1
Fifth stage
Medicine
Lec-4
د
.فاخر
27/11/2016
GOUT
Gout once called the “Disease of Kings” is ,also seen in Women,Especially After
Menopause
GOUT
Gout is a true crystal deposition
disease. It can be defined as the pathological
reaction of the joint or periarticular tissues to the
presence of monosodium urate monohydrate
(MSUM) crystals.
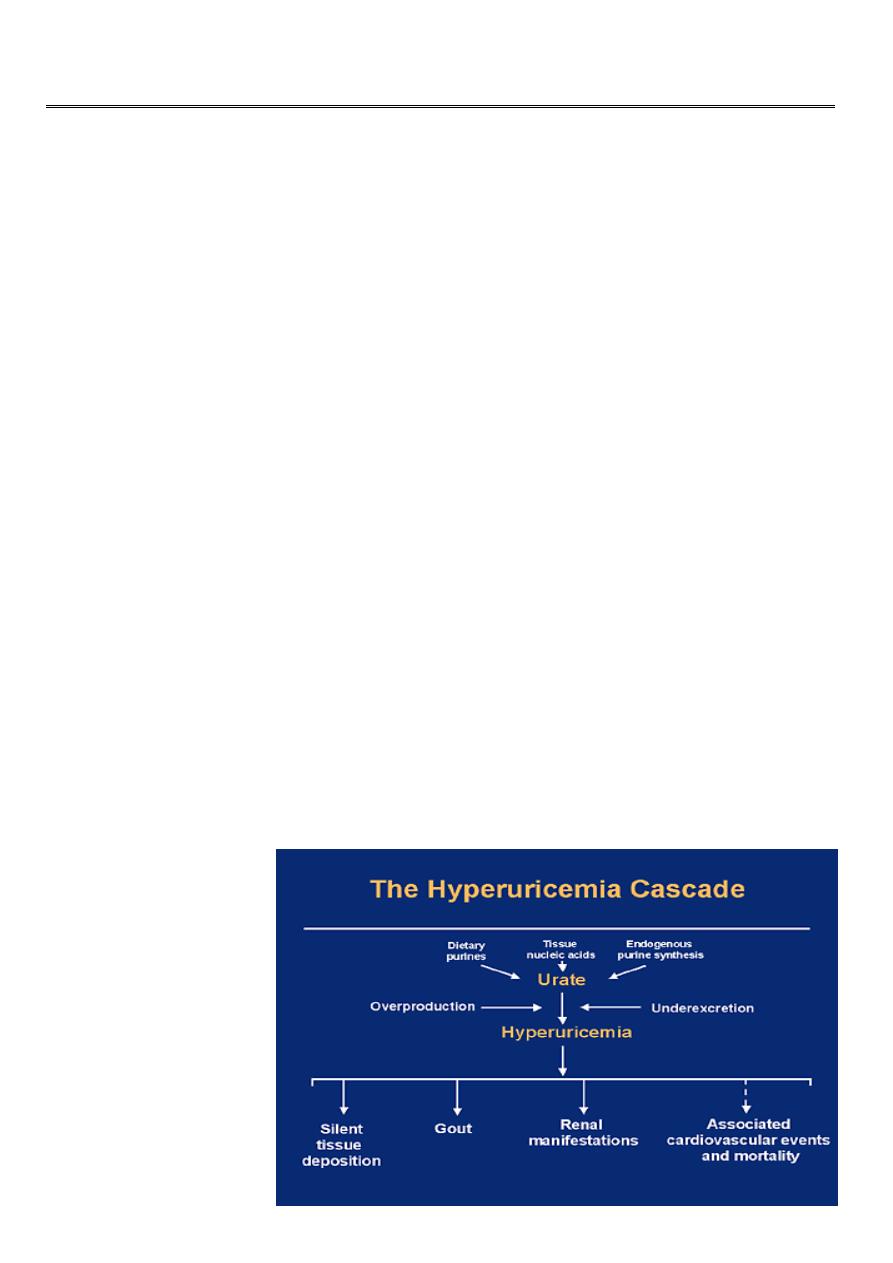
Urate : end product of purine metabolism
Hyperuricemia : serum urate > urate solubility)
6.8 mg/dl
The prevalence of gout varies between populations but is around 1% with a strong male predominance (> 10:1).
Prevalence increases with age and increasing serum uric acid concentration. 'Primary' gout is almost exclusively a
male disease and the most common cause of inflammatory arthritis in men over the age of 40..
HYPERURICEMIA & GOUT
Hyperuricemia caused by:(1)Overproduction 10%(2)Underexcretion 90%

2
Classification of Hyperuricemia
Overproduction (10%)
Ethanol
HGPRT deficiency
(hypoxanthine-guanine phosphoribosyl transferase)
PRPP synthetase overactivity
(phosphribosyl pyrophosphate synthetase)
Myeloproliferative disorders
Cytotoxic chemotherapy
Underexcretion (90%)
Renal insufficiency
Drugs and toxins
Diuretics
Ethanol
Cyclosporine A
Pyrazinamide
Lead nephropathy
Low-dose aspirin
Ketosis
Estrogen have a mild uricosuric effect; therefore, gout is unusual in premenopausal women
Higher renal clearance of urate in women possibly due to their higher plasma estrogen
levels
Pathogenesis of Gouty Inflammation
Urate crystals stimulate the release of numerous inflammatory mediators in synovial cells
and phagocytes
The influx of neutrophils is an important event for developing acute crystal induced
synovitis

3
GOUT RISK FACTORS
Male
Postmenopausal female
Hypertension
Pharmaceuticals:Diuretics, ASA, cyclosporine
Alcohol intake:Highest with beer
High BMI (obesity)
Diet high in meat & seafood
Clinical features
1- Acute gouty arthritis
extremely rapid onset, reaching maximum severity in just 2-6 hours, often waking the
patient in the early morning
severe pain, often described as the 'worst pain ever'
extreme tenderness-the patient is unable to wear a sock or to let bedding rest on the joint
marked swelling with overlying red, shiny skin
During the attack the joint shows signs of marked synovitis but also periarticular swelling
and erythema. There may be accompanying fever, malaise and even confusion, especially if
a large joint such as the knee is involved. As the attack subsides, pruritus and desquamation
of overlying skin are common. The main differential
diagnosis is septic arthritis, infective
cellulitis or
another crystal disease.
After an acute attack some people never have a second episode; in others the next episode
occurs after years. In most, however, a second attack occurs within 1 year and the
frequency of attacks gradually increases with time. Later attacks are more likely to involve
several joints and to be more severe
2-Chronic tophaceous gout
Large MSUM crystal deposits produce irregular firm nodules ('tophi') at the usual sites for
nodules around extensor surfaces of fingers, hands, forearm, elbows, Achilles tendons and
sometimes the helix of the ear. The white colour of MSUM crystals may be evident and
permits distinction from rheumatoid nodules.
4
TOPHI
—
Solid urate deposits in tissues
—
Irregular & destructive
3- Progressive renal disease
an important complication confined to untreated severe chronic tophaceous gout. This
results from MSUM crystal deposition in the interstitium of the medulla and pyramids with
consequent chronic inflammation, giant-cell reaction, fibrosis, glomerulosclerosis and
secondary pyelonephritis…Renal stone ..
Investigations
Definitive diagnosis requires identification of MSUM crystals in the aspirate from a joint,
bursa or tophus. In acute gout synovial fluid shows
increased turbidity due to the
greatly elevated cell count
(> 90% neutrophils..)
Assessment of renal function (serum creatinine, urine testing), hypertension, blood glucose
and serum lipid profile should be undertaken. An FBC and ESR should detect
myeloproliferative disorders during remission of acute gout. During an attack a marked
acute phase response (elevated CRP, neutrophilia) is usual; the ESR is often modestly raised
in tophaceous gout
X-rays can assess the degree of joint damage. In early disease they are usually normal, but
narrowing of joint space, sclerosis, cysts and osteophyte (changes of OA) may develop in
affected joints with time, or be
present as a predisposing factor in
secondary gout. Gouty 'erosions'
(bony tophi) are a less common but

5
more specific feature occurring as
para-articular 'punched-out' defects
with well-delineated borders and
retained bone density. Tophi may
also be visible as eccentric soft tissue swellings..
Management
The acute attack
A fast-acting oral NSAID (. Indomethacin 50 mg 4hourly. naproxen, diclofenac,) can give
effective pain relief and is the standard treatment. Patients can keep a supply of an NSAID
with which they are familiar and take it as soon as the first symptoms are noticed,
continuing for the duration of the attack.
. Oral colchicine (a potent inhibitor of neutrophil microtubular assembly)
can be very effective, but unfortunately often causes vomiting and severe
diarrhoea at the doses needed for rapid relief(1 mg loading dose, then 0.5 mg 6-hourly
until symptoms abate). The compromise is to try
lower doses (0.5 mg 8-12-hourly) for a slower onset of benefit.
Aspiration of the joint will give instant relief and, when combined with an intra-articular
corticosteroid injection to prevent fluid reaccumulation, often effectively aborts the attack
Correction of any predisposing factors
should always be attempted. Lifestyle alteration to correct obesity and reduce excess beer
consumption may significantly reduce hyperuricaemia. Diuretics should be stopped if
possible. Although a very high purine diet (large amounts of seafood, red meat and offal)
should be tempered, there is no need for a specific highly restrictive diet.
and trigger acute attacks..
HYPOURICAEMIC DRUGS
INDICATIONS FOR HYPOURICAEMIC DRUGS
1-Recurrent attacks of acute gout
Tophi
2-Evidence of bone or joint damage

6
3-Associated renal disease
4-Gout with greatly elevated serum uric acid
ALLOPURINOL
Allopurinol: blocks conversion
of xanthine to uric acid. Works
for underexcretors and overproducers
The aim of treatment is to bring the serum uric acid level into the lower half of the normal
range to ensure dissolution of crystals and to prevent new ones forming. The serum uric
acid should therefore be measured every 3-4 weeks and the dose of allopurinol increased in
100 mg increments until this is achieved (maximum 900 mg daily).
.