Working Length Determination
Dr. Ahmed JawadWorking length- definition
The distance from a coronal reference point to the point at which canal preparation and obturation should terminate.The first step in cleaning and shaping is working length determination.
Significance:
• 1) Determine the instrument length in the canal.• 2) Limits the depth to which the canal filling maybe placed.
• 3) Limits the postoperative pain & discomfort as instrumentation shorter than the apical constriction leaves uncleaned space, while beyond the apical constriction irritate the periapical tissues, violate the apical zone and affect the compaction of the filling material against the apex.
• 4) Determination of the success of treatment.
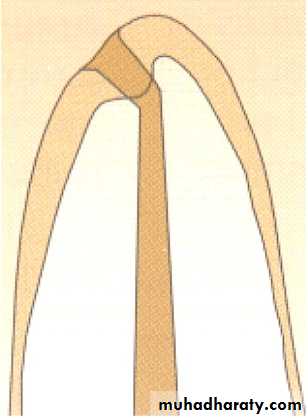
Anatomy of the Apex
1
2
3
Tooth apex (radiographic apex)
Apical foramen (major foramen)
Apical constriction (minor foramen)Distance between 1 and 2:
The apical foramen deviates from the apex in 50-98% of the teeth.This deviation averages 0.3 to 0.6 mm but could be as much as 3 mm.
1
2
3
Tooth apex (radiographic apex)
Apical foramen (major foramen)
Apical constriction (minor foramen)
Distance between 2 and 3:0.5 mm in 18-25 y old, and 0.7 in 55+ y old.
Distance between 1 and 3:
0.89 mm with a range of 0.1 to 2.7 mm.
1
2
3
Tooth apex (radiographic apex)
Apical foramen (major foramen)
Apical constriction (minor foramen)Anatomical Apex & Radiographic Apex
Anatomical apex:
is the tip or the end of the root determined morphologically, which is the natural apical constriction formed by the cemento-dentinal junction (narrowest part in the canal).
Radiographic apex:
is the tip or the end of the root determined radio-graphically.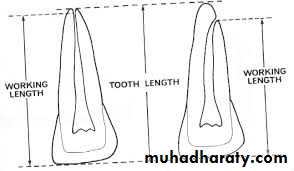
Reference points
It is the site on the occlusal or incisal surface from which measurements are made.This point is used throughout canal preparation & obturation.
The measurement should be made from a secure reference point on the crown, in close proximity to the straight-line path of the instrument, a point that can be identified and monitored accurately.
A definite, repeatable plane of reference to an anatomic land mark on the tooth – necessary.
(usually the incisor edge in anterior teeth , the cusp tip in posterior teeth).

Reference points
• Don’t use weakened enamel walls, temporary filling or diagonal lines of fracture as a reference site for Length of tooth measurement.• Diagonal surfaces should be flattened to give an accurate site of reference.
• Weakened cusps or incisal edges are reduced to a well – supported tooth structure.
Requirements of W.L. Determination
• Knowledge of pulp anatomy and average length of each individual root.• Good, undistorted preoperative radiographs showing the total length and all roots of the involved tooth.
• Strait-line access.
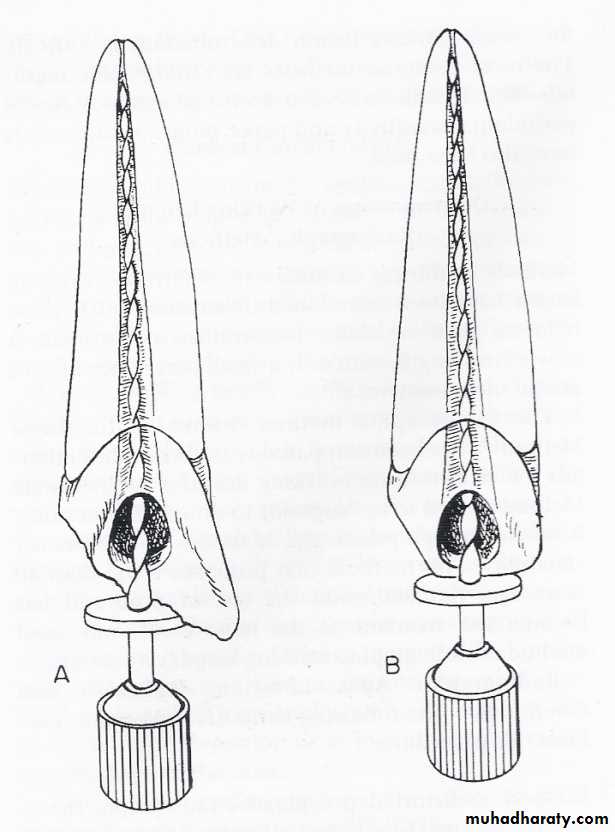
• Small stainless steel K-files facilitate the process and the exploration of the canal.
• A definite, repeatable plane of reference, it should be noted on the patient record.
Techniques of W.L Determination
• Radiographic methods• Digital tactile methods
• Paper point evaluation
• By apical periodontal sensitivity
• Electronic apex locators
1.Radiographic Methods
Preoperative radiographRadiograph of the tooth with endodontic instrument placed to its tentative working length.
Parallel technique is preferable over bisecting technique

