Lecture 01 Pathology D. Rasha
CARDIOVASCULAR SYSTEM
Blood Vessels:
Vascular disorders are responsible for more morbidity and mortality than any other
category of human diseases, arterial diseases are the most important. This importance
achieved from:
1- Narrowing vessels and this is producing ischemia of tissues perfused by such
vessels.
2- Damaging the endothelial lining and this is promoting intravascular thrombosis, a
process that contribute to critical ischemia of vital organs such as the heart and
brain.
3- Weakening the walls of vessels, predisposing to dilation or possibly rupture.
4- Contributing to the pathogenesis of some of the most common diseases in human
as atherosclerosis, hypertension and diabetes.
The blood vessels wall is consist of important cell types play a role in pathgenesis of severe
arterial disorders. These cell types are:-
(1) Endothelial cells:
Which are important multifunctional cells that's having many synthetic and metabolic
properties as:-
1- It regulates the activity of platelets and has an important role in modulating both
coagulation and fibrinolytic systems.
2- It regulates vascular tone and blood flow.
3- Elaboration of prothrombotic molecules.
4- Maintenance of permeability barrier.
(2) Vascular smooth muscles cells:-
Also have many functions;
1- Vasoconstriction and dilation in response to normal and pharmacological stimuli.
2- Extracellular matrix production as collagen, elastin and proteoglycans.
3- Migration and proliferation.

Arterial Disorders:-
Arteriosclerosis:-
Is the generic term for 3 pattern of vascular diseases, all of which cause thickening and
inelasticity of arteries:
(1) The dominant pattern is atherosclerosis which characterized by the formation of
intimal fibrofatty plaques that have a central core rich in lipid, this occur in large
arteries as
aorta
leading to ischemia of intestines and lower extremities and
abdominal aortic aneurysms which may rupture causing fatal hemorrhage, or
coronary arteries
resulting in ischemic heart diseases and myocardial infarction,
or
cerebral arteries
presented as cerebrovascular accident.
(2) Monkeberg's medial calcific sclerosis characterized by calcification in the media of
muscular arteries, it's usually occur in medium sized muscular arteries in person
older than 50 years. These medial lesions don't cause narrowing of vessel lumen.
(3) Arteriosclerosis which occurs in small vessels associated with hypertension and
diabetes mellitus, this type cause thickening of vessel walls and luminal narrowing
so it will cause ischemic injury of organs.
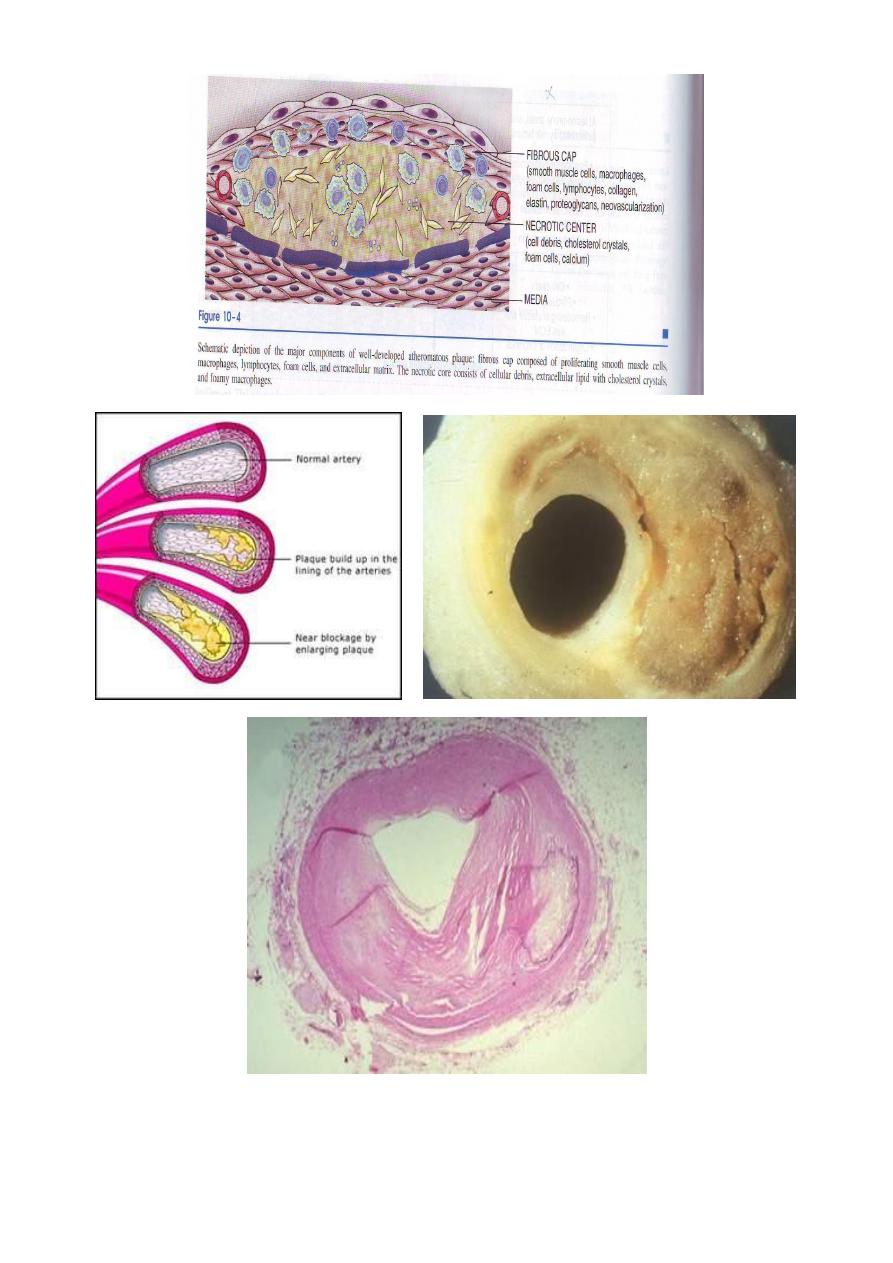
Atherosclerosis:-
Intimal plaques called (atheroma) that protrude into the lumen, weaken the underlying
media and undergo a series of complications as thrombosis so called atherothrombotic
disease characterize it.
Atherosclerosis alone accounts for more than half of all deaths in the western world ,the
disease begins in childhood and progress slowly over the decades.
Risk factors:-
Can be divided into constitutional factors and acquired factors which are controllable.
i.
Constitutional factors:-
1. Age: between 40-60 years increasing the risk to five folds.
2. Sex: men are much more prone to atheroma and its consequences than women
that's because females hormones may be protective while androgen may increase
the risk of atheroma.
So that after menopause the frequency of myocardial infarction becomes the same
in both sexes by the 70
th
and 80
th
decade of life.
3. Familial predisposition: it's most likely polygenic and it may relate to familial
clustering of other risk factors, such as HT, DM and familial hypercholesterolemia.

In other instances, it involves well defined hereditary genetic derangement in
lipoprotein deposition that result in high blood lipid vessels.
II.
Acquired factors:-
Can be divided into major risk factors which include:-
1- Hyperlipidemia.
2- Hypertension.
3- Cigarette smoking.
4- Diabetes mellitus.
Hyperlipidemia: specifically hypercholesterolemia. The major component of the total
serum cholesterol associated with increased risk is low density lipoproteins (LDL)
cholesterol. In contrast, the higher the level of high density lipoproteins (HDL), the
lower the risk. HDL is believed to mobilize cholesterol from developing an existing
atheroma and transport it to the liver for excretion in the bile, thereby called the
"good cholesterol".
The higher the level of HDL the lower is the risk of IHD.
Hypertension: major risk factor of atheroma at all ages. Both systolic and diastolic
levels are important in increasing the risk. Antihypertensive reduces the incidence of
ATH-related diseases, especially strokes and IHD.
Smoking: when one or more packs of cigarette are smoked per day for several years,
the death rate from IHD increased by up to 200%. Cessation of smoking reduced the
increased risk subtaintially.
Diabetes Mellitus: it induces hypercholesterolemia& a markedly increased
predisposition to atheroma. The incidence of MI is twice as high in diabetic as in non
diabetic. It also increases the risk of the stroke.
The less important risk factors are:-
1- Insufficient regular physical activity.
2- Obesity which regarded as independent risk factor.
3- Behavioral pattern & stress people who are aggressive and angry particularly at
risk
4- Diet high dietary intake of cholesterol & saturated fat such as those present in egg
yolk , animal fats & butter raises the plasma cholesterol level.
The multiple factors impose more than additive effect e.g. if 3 risk factors are present as
(hyperlipidemia, HT and smoking) the heart attack rate 7 times greater than when none
are present, but atherosclerosis may develop in absence of any apparent risk factors.

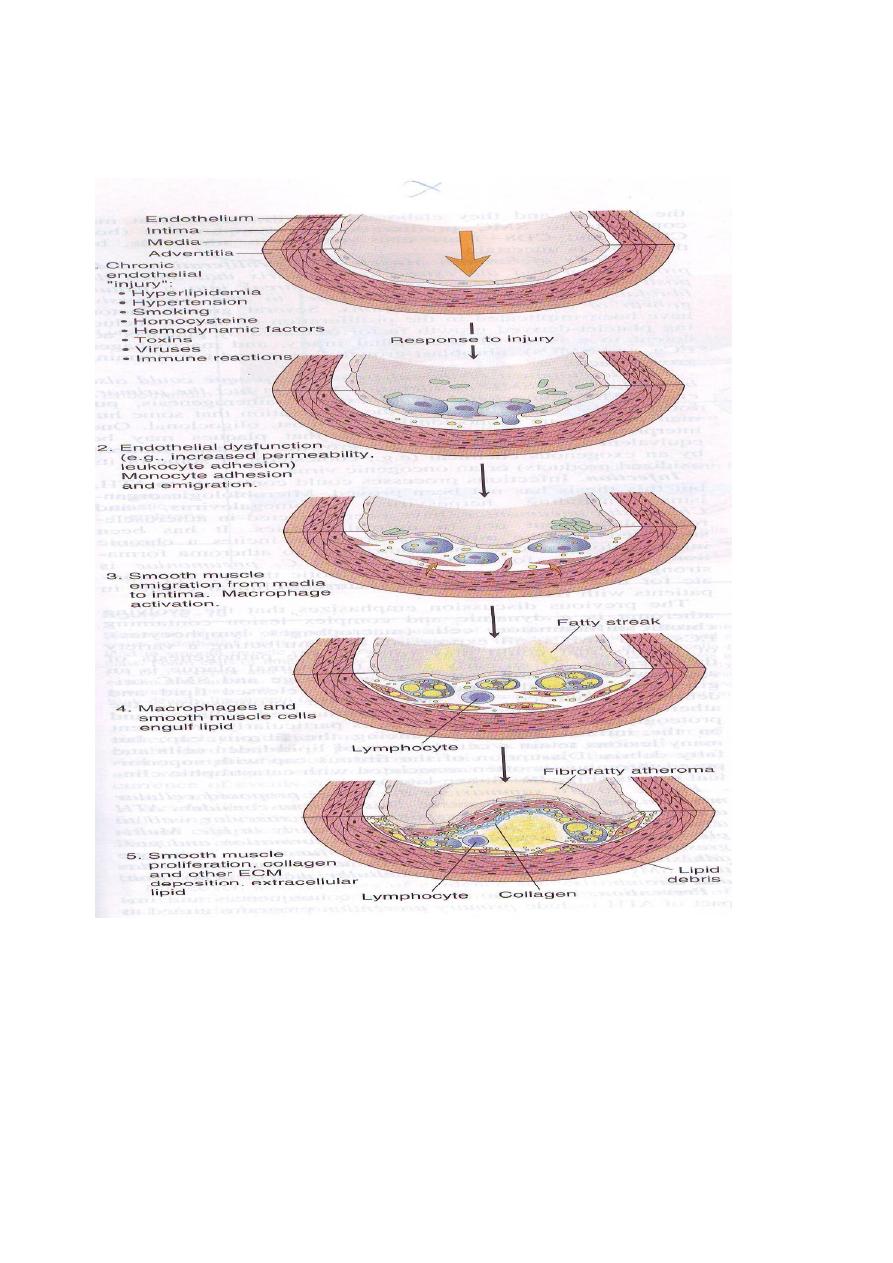
Pathogenesis:-
These are a number of hypotheses for pathogenesis of atherosclerosis, the most
important one is response- to- injury hypothesis which begins by chronic endothelial
injury from hyperlipidemia, HT, cigarette smoking, immune reaction, haemodynamic
factors, toxins and viruses, these factors cause increased endothelial permeability to:-
1- Lipoproteins especially LDL or modified LDL.
2- Circulating monocytes, leukocytes, T-lymphocytes and SMCs of intimal or
medial origin.
The monocytes after endothelial injury adhere and migrate between ECs to localized
subendothelially they transformed into macrophages and engulf the lipoproteins to
become foam cells, macrophages also proliferate in the intima. If injury continue,
platelets also adhere to the endothelium. SMCs some of medial origin also migrate in the
intima and take present lipids to transform into foam cells, the accumulation of these
foamy cells appear macroscopically as fatty streaks, the SMCs also synthesize collagen,
elastin and glycoproteins to form mature fibrofatty atheroma.
Thrombosis is a complication of late-stage atherosclerosis and organization of thrombi
may contribute to plaque formation, platelets generally do not adhere to the arterial wall
without severe injury of endothelial cells, Where the foam macrophages and SMCs died
the released extracellular lipid and cellular debris which surrounded by SMCs.
Morphology:-
Macroscopically:-
The atheroma of aorta and large arteries occur in childhood as fatty
streaks in the 1
st
years of life, these begin as 1 mm, soft yellow intimal discolorations (fatty
dots) that progressively enlarge by becoming thicker and slightly elevated while they
elongate with long axis to produce fatty streaks 1-3 mm wide and 1-5 cm length.
The atheroma plaque appearance depending on the content of lipid, so it may be bright
yellow if lipid content more, or grey if fibrous tissue more.
Microscopically:-
The plaques have essentially 3 components:-
1- Cells including vascular SMCs, blood derived monocytes/macrophages and
scattering of lymhpcytes.
2- Connective tissue fibers and matrix.
3- Lipids.
Some plaques contain relatively small amounts of lipids and are composing almost
entirely of connective tissue cells from fibrous plaque.
The extracellular lipid core composed of cholesterol (which forms needle-like crystals).
Plaques may develop 4 complications, these are:-
Ulceration
,
thrombosis
and
intraplaque hemorrhage
have serious consequences in
smaller vessels such as those of heart and brain and may cause
total occlusion
. In larger
vessels e.g. aorta, such complication have little effect on the luminal diameter by damage.
the underlying media may cause atherosclerotic aneurysm as in distal aorta below renal
arteries.