These are a heterogeneous group of diseases characterized
by inflammation and necrosis of blood-vessel walls, with
associated damage
to skin, kidney, lung, heart, brain and
gastrointestinal tract
. There is a wide spectrum of
involvement and disease severity, ranging from mild and
transient disease affecting
only the skin, to life-threatening
fulminant disease with
multiple organ failure
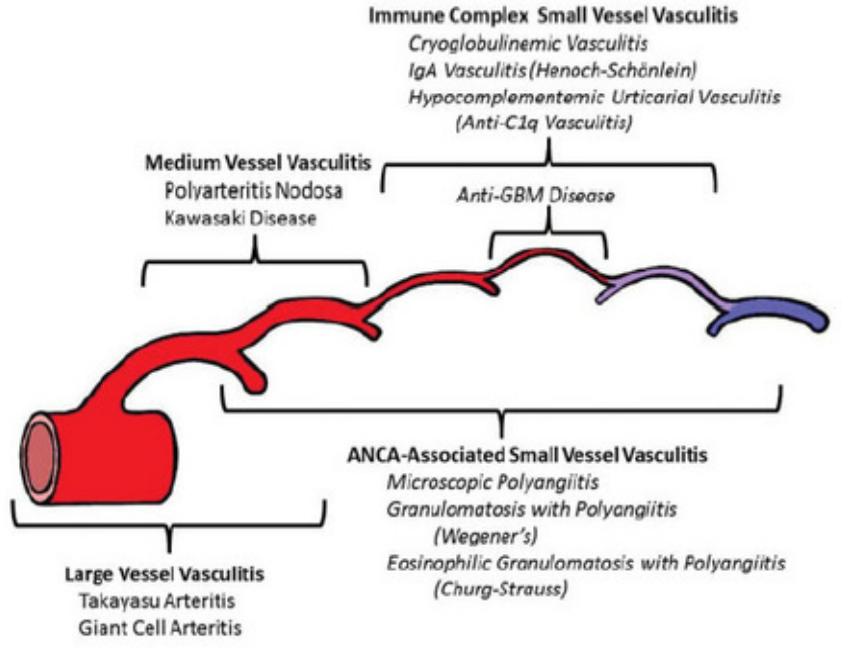
Classified according to the size of vessel involved into:
1-
Large vessel
–giant cell arteritis ,Takayasu’s arteritis
2-Medium vessel
–classical polyarteritis nodosa ,
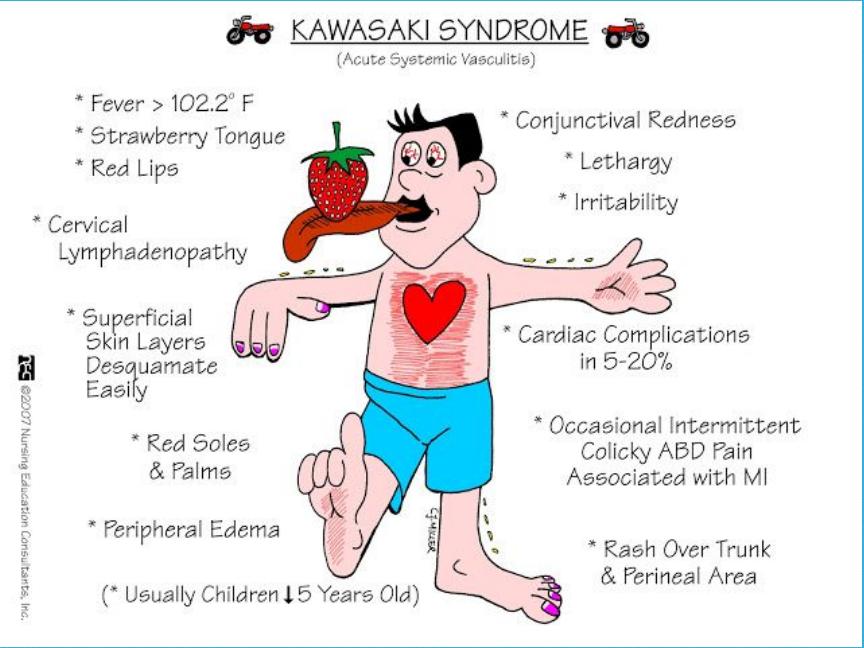
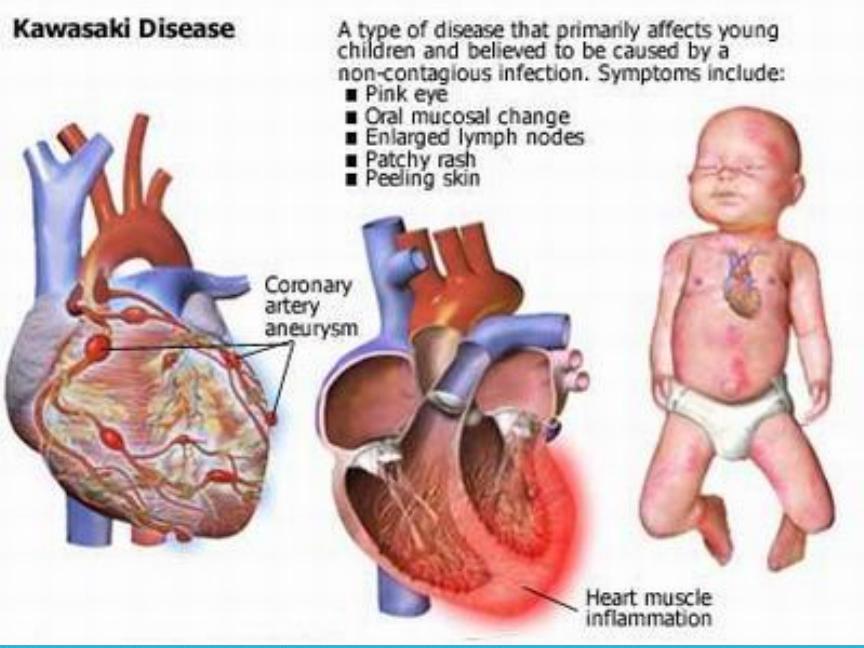
Kawasaki disease
3-
Small vessel
–microscopic polyangiitis ,
wegner’s
granulomatosis
,Churg-Strauss syndrome ,Henoch –
Schonlein purpura ,mixed essential
cryoglobulinaemia
•
Drug induced Vasculitis , antithyroid
drugs,allopurinol ,hydrlazine ,
•
Serum sickness
•
Infection –HBV ,HCV
•
Malignancy
•
Rheumatic diseases –SLE ,RA
•
Endocarditis

•
Constitutional symptoms
–fever ,weight loss ,fatigue
•
Skin
–purpura , liviido reticularis ,digital infarction
•
Musculoskeletal
–arthralgias ,arthritis
•
Pulmonary
–alveolar hemorrhage , pulmonary nodules
•
GIT
–bowl ischemia /infarction
•
Renal
–GN ,nephrotic syndrome ,renovascular
involvement ,hypertension
•
Neurological
–mononeuritis multiplex ,visual
disturbances ,stroke ,lightheadedness
•
CVS
–pulselessness /bruits ,claudication ,aneurysms
•
Lab abnormalities
–anemia ,eosinophilia , elevated acute phase reactant ,renal
insufficiency ,active urinary sediments
•
Tissue biopsy
(skin ,nasal septum ,muscle)
•
Renal biopsy
(RFT/GUE abnormality)
•
Visceral angiography
•
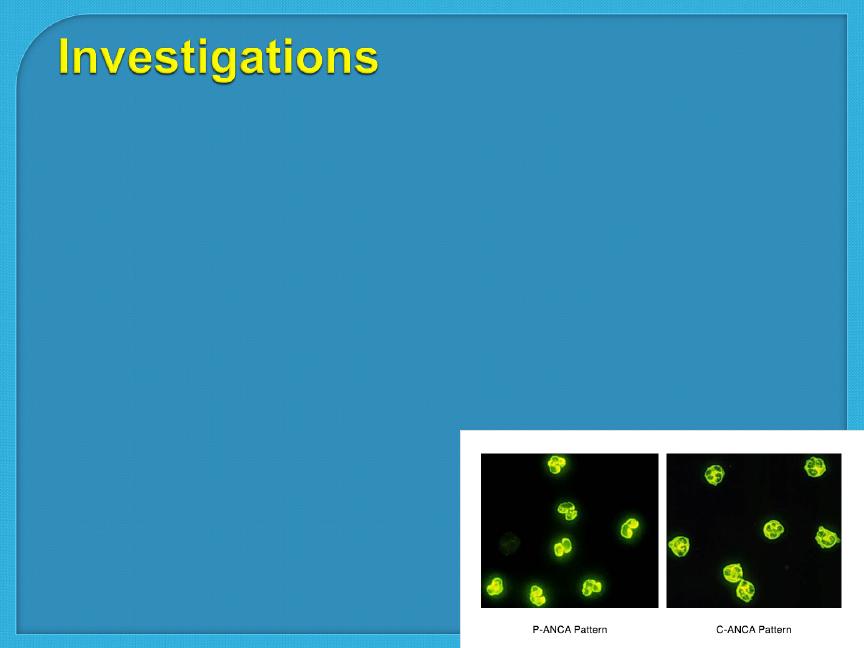
ANCA
: c-ANCA - p-ANCA (Anti-neutrophil cytoplasmic antibody )
•
Which are a group of autoantibodies, mainly of the IgG type,
against antigens in the cytoplasm of neutrophil granulocytes (the most
common type of white blood cell) and monocytes. They are detected as
a blood test in a number of autoimmune disorders, but are particularly
•
associated with systemic vasculitis.
•
•
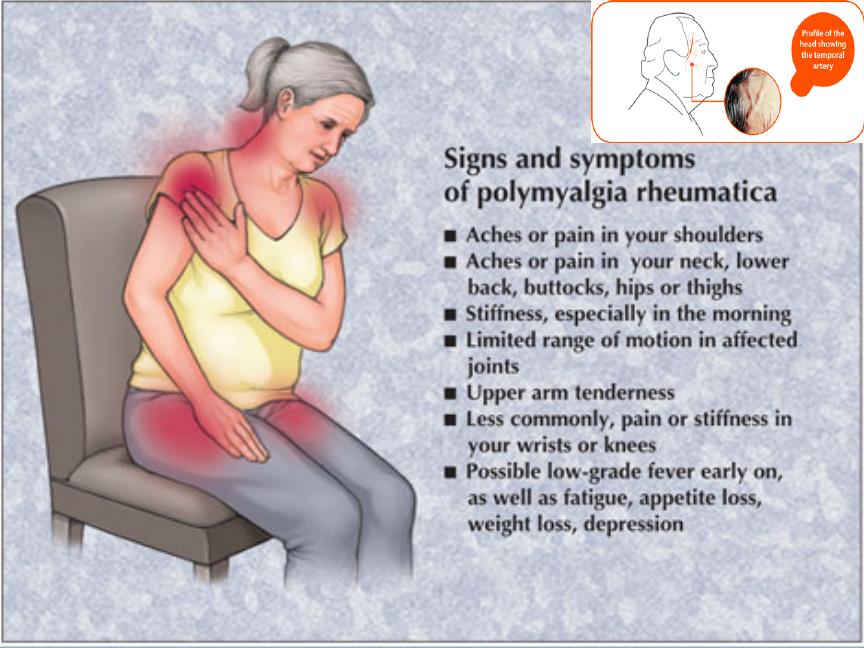
Clinical syndrome of muscle pain and stiffness
and classically ,increased ESR
•
Close association with GCA
•
Prevalence is 20 per 100 000 (over 50)
•
Mean age of onset is 70
•
♀:♂ ratio is 3:1
•
ESR is elevated above 40 mm/hour
•
Normochromic ,normocytic anemia
•
Elevated CRP (prior to ESR)
Oral corticosteroids
•
Prednisolone 15 mg per day
•
Dramatic response within 72 hours
•
12 -18 months treatment
•
Osteoporosis prophylaxis with bisphosphonate

Steroid sparing agents
(methotrexate
,azathioprine)
•
Steroid can not be withdrawn at 2 years
•
Dose greater than 7.5 mg per day
GCA should be treated promptly
•
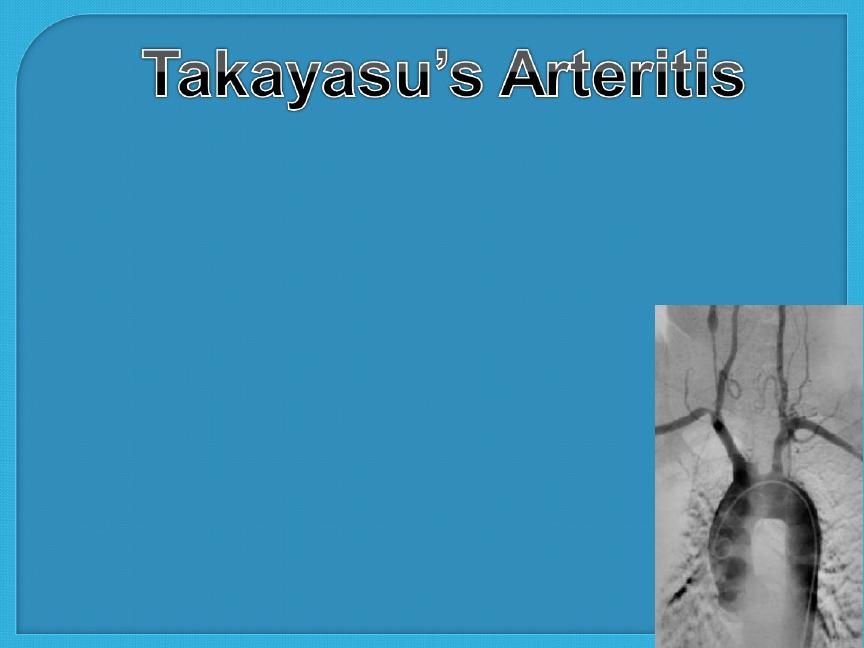
Chronic inflammatory granulomatous panarteritis of
elastic arteries
•
Aorta and its branches , carotid ,ulnar ,brachial ,radial
and axillary arteries are most commonly involved
•
♀:♂ ratio is 8 :1
•
Typical age of onset is 25 -30 years
•
Aetiology is unknown
•
Thickened and inflammed intima
without fibrinoid degeneration

•
Claudication
•
Systemic symptoms
On examination
•
Loss of pulses
•
Hypertension
•
Bruits
•
Aortic incompetance
• type 1: localised to the aorta and its branches
• type 2: localised to the descending thoracic and
abdominal aorta
• type 3: combines features of 1 and 2
• type 4: involves the pulmonary artery.

•
High ESR
•
Normochromic normocytic anemia
•
Angiography – coarctation ,occlusion ,
anuerysmal dilatation
•
High dose oral prednesolone
•
Additional methotrexate or cyclophosphamide is
usually required
•
Reconstructive vascular surgery (avoided during
active inflammation ) benefit hypertension secondary
to aortic or renal lesion
•
5 –year survival rate is 80%
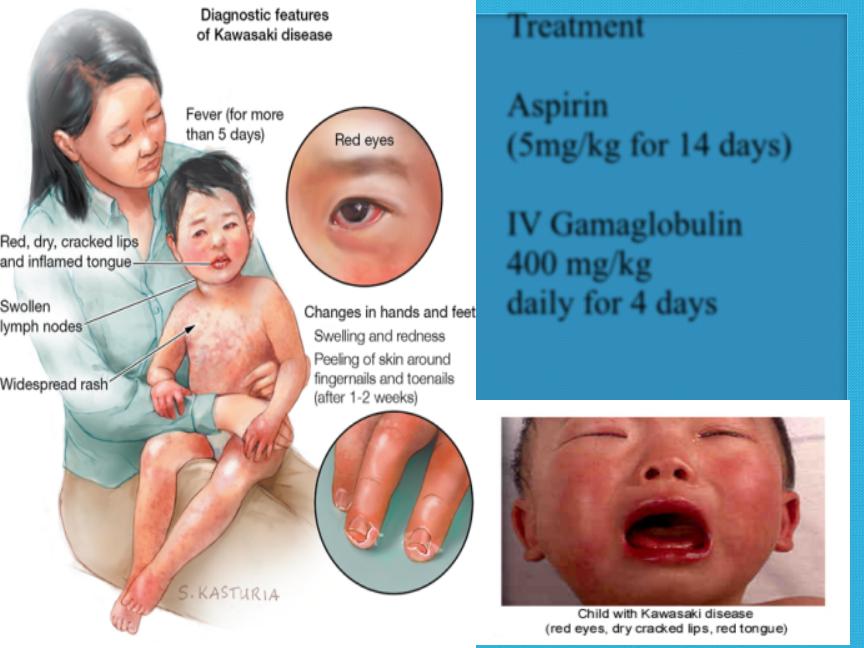
Treatment
Aspirin
(5mg/kg for 14 days)
IV Gamaglobulin
400 mg/kg
daily for 4 days
•
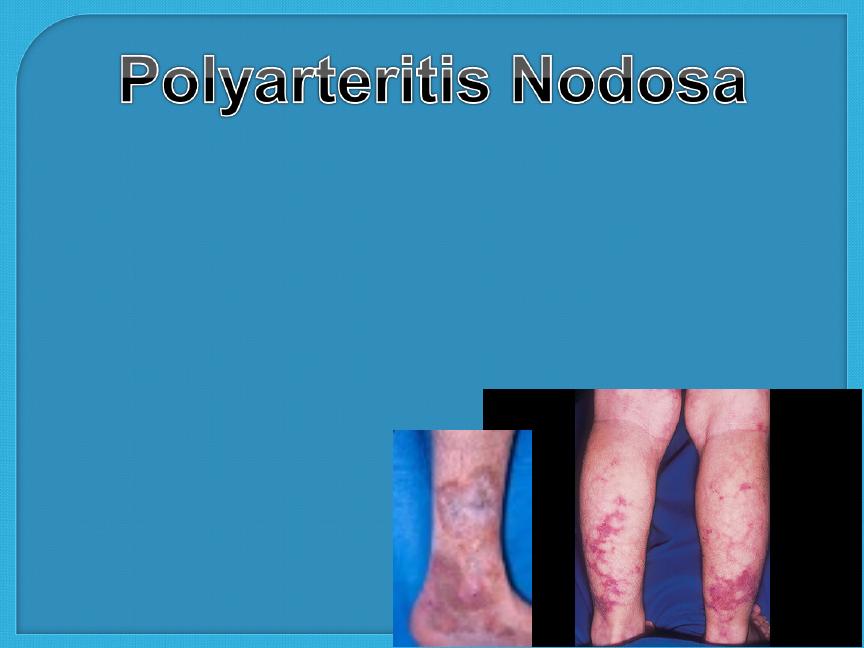
PAN is a necrotising vasculitis characterised by
transmural inflammation of medium sized to small
arteries
•
Annual incidence is 2 per million
•
Peak incidence is 4th and 5th decade
•
♂:♀ ratio is 2:1
•
HBV is a risk factor
•
Myalgia ,arthralgia ,fever and weight loss
•
Skin lesions –palpable purpura ,ulceration ,infarction
and livedo reticularis
•
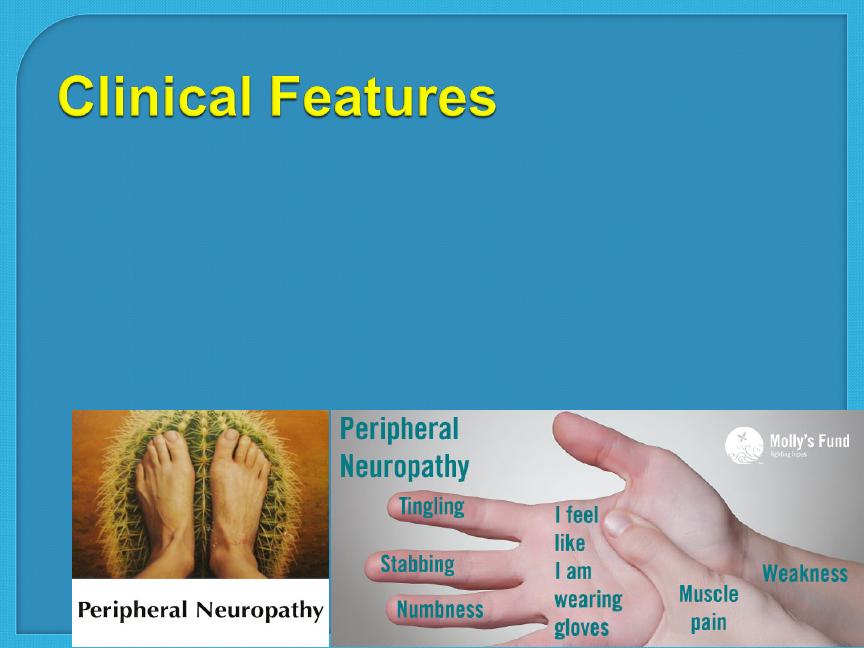
Peripheral neuropathy (70%) –symmetrical ,sensory
and motor
•
Severe hypertension and/ or renal impairment

•
Normochromic normocytic anemia
•
Mild to moderate leukocytosis
•
Moderate to profound thrombocytosis
•
Elevated ESR ,CRP
•
RF ,ANF are negative
•
GUE –hematuria , RBC cast
•
Hepatitis B and C serology
•
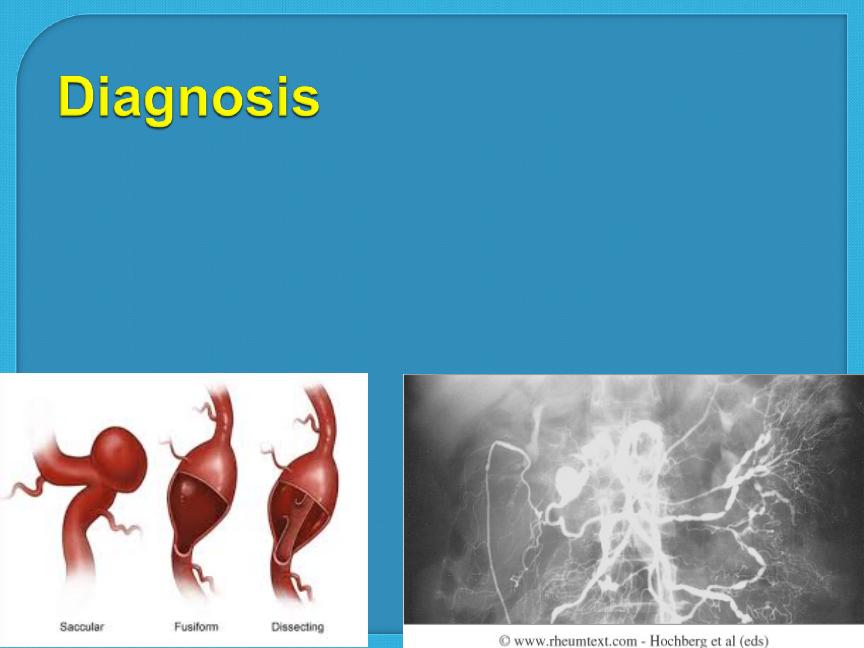
Angiography –multiple anuerysims and smooth
narrowing of mesenteric , hepatic or renal
systems
•
Tissue biopsy (muscle or sural nerve)
•
HBV related disease –antiviral therapy
•
Idiopathic disease –corticosteroids and
cyclophosphamide
•
Mortality < 20%
•
Relapse –up to 50%
•
The annual incidence is 5 -10 per million
•
♂:♀ ratio is 1:1
•
Can be seen at any age (rare before adolescence)
•
Mean age of onset is 40 years
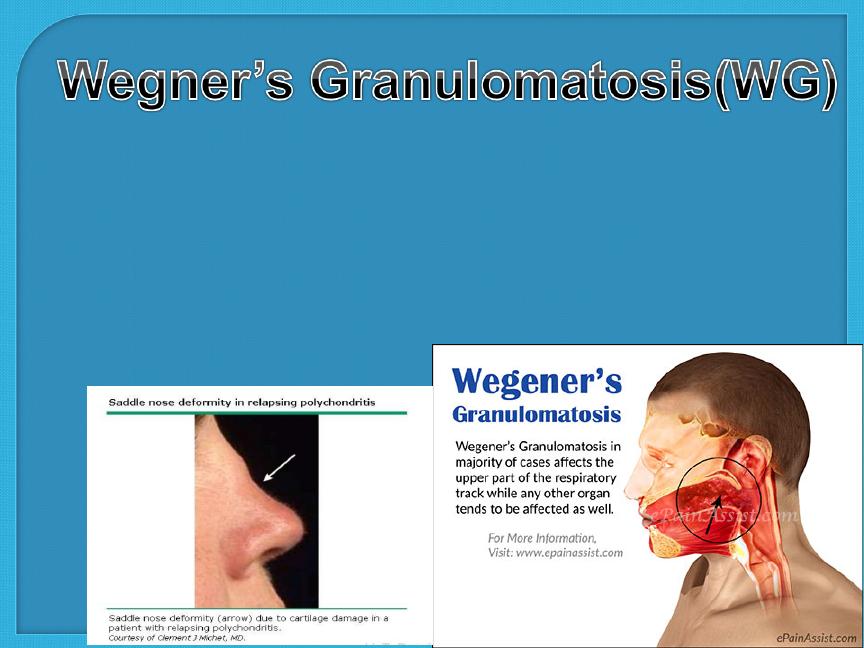
It is a syndrome characterized by:
•
Granulomatous inflammation involving the
respiratory tract
•
Necrotizing vasculitis affecting small to medium sized
vessel
•
Necrotizing GN is common
•
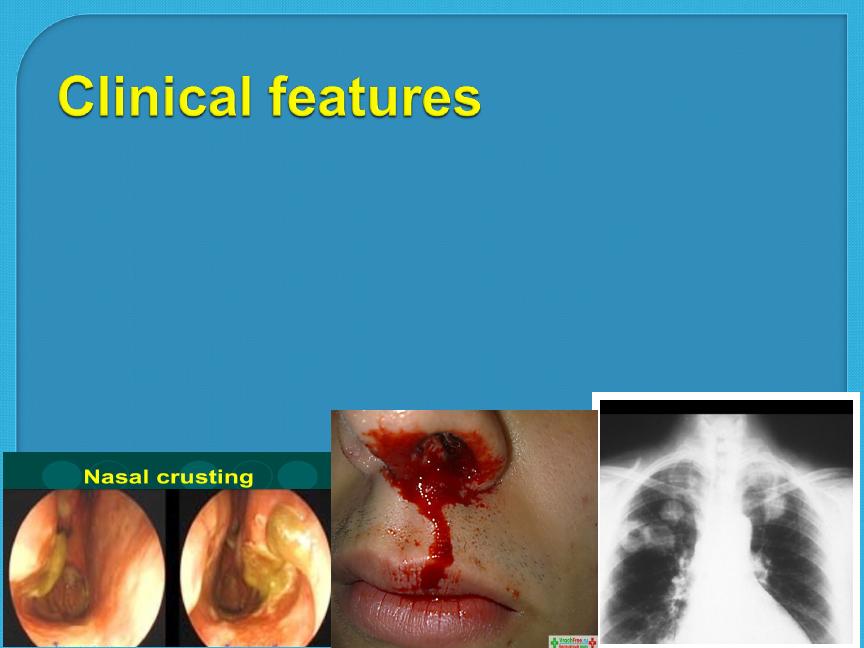
Upper airway involvement (95%) –epistaxis ,nasal crusting
,sinusitis ,nasal mucosal ulceration, nasal septal perforation and
deafness (serous otitis media )
•
Pulmonary involvement(85% -90%) –asymptomatic infiltrate
,cough
•
,hemoptysis ,dyspnea and
•
chest discomfort

•
Eye involvement(52%) –mild conjunctivitis
,episcleritis ,scleritis ,granulomatous
sclerouveitis , cilliary vessel vasculitis
,retroorbital mass lesion (proptosis ,diplopia ,loss
of vision)
•
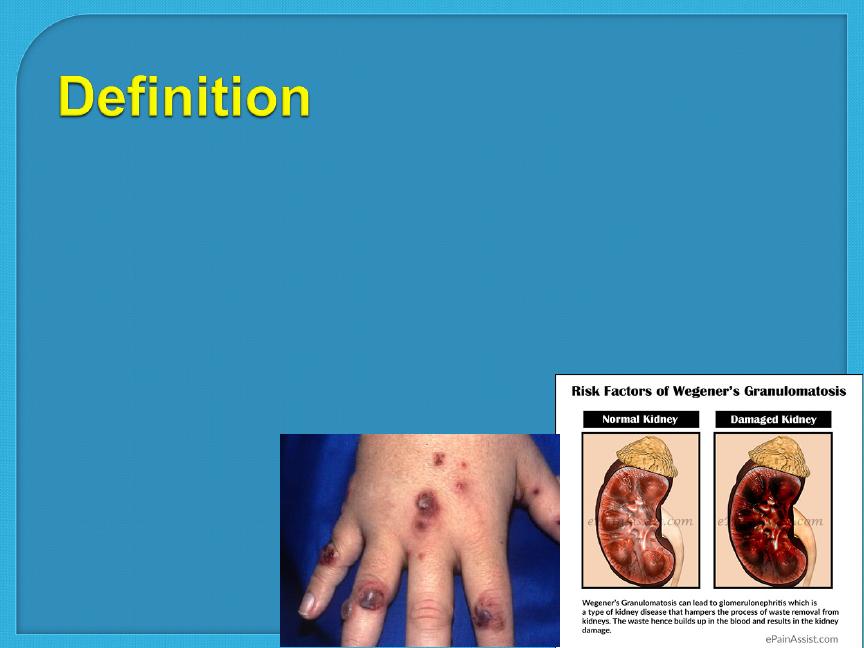
Skin lesion –papule ,vesicle , palpable purpura
,ulcerations or subcutaneous nodules
•
Renal disease (77%) -GN
•
Demonstration of necrotising granulomatous
vasculitis on tissue biopsy in the presence of
compatible clinical features (pulmonary tissue
offer the highest diagnostic yield )
•
When biopsy specimens are non diagnostic,
ANCA assays provide important adjunct to
diagnosis

•
Treatment with
glucocorticoids
is helpful in
stabilizing the acute inflammatory process but
is almost always inadequate. Thus patients are
treated with a combination of glucocorticoids
and immunosuppressive agents, especially
cyclophosphamide, azathioprine, or
methotrexate
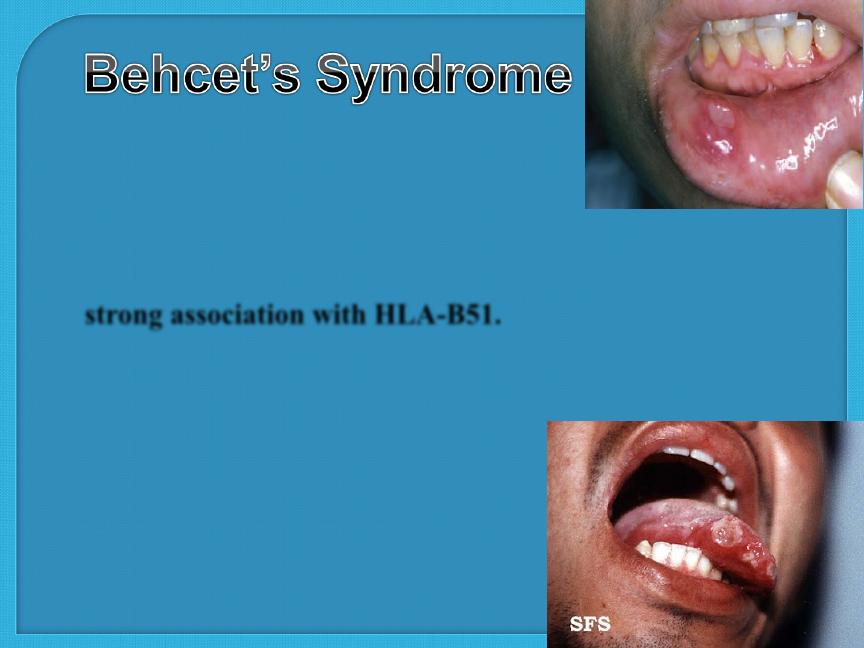
This is a vasculitis of unknown etiology
that characteristically targets small arteries and venules. It is rare in
Western Europe but more common in ‘Silk Route’ countries around
the Mediterranean and Japan, where there
is a
strong association with HLA-B51.
Oral ulcers are universal ,Unlike aphthous
ulcers, they are usually deep and multiple, and last for
10–30 days. Genital ulcers are
also a common problem,
occurring in 60–80% of cases.,

The usual skin lesions are
erythema nodosum or acneiform lesions, but migratory
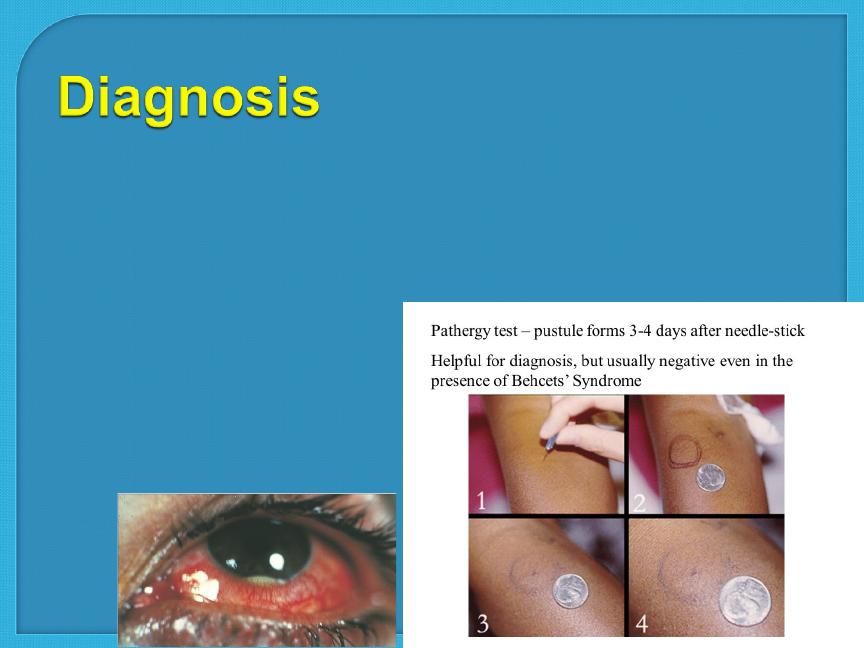
thrombophlebitis and vasculitis also occur. Ocular
involvement is common and may include anterior or
posterior uveitis or retinal vasculitis. Neurological
involvement occurs in 5% and mainly involves the
brainstem, although the meninges, hemispheres and
cord can also be affected, causing pyramidal signs
•
Recurrent oral ulcerations plus 2 of the
followings:
•
Recurrent genital ulceration
•
Eye lesions
•
Skin lesions
•
Pathergy test

•
Recurrent oral ulceration –universal ,usually painful, shallow
or deep with central yellowish necrotic base ,singly or in
croups ,anywhere in the oral cavity ,persist for 1-2 weeks ,no
scar formation.
•
Genital ulceration –less common, more specific ,don’t affect
the glance penis or urethra ,and produce scrotal scars.
•
Skin involvement –folliculitis ,erythema nodosum ,acne-like
exanthem ,and infrequently vasculitis.
•
Leukocytosis
•
Elevated ESR
•
Elevated CRP
•
Autoantibodies may be found

•
Mucous membrane involvement –topical glucocorticoid
(mouth wash or paste)
•
Thalidomide –resistant oral and genital ulceration
•
Colchicine –erythema nodosum and arthralgia
•
Thrombophlebitis –aspirin 325 mg /day
•
Uveitis and CNS-Behcet’s –systemic glucocorticoids and
azathioprin
•
Interferon –very effective for CNS-Behcet’s and refractory
uveitis