pg.
1
Fifth stage
Psychiatry
Lec-6
.د
الهام
6/11/2016
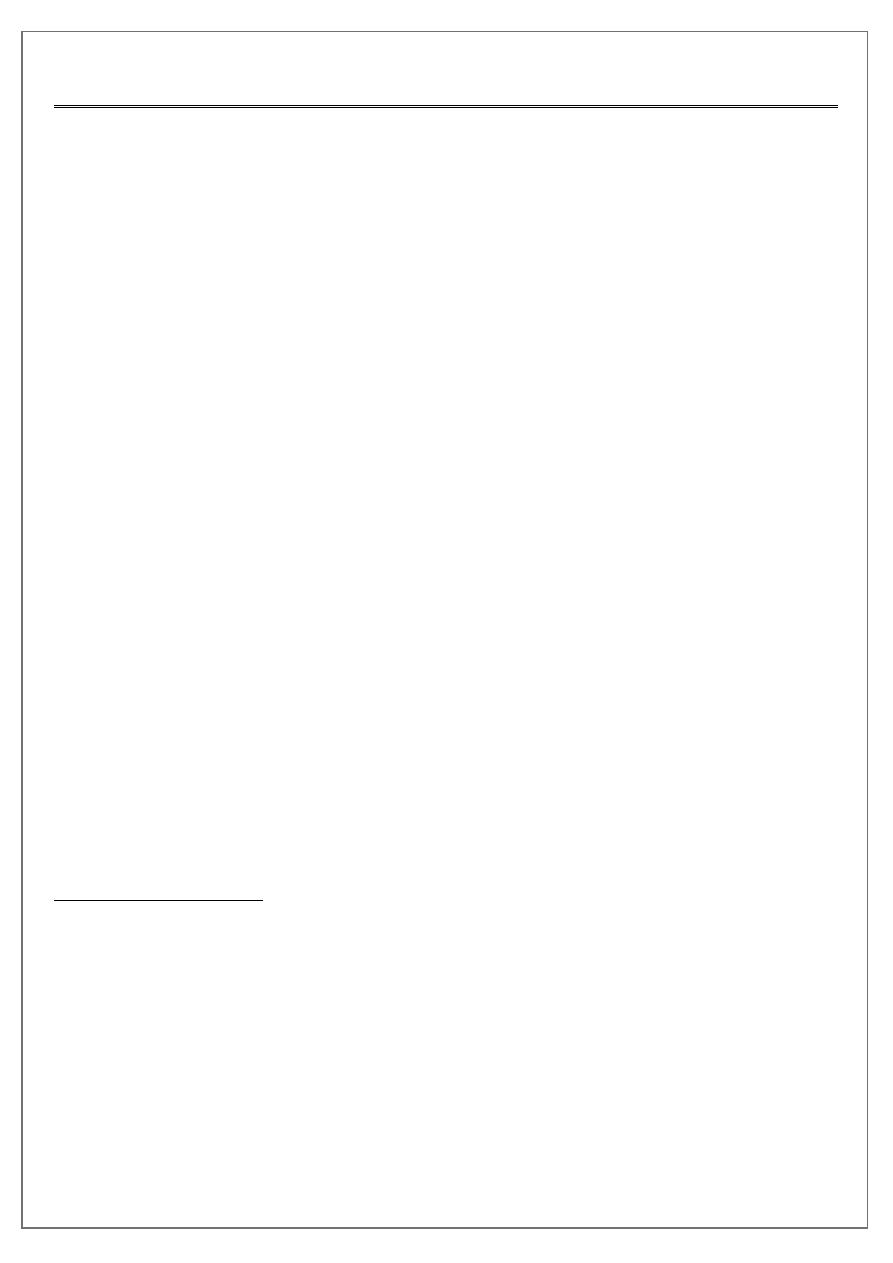
Obsessive compulsive disorder (OCD)
A common, chronic condition, often associated with marked anxiety and depression,
characterised by obsessions and compulsions .
Obsessions/compulsions must cause distress or
interfere with the person's social or individual functioning (usually by wasting time), and
should not be the result of another psychiatric disorder.
At some point in the disorder, the person recognizes the symptoms to be excessive or
unreasonable.
Clinical features:
Obsessional symptom
Thoughts
Ruminations
Impulses
'Phobias'
Compulsive rituals
Abnormal slowness
Anxiety
Depression
Depersonalization
Obsessional thoughts
words, ideas, and beliefs
recognized by patients as their own,
intrude forcibly into the mind.
unpleasant, or shocking to the person, (may be obscene or blasphemous).
atempts are made to exclude them.
It is the combination of an inner sense of compulsion and of efforts at resistance that
characterizes obsessional symptoms,
Obsessional thoughts may take the form of single words, phrases, or rhymes,
Obsessional images are vividly imagined scenes, often of a violent or disgusting kind (e.g.
involving sexual practices that the person finds abhorrent.
pg.
2
Obsessional rumnations
are internal debates in which arguments for and against even the simplest everyday
actions are reviewed endlessly.
Obsessional impulses
are urges to perform acts, usually of a violent or embarrassing kind (e.g. leaping in front
of a car, injuring a child, or shouting blasphemies at a religious ceremony).
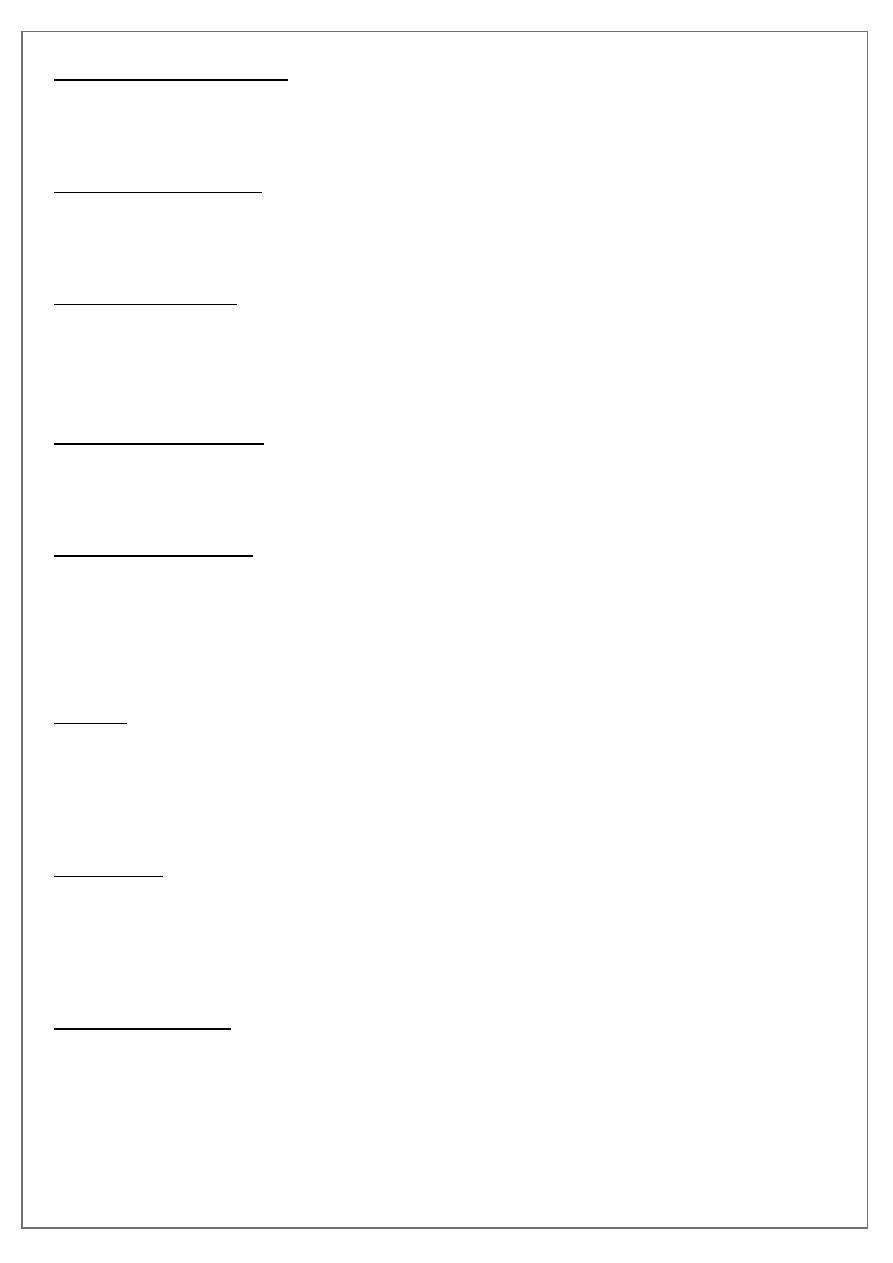
Obsessional rituals
include both mental activities (e.g. counting repeatedly in a special way, or repeating a
certain form of words) and repeated but senseless behaviours (e.g.washing the hands 20
or more times a day).
Obsessional slowness
. Although obsessional thoughts and rituals lead to slow performance, a few obsessional
patients are afflicted by extreme slowness that is out of proportion to other symptoms.
Obsessional phobias
. Obsessional thoughts and compulsive rituals may worsen in certain situations-for
example, obsessional thoughts about harming other people may increase in a kitchen or
other place where knives are kept. The person may avoid such situations because they
cause distress.
Anxiety
This is a prominent component of obsessivecompulsive disorders.
Some rituals are followed by a lessening of anxiety, while others are followed by
increased anxiety.
Depression
Obsessional patients are often depressed.
In some patients, depression is an understandable reaction to the obsessional
symptoms; in others, depression appears to vary independently.
Depersonalization
. Some obsessional patients complain of depersonalization.
The relationship between this distressing symptom and the other features of the
disorder is unclear.
pg.
3
Differential diagnosis
Anxiety disorders
Depressive disorder
Schizophrenia
Organic disorders
Epidemiology
Mean age: 20 yrs,
70% onset before age 25 yrs,
15% after age 35 yrs.
Sex distribution equal.
Prevalence: 0.5-3% of general population.
pg.
4
Aetiology of OCD:
Neurochemical Dysregulation of the 5HT system, or 5HT/DA interaction.
Immunological Cell-mediated autoimmune factors may be associated (e.g. against basal
ganglia peptides_as in Sydenham’s chorea).
Imaging CT and MRI: bilateral reduction in caudate size. PET/SPECT: hypermetabolism in
orbitofrontal gyrus and basal ganglia (caudate nuclei) that normalizes following
successful treatment (either pharmacological or psychological).
Genetic Suggested by family and twin studies (3-7% of first-degree relatives affected,
MZ: 50-80% DZ: 25%.), no candidate genes as yet identified.
Psychological Defective arousal system and/or inability to control unpleasant internal
states. Obsessions are conditioned (neutral) stimuli, associated with an anxiety-
provoking event. Compulsions are learned (and reinforced) as they are a form of
anxiety-reducing avoidance.
Psychoanalytical Regression from Oedipal stage to pre-genital anal-erotic stage of
development as a defence against aggressive or sexual (unconscious) impulses.
Associated defences:isolation, undoing, and reaction formation.
Associations:
Avoidant, dependent, histrionic traits (-40% of cases),
anankastic/obsessive-compulsive traits (5-15%) prior to disorder.
In schizophrenia, 5-45% of patients may present with symptoms of OCD (schizo-
obsessive poorer prognosis).
Sydenham chorea (up to 70% of cases) and other basal ganglia disorders (e.g. Tourette’s
Syndrome, post-encephalitic parkinsonism).
Comorbidity:
Depressive disorder (50-70%),
alcohol- and drug-related disorders,
social phobia,
specific phobia,
panic disorder,
pg.
5
eating disorder,
PTSD,
tic disorder (up to 40% in juvenile OCD) or TS.
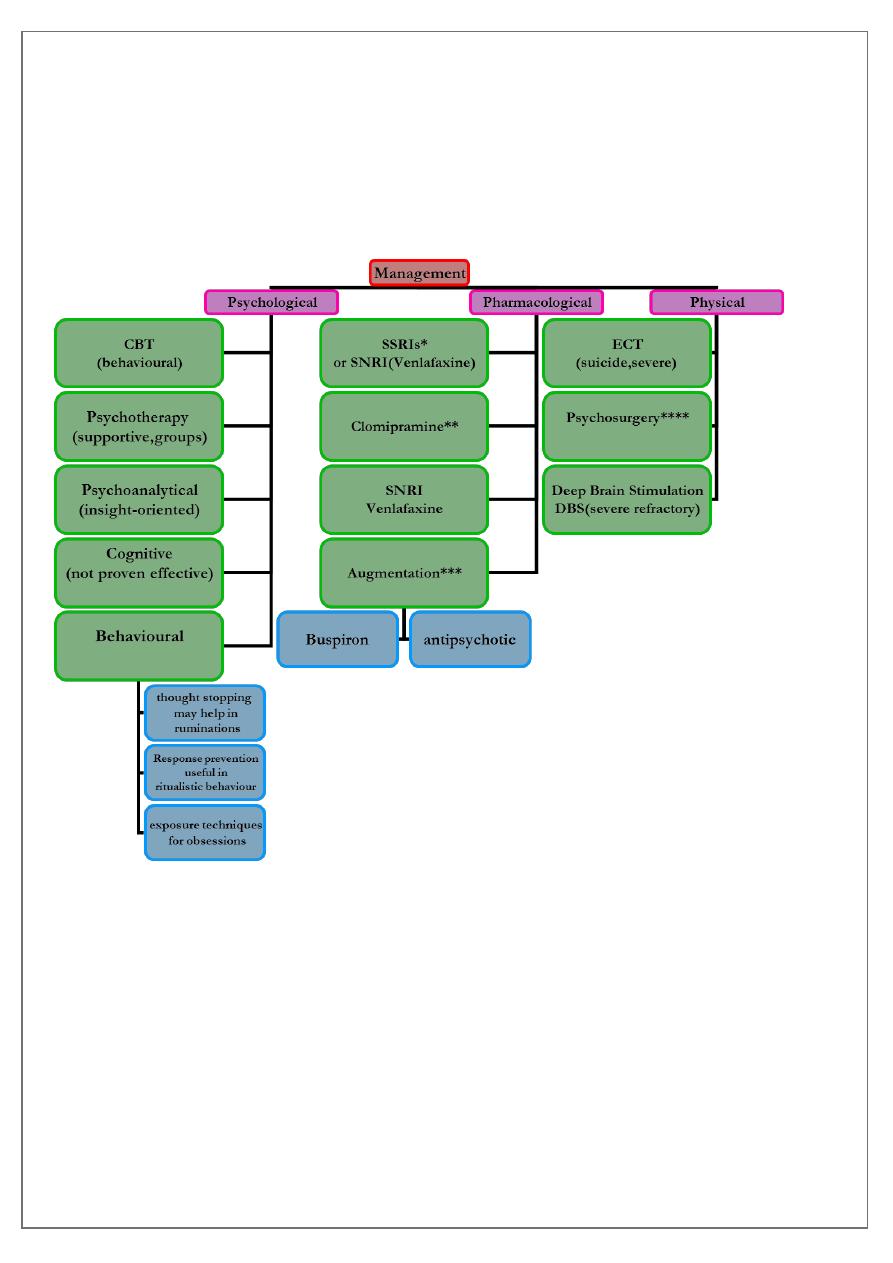
Management:
•
*
Antidepressants SSRIs: fluoxetine, fluvoxamine, sertraline, or paroxetine should be
considered first-line (no clear superiority of any one agent, high doses usually needed
(e.g. 40-60 mg fluoxetine, allow at least 12 wks for treatment response, regard as
long-term).
• **Clomipramine (e.g. 250-300 mg) has specific anti-obsessional action
( second-line choice).
• ***Augmentative strategies:
– antipsychotic (risperidone, haloperidol, pimozide)
pg.
6
• if psychotic features,
• tics, or
• schizotypal traits;
– buspirone/short term clonazepam if marked anxiety
• ****psychosurgery may be considered for severe, incapacitating intractable cases, i.e
treatment resistance:
– 2 antidepressants,
– 3 combination treatment,
– ECT, and
– behavioural therapy)
• where the patient can given informed consent e.g. stereotactic cingulotomy
(reported up to 65% success). In theory, disrupts the neuronal loop between the
orbitofrontal cortex and the basal ganglia.
Course:
Often sudden onset (e.g. after stressful loss event,e.g loss, pregnancy, sexual problem),
symptom intensity may fluctuate (contact-related/phasic) or be chronic.
Differential diagnosis:
Normal (but recurrent) thoughts, worries, or habits;
anankastic PD/OCD,
schizophrenia;
phobias;
depressive disorder;
hypochondriasis;
body dysmorphic disorder;
trichotillomania.

pg.
7
Outcome:
20-30% significantly improve,
40-50% show moderate improvement,
but 20-40% have chronic or worsening symptoms.
Relapse rates are high for stopping medication.
Suicide rate increased esp. if there is secondary depression.
Prognostic factors: