at –40 mV, they are not active. This is why stage 0 takes longer time
than that of atria and ventricle.
Stage 1 and 2: Stage 1 (spike) is not seen in pacemaker potential while stage 2
(plateau) is much shorter.
Stage 3 (Repolarization): It is caused by K efflux through outward K current
channels. See figure 12.
Figure (12): Action potential of SA node.
Latent pacemaker:
The cells in the SA node are not the only myocardial cells generate action
potential automaticity; other cells called latent pacemakers which include the
cells of the AV node, bundle of His and Purkinje fibers. They have driving the
heart rate only if the SA node is suppressed.
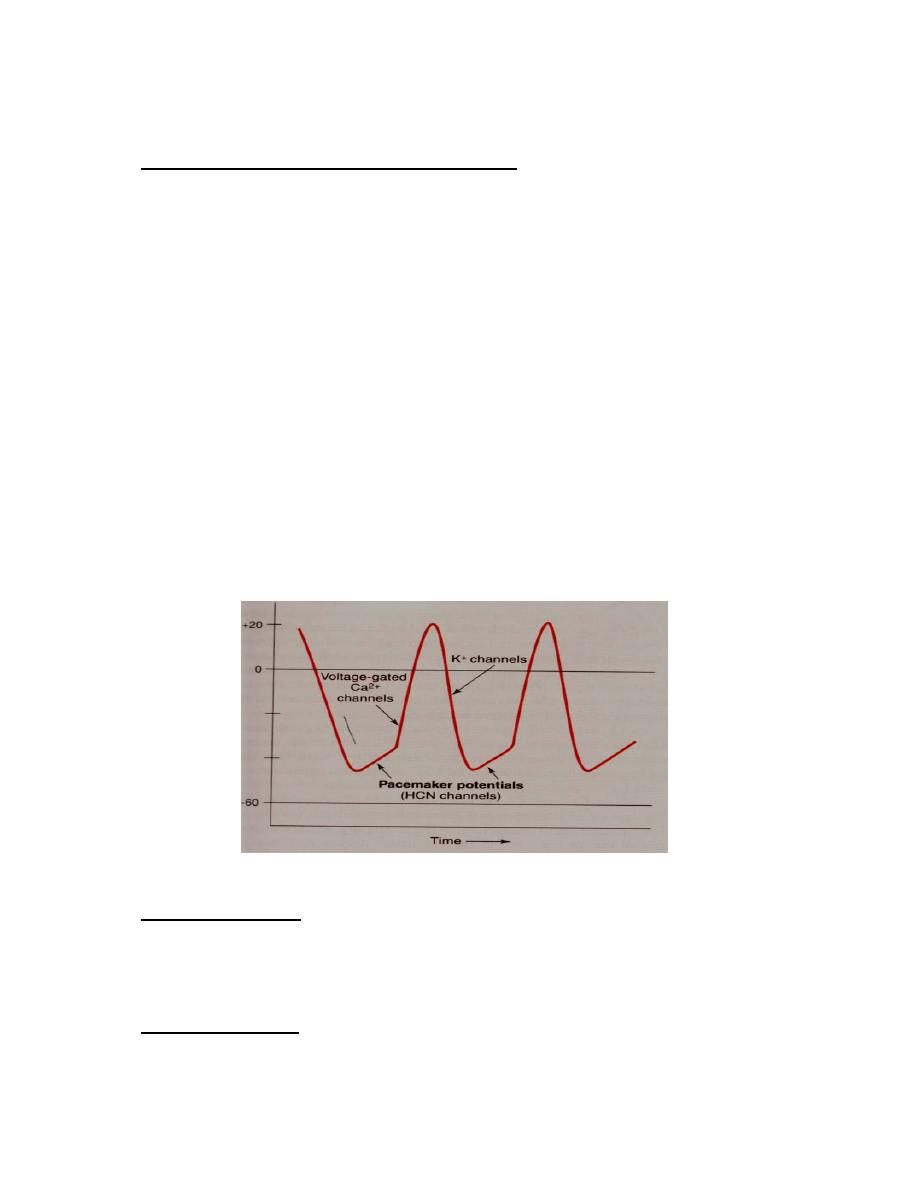
Refractory period:
1- Absolute refractory period (ARP): It is the period during which the
membrane can not be re-excited by an outside stimulation whatever the level of
4
external voltage applied. It is prolong in cardiac cell due to presence of plateau. It
occurs in phase 0, 1, 2 and half phase 3 until membrane reaches approximately –
50 mV during repolarization.
2- Relative refractory period (RRP): It is the time during which action potential
can be generated with stimulus larger than normal. See figure 13.
Figure (13): Refractory periods. ERP: the effective refractory period. ARP:
The absolute refractory period. RRP: The relative refractory period
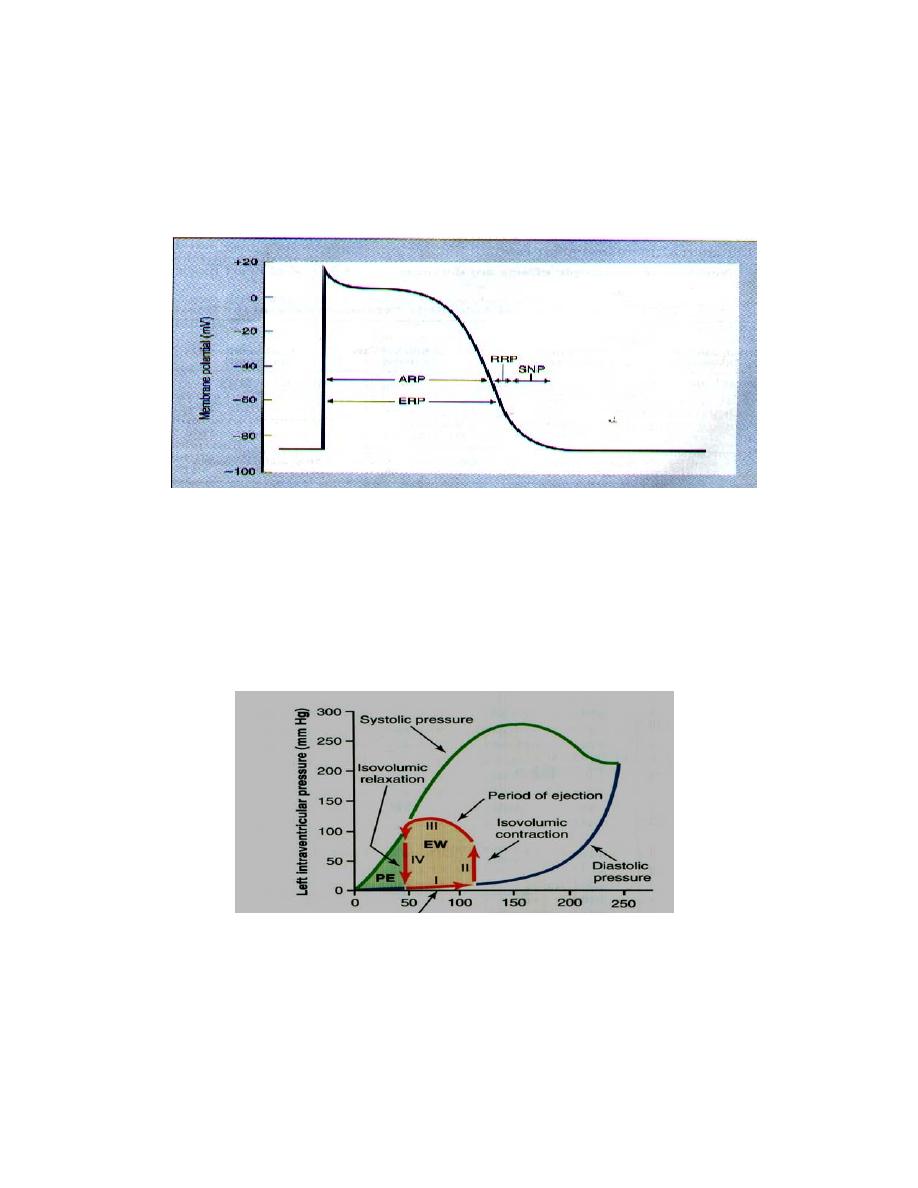
Mechanical events of left ventricle:
Figure 14 shows the different mechanical events (normal function) of left
ventricle during cardiac cycle: It is divided into four phases:
1- phase I: Period of filling.
2- Phase II: period of isovolumic Contraction.
3- Phase III: period of ejection.
4- Phase IV: Period of isovolumic relaxation.
Figure (14): Left ventricular function loop (Hall, 2016)
The filling of the ventricle which is about (120-130 ml) is called end diastolic
volume. The ventricle empties about 70 ml only stroke volume. The remaining
volume (50-60 ml) is called end systolic volume. Stroke volume differs
depending on age and size of body.

5
Ejection fraction = Stroke volume/ end diastolic volume, which is the fraction
of the end-diastolic volume that is ejected.
Normal ejection fraction of left ventricle (55-80%), right ventricle is (45%).