1
Fifth stage
Surgery
Lec-5
د
.
مثنى الحموشي
13/12/2016
Fractures around the elbow in children
Supracondylar fracture of the humerus
It is very common fracture in children , and according to the displacement of the distal
segment the fracture will be of two types :
A- posterior type :it is the commonest type about 95% of the cases , it is occur due to fall on
out stretched hand , the humerus breaks just above the condyles , the distal fragment is
displaced backward .
B- anterior type :it is due to direct blow on the elbow posteriorly ; it is rare
Classification :
Grade one : undisplaced fracture .
Grade two : angulated fracture with the posterior cortex is still in continuity .
Grade three : completely displaced fracture .
Clinically :
History of fall on out stretched hand , the child is in pain , swelling , deformity (which is
s
shape in posterior type) . It is very important to check the distal pulsation (radial pulse) and
capillary refilling to asses the distal circulation , also checking the nerves for any injuries
( mainly the median nerve ) .
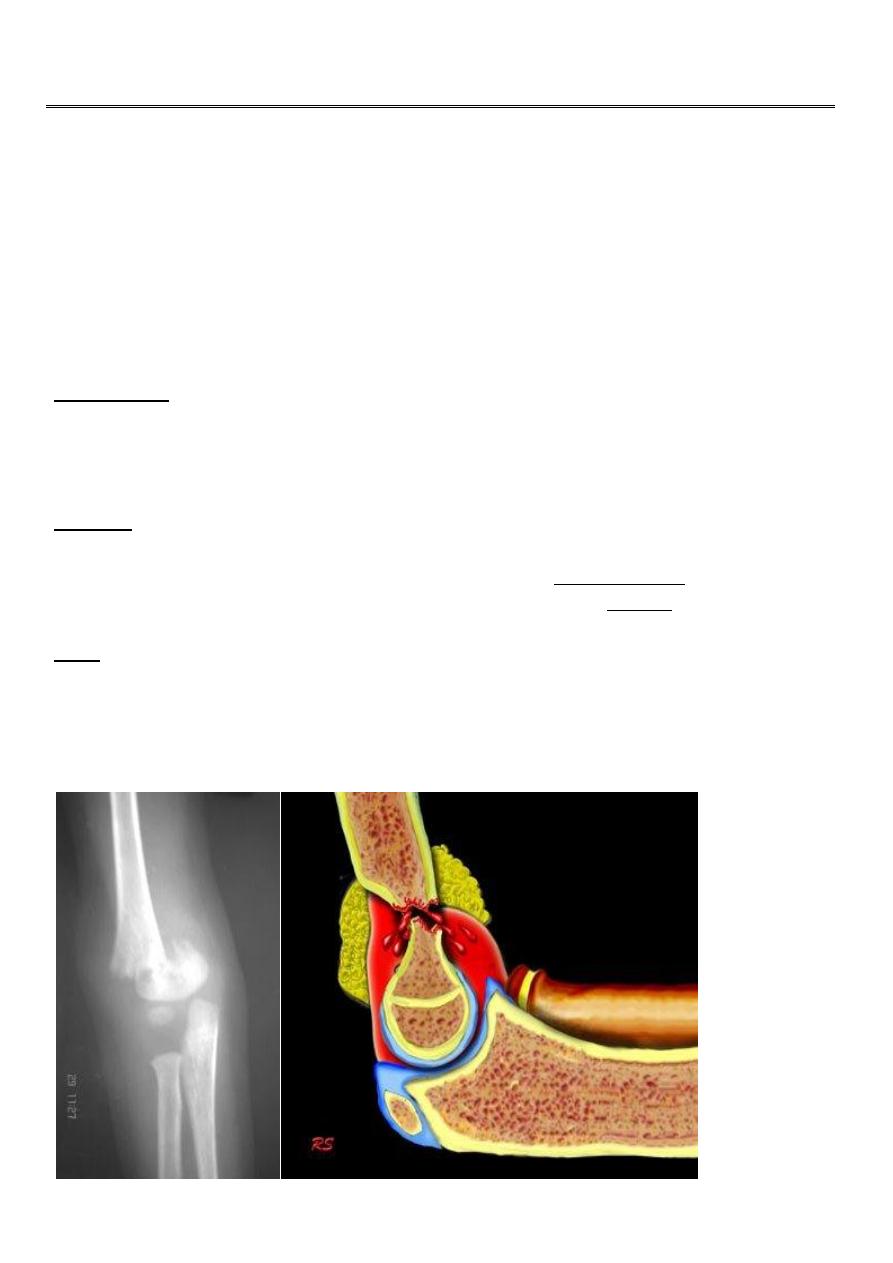
X-ray : the fracture is seen clearly in A-P , and lateral views . In undisplaced fracture the
fat-pad sign which is triangular lucency in front of the distal humerus this will raise the
suspicion of the fracture.
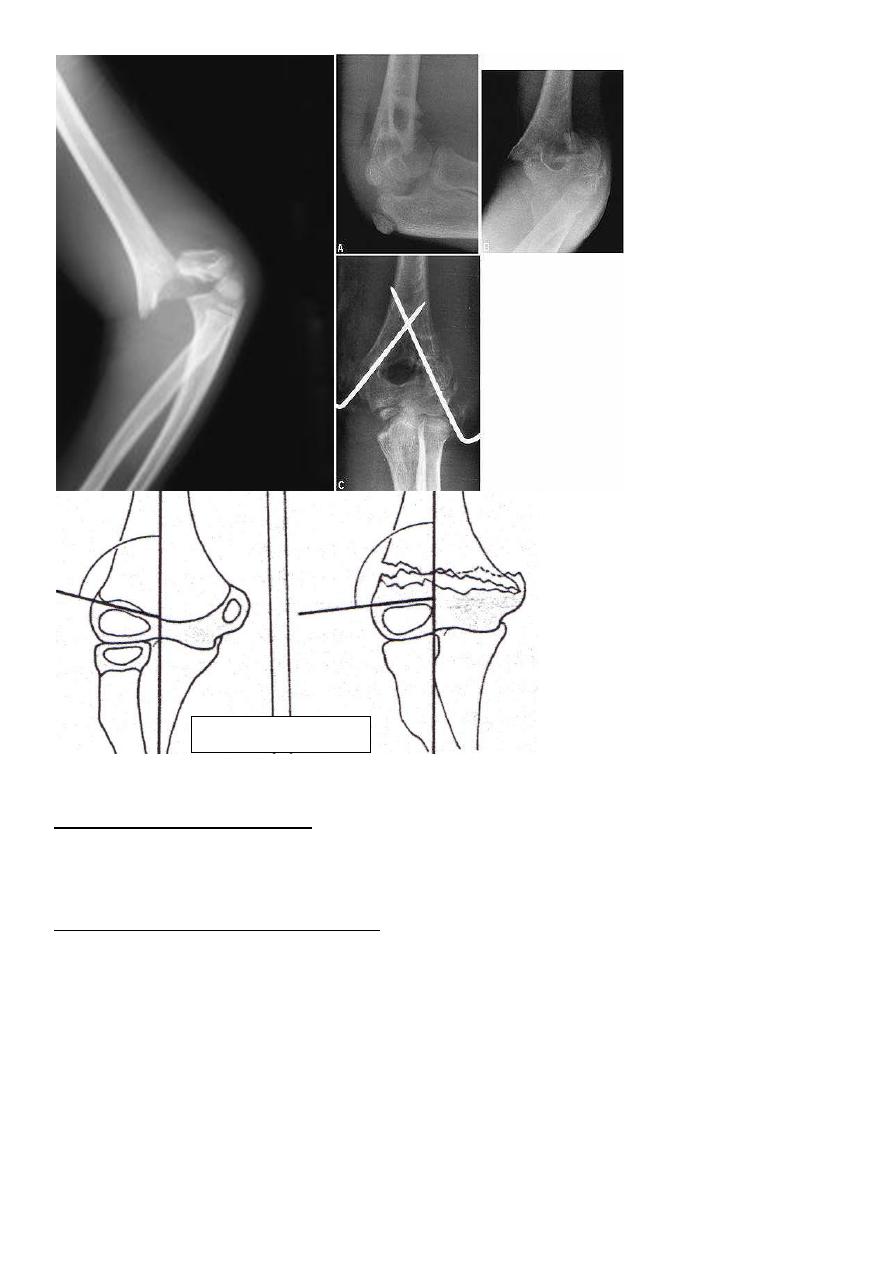
In A-P view we can measure the Boumans’ angle which is helpful in assessing the degree of
angulation of the distal segment normally less than 80`.
2
Treatment
Grade one (undisplaced fract.) : the elbow is immobilized at 90` flexion and neutral rotation
in back slab and hanged by sling , 10-14 days later another x-ray taken to exclude
displacement then full p.o.p is done and it leaved for another 3 weeks .
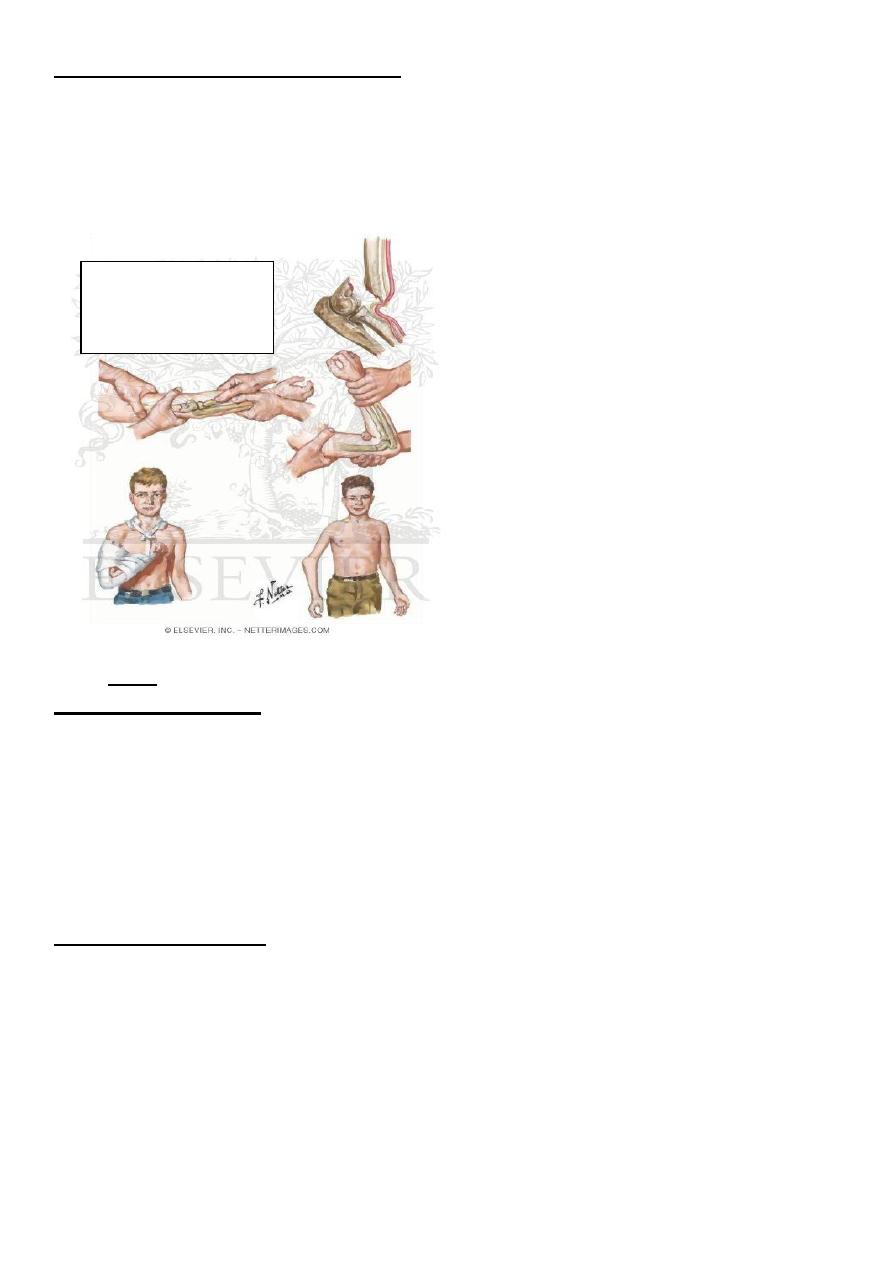
Grade two (posterior angulated fract.) :
Manipulation under anesthesia by doing :
1-contineous traction for 2-3 minute with
counter traction .
2-correction of the side way tilt and rotation .
3- gradual flexion of the elbow to 120`then feel the radial pulsation if ( –ve ) then do
gradual extension tell the pulsation become (+ve) .
Then back slab and x-ray checking ; after 10 days full p.o.p done for another 3 weeks .
If manipulation failed then do open reduction and fixation or percutaneous pining .
Boumann`s angle
3
Grade three (completely displaced fract.) :
Manipulation under anesthesia if fail then do close pining or open reduction and fixation by
k-wires .
Indications of open reduction :
1- closed fracture can not reduced by manipulation .
2-open fracture .
3- associated vascular damage .
Complications
Early :1-vascular damage. 2-nerve damage .
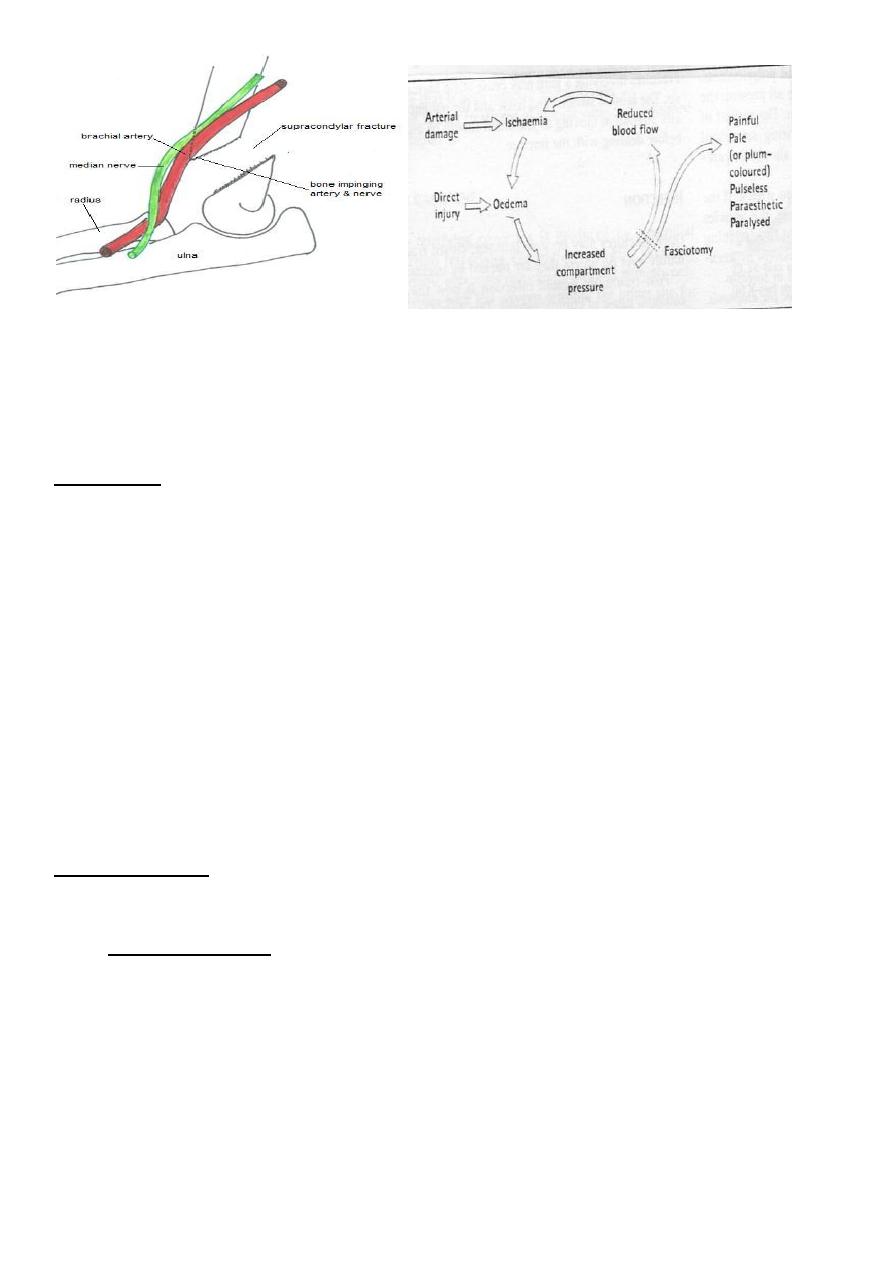
1- vascular damage :
mainly brachial artery;this will lead to ischemia of the forearm
(Volkmann's ischemia ) .
The ischemia also occur in the forearm due to edema in the muscles in close facial space
this called( compartment syndrome) , and this will end after 12 hours or less in necrosis of
nerves and muscles within the compartment .
Nerves are capable of regeneration but muscles once infarcted can never recover and
replaced by inelastic fibrous tissue (Volkmann's ischemic contracture) .
Similar events can happened when use tight p.o.p.
Compartment syndrome :
It is a condition in which there is increase in the pressure within the osteofacial space
leading to ischaemia and swelling of the muscles within the space ,leading to more
decrease in the blood flow in the compartment and if continue more than 12 hours then
ischemia and necrosis of the muscles and nerves will be eventual .
This condition can be caused by : proximal arterial injury , soft tissue bleeding from
fractures and operations , tight dressing and p.o.p .
Most common sites are the forearm and legs .
The manipulation ,
the cubitus varus
deformity
4
Clinical features of volk. Ischemia
The classic features of ischemia are the 5 p:-
1-pain .2- paler .3-pulseless .4-parasthesia .
5-paralysis .
the early symptom are pain and parasthesia.
Examination : the ischemic muscle is highly sensitive to stretching , so when we do
hyperextension of the fingers there will be sever pain and it is the most early sign of
ischemia .
The diagnosis can be confirmed by measuring the intracompartmental pressure by special
catheter introduced into the compartment , if it is more than 40 mm mercury is an
indication of urgent decompression
Also if the patient has 3 of the 5 ps .
Treatment of compartment syndrome :
The compartment should be decompressed by immediate and complete removal of the
cast, the bandages and the dressing ; the limb should be nursed flat with slight elevation
above the level of the heart , and if the pressure above 40 mm Hg then immediate open
fasciotomy should be done and the wound should be left opened .
Also fasciotomy should be done if 3 of the 5 p become +ve
2- nerve injury :
Median nerve can be injured by the fracture ; ulnar and radial nerves can
be injured during the operation .
Late complications :
1- malunion : it is a common complication .
Uncorrected side tilt or angulation and rotation lead to deformity ; mainly varus deformity
called cubitus varus and rarely valgus called cubitus valgus deformity .
Varus deformity is more common , disfiguring and called (gun stock) deformity which is
permanent deformity that is need surgical correction .
Valgus deformity is rare and cause late ulnar nerve palsy .
5
2- elbow stiffness and myositis ossificans :
Elbow is very liable for stiffness after injury ;passive physiotherapy is contraindicated in
elbow stiffness because it make the condition worse and aggravate myositis ossificans . So
it is advised to do active physiotherapy .
Fracture of the lateral epicondyle of the humerus
This fracture occur due to fall on out stretched hands . The fracture piece although it look
small in the x-ray but it in fact is large and it pulled by extensor muscle of the wrist which
attached to it .
In sever cases the piece is rotated by the action of the extensor muscle and become
capsized lead to nonunion later on if not treated .
Clinically :
The elbow swollen and deformed , tenderness at the site of the fracture .
Treatment :
If there is no or minimal displacement we can do back slab above the elbow which is 90`
flexed and the forearm is neutral ; after 7 days repeat the x-ray for checking and full p.o.p.
for 3-4 weeks , followed by active physiotherapy .
Displaced fracture need open reduction and fixation by K-wire or screw .
Complications :
Late complication :
1- malunion . This will lead to recurrent dislocation of the elbow .
2- nonunion .this complication is inevitable if the distal piece is capsized and not treated ;
this will lead to disturbing of the growth at the distal end of the humerus lead to cubitus
valgus and late ulnar nerve palsy .
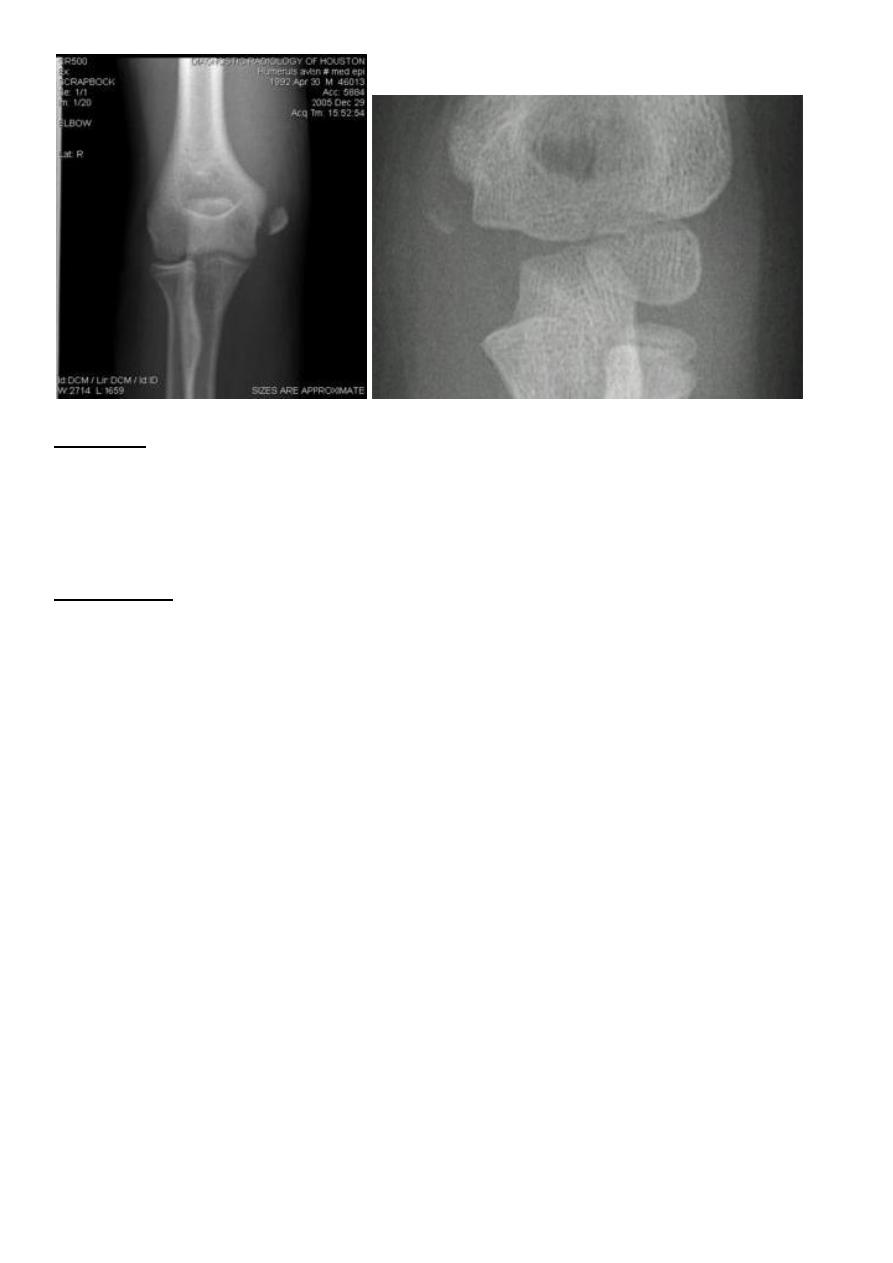
Fracture medial epicondyle of the humerus
It is occur due to fall on out stretched hands ; the medial epicondyl is avulsed by the effect
of the strong flexor muscles of the wrist . If the elbow joint is dislocated or subluxated even
momentarily , the fracture piece may introduced into the joint .
Clinically :
History of trauma , pain and tenderness , swelling , sensation and power of the fingers
should be tested to exclude ulnar nerve damage .
6
Treatment :
Minor displacement less than 5 mm. need only back slab in elbow flexed , after 7 days do
full p.o.p. for 2-3 weeks .
If the piece is trapped into the joint , then it must be freed either by manipulation under
anesthesia , if failed or the piece is severely displaced then we should do open reduction
and fixation by K wire or screw .
Complication : early : ulnar nerve damage .
late : stiffness of the elbow .